Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
36 Cards in this Set
- Front
- Back
|
Define Malignant hyperthermia.
|
a sub clinical myopathy that is unmasked upon exposure to volatile anesthetics or succinylcholine.
|
|
|
What is the significance of chromosomes 1,3,7,17,19?
|
genetic coding site for Ca++ release channels of sarcoplasmic reticulum
|
|
|
Where is the gene for MH located?
|
chromosomes 1,3,7,17 & 19.
|
|
|
Pathophysiology: What are some results of skeletal muscle that acutely increases its 02 consumption & lactate production?
|
Heat production.
Respiratory & metabolic acidosis. Muscle rigidity. Sympathetic stimulation. Increased cellular permeability. |
|
|
What are some possibilities of patients w/ normal Ry1 receptors?
|
Possible abnormalities in 2º messengers & modulators of Ca++ release (Fatty acids & phosphatidylinositol).
Possible abnormal Na+ channels. |
|
|
What is MH caused by?
|
a loss of control of Ca++ concentration w/n the muscle fiber. (Generalized alteration in cellular & sub cellular membrane permeability)
|
|
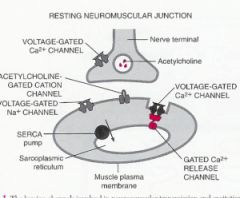
What are the general mechanism of skeletal muscle contraction?
|
Action potential travels along a motor nerve to its endings on muscle fibers, where the nerve secretes neurotransmitter Ach.
|
|
|
How does Ach act on muscle fiber?
|
acts on the area of muscle fiber membrane to open multiple Ach-gated channels through protein molecules floating in the membrane.
|
|
|
What does Calcium initiate in the cell?
|
initiate attractive forces b/n the actin & myosin filaments, causing them to slide alongside each other in a contractile process.
|
|
|
What does opening of the Ach-gated channels in the neuromuscular junction allow?
|
allows Na+ ions to flow to the interior of muscle fiber membrane initiating action potential in muscle fiber.
|
|
|
What does the action potential traveling along the muscle fiber membrane do?
|
causes sarcoplasmic reticulum (SR) to release Ca++ stored w/n the reticulum
|
|
|
What is the genetic coding site for the Ca++ release channels of skeletal muscle sarcoplasmic reticulum?
|
Rγ1 receptor
|
|
|
What can having a defect in the Ry1 receptor lead to?
|
A defect in this receptor affects Ca++ release channels allowing an increased flood in Ca++ & results in MH susceptibility.
|
|
|
What does Dantrolene do?
|
It is thought that Dantrolene interferes w/ the Ca++ release by binding at the Rγ1 receptor & Ca channel sites.
|
|
|
What is the incidents of MH in children? Adults?
|
1 in 12,000-15,000
1 in 40,000 |
|
|
Where are higher incidents of MH seen?
|
Mid-west (USA).
Children & young adults. Operations such as Orthopedic (joint dislocation repair), Ophthalmic (ptosis & strabismus), Head & neck (cleft palate, T&A, dental). Duchenne muscular dystrophy. (also observed in Burkitt’s lymphoma, Osteogenesis imperfecta, Myotonia congenita, Neuroleptic malignant syndrome, Myelomeningocele. |
|
|
What are some signs & symptoms of MH?
|
Any characteristics of hypermetabolism. (Tachycardia, Tachypnea, Hypercarbia, Arterial hypoxemia, Metabolic or Respiratory Acidosis, Hyperkalemia, Cardiac dysrhythmias, Hypotension, Skeletal muscle rigidity after SCh, Hyperthermia, Mottled skin)
|
|
|
What is the FIRST indication that an individual is susceptible when there is an absence of history?
|
an exaggerated response to SCh
|
|
|
What may be seen in early responses that may indicate MH?
|
increased tension of masseter muscles (more pronounced in kids).
May be impossible to open mouth for intubation. |
|
|
What is Trismus-Masseter Spasm?
|
Defined as jaw muscle rigidity in association w/ limb muscle flaccidity after giving SCh.
