Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
97 Cards in this Set
- Front
- Back
|
the cause of most cases of severe disease and most deaths, predominates in Africa, New Guinea, and Hispaniola
|
P. falciparum
|
|
|
is more common in Central America
|
P. vivax
|
|
|
both are equally prevalent in South America, the Indian subcontinent, eastern Asia, and Oceania.
|
P. falciparum and P. vivax
|
|
|
is unusual outside of Africa, where it makes up ~1% of isolates.
|
P. ovale
|
|
|
is found in most areas (especially throughout sub-Saharan Africa) but is less common
|
P. malariae
|
|
|
(the monkey parasite) can reliably be identified only by molecular techniques and is present in Borneo and Southeast Asia.
|
P. knowlesi
|
|
|
Malaria is the most important parasitic disease in humans, causing about ____ deaths each year.
|
1 million
|
|
|
After introduction of ____ into the bloodstream by female anopheline mosquitoes, the parasite travels to the liver.
|
sporozoites
|
|
|
After introduction of sporozoites into the bloodstream by female anopheline mosquitoes, the parasite travels to the liver and reproduces to form _____ that infect the RBCs.
|
merozoites
|
|
|
The merozoites transform into ______, feed on intracellular proteins (principally hemoglobin), multiply 6-20 fold every 48-72 h, and cause the RBCs to rupture
|
trophozoites
|
|
|
Some parasites develop into long-lived sexual forms called ___, which can be taken up by another female anopheline mosquito allowing transmission
|
gametocytes
|
|
|
in P vivax or P ovale infection, dormant forms called _____ remain in liver cells and may cause disease 3 weeks to more than 1 year later
|
hypnozoites
|
|
|
RBCs infected with P falciparum may exhibit ______ (attachment to venular and capillary endothelium), ______ (adherence to uninfected RBCs), and agglutination (adherence to other infected RBCs)
|
cytoadherence, rosetting
|
|
|
adherence to uninfected RBCs
|
rosetting
|
|
|
adherence to other infected RBCs
|
agglutination
|
|
|
Cytoadherence, rosetting and agglutination causes sequestration of P. falciparum in vital organs, with consequent underestimation of ____ numbers in the body
|
parasite
|
|
|
_____ is central to the pathogenesis of falciparum malaria but is not evident in the other three "benign" forms
|
Sequestration
|
|
|
In ______ individuals, infection triggers nonspecific host defense mechanisms such as increased splenic filtration
|
nonimmune
|
|
|
with repeated exposure to malaria, patients develop ____ to high-level _______ and disease but not to infection
|
resistance, parasitemia
|
|
|
______ (eg sickle cell disease, ovalocytosis, thalassemia) and G6PD deficiency are more common in endemic areas and protect death from malaria.
|
Hemoglobinopathies
|
|
|
Pts initially develop nonspecific symptoms (e.g., headache, fatigue, myalgias) that are followed by _____
|
fever
|
|
|
Febrile paroxysms at regular intervals are unusual and suggest infection with _____ or ______.
|
P vivax or P ovale
|
|
|
The diagnosis of severe falciparum malria requires more than one or one of the following:
|
impaired consciousness/coma, severe normocytic anemia, renal failure, pulmonary edema, ARDS, circulatory shock, DIC, spontaneous bleeding, acidosis, hemoglobinuria, jaundice, repeated generalized convulsions, and a parasitemia level of more than 5%
|
|
|
_____ malaria manifests as diffuse symmetric encephalopathy, typically without focal neurologic signs
|
Cerebral
|
|
|
_____ is an ominous sign associated with mortality rates of ~20%
|
Coma
|
|
|
______ women have unusuall severe illness.
|
Pregnant women.
|
|
|
Premature labor, fetal distress, stillbirth and delivery of low-birth-weight infants are common.
|
Pregnant women
|
|
|
_______ (hyperreactive malarial splenomegaly) may result as a chronic complication of malaria and is characterized by massive splenomegaly, hepatomegaly, and an abnormal immunologic response to infection.
|
Tropical splenomegaly
|
|
|
Although antibody-based diagnostic tests are being used with increasing frequency, demonstration of ______ forms of the parasite on __________ is required for diagnosis.
|
asexual; peripheral blood smears
|
|
|
______ and the less sensitive thin smears detect parasitemia levels as low as 0.001% and ~0.05%, respectively
|
Thick
|
|
|
If the level of clinical suspicion is high and smears are initially negative, they should be repeated _________ for 2 days.
|
every 12-24 hours
|
|
|
Other laboratory findings generally include ______,______ anemia; elevated ________ markers, and thrombocytopenia.
|
normochromic, normocytic and inflammatory
|
|
|
Treatment for uncomplicated malaria
|
chloroquine-sensitive strains of P vivax, P malariae, P ovale, P knowlesi, P falciparum - the treatment is Chloroquine (10mg of base/kg stat followed by 5mg/kg at 12, 24, and 36 h or by 10 mg/kg at 24 h and 5 mg/kg at 48 hours) OR
Amodiaquine (10-12 mg of base/kg qd for 3 days) |
|
|
Radical treatment for P vivax or P ovale infection
|
chloroquine , amodiaquine,
primaquine should be given (0.5mg of base/kg qd) for 14 days to prevent relapse. In mild G6PD deficiency, 0.75,g of base /kg should be given once weekly for 6-8 weeks. |
|
|
This drug should NOT be given in severe G6PD deficiency
|
Primaquine
|
|