Jaw muscle tone: exaggerated, prolonged & tight, “jaws of steel”, risk increases greatly. |
|
|
What should you do once trismus appears?
|
Check ETC02, urine color & arterial or venous blood for CK, acidosis, electrolytes (especially K+).
With “jaws of steel” that persist for more than a few minutes, halt procedure. |
|
|
If jaw is slightly resistant to opening, what should you do?
|
Continue & observe carefully.
If jaw is modestly tight, either halt procedure or continue w/ nontriggering agents. |
|
|
What are some early signs of MH?
|
Hypercarbia.
Hyperkalemia (but resolves rapidly after normothermia). |
|
|
What is the most common cause of death in MH patients?
|
V-Fib.
|
|
|
What are some things you may see in ABGs or venous blood work in MH patients?
|
Arterial hypoxemia.
Hypercarbia (PaCO2 100-200 mmHg). Respiratory-metabolic acidosis (pH 7.15-6.80). Marked central venous 02 desaturation. |
|
|
What are some late signs & symptoms of MH?
|
Elevated Temperature.
Rhabdomyolysis. Elevated Transaminase enzymes & CK. (12-24hrs post) DIC. Pulmonary edema. ARF. CNS may manifest blindness, seizures, coma or paralysis. |
|
|
What are the treatment doses of Dantrolene?
|
(2-3 mg/kg) IV as bolus, & repeat dose q 5-10 min until symptoms are controlled (up to or > 10 mg/kg)
|
|
|
What other steps should you do if MH is identified?
|
Turn off volatile gases.
Hyperventilate w/ 100% 02. Initiate active cooling measures (stop when temp is 38ºC). Conclude surgery ASAP. Correct metabolic acidosis (NaHC03 1-2 mEq/kg IV). Maintain UOP w/ hydration, mannitol 0.25 g/kg, lasix 1 mg/kg IV. Treat cardiac dysrhythmias. Consider treating hyperkalemia if not decreased w/ normothermia (glucose 50 ml of D50 & 10 units regular insulin).Monitor in ICU for reoccurring. |
|
|
When was Dantrolene approved for use by the FDA? What is its effectiveness? Cost?
|
FDA approved in 1979.
73% show twitch depression w/ 2.5 mg/kg. Expensive therapy ($60-100 per vial). |
|
|
What are some things that may mimic MH?
|
Contrast dye.
Diabetic coma. Drug toxicity-overdose. Heat stroke. Anesthesia machine malfunction w/ increased C02. Thyroid storm. Intracranial free blood. Pheochromocytoma. Sepsis. |
|
|
What are some prophylaxic Dantrolene uses & considerations?
|
One protocol, 2.4 mg/kg IV over 10-30 min prior to induction.
50% of this dose repeated in 6 hrs. Should have foley catheter in place. May cause nausea, diarrhea, blurred vision & weakness. |
|
|
What are some triggering agents of MH?
|
Volatile gases (Halothane, Enflurane, Isoflurane, Sevoflurane, Desflurane).
N20 (may be weak trigger). Succinylcholine. |
|
|
What are some safe agents to administer in a patient w/ suspected MH?
|
Barbiturates, propofol, etomidate, opioids, benzodiazepines, ketamine, nondepolarizing muscle relaxants.
N20 questionable, if in doubt, do not use. Muscle relaxant antagonists. Local anesthetics. Vasopressors. |
|
|
What are some precautions, in regards to MH, you should take w/ the anesthesia machine?
|
Disposable circuit & new fresh gas outlet hose.
New C02 absorbent. No vaporizers (removed or taped off). Continuous flow of 02 at 10L/min for 5-20 minutes. Regional anesthesia if possible. |
|
|
Regarding MH, what are some things you can do before a surgical procedure?
|
Careful evaluation of history.
Genealogy should go back several generations. Patient can undergo muscle biopsy contracture study. (costly, false positives & only 30 centers, painful) |
|
|
What are some resources available if your patient experiences MH.
|
The Malignant Hyperthermia Association of the United States (MHAUS) 1-800-644-9737.
24 hour hotline 1-800-MH-HYPER. Web www.mhaus.org |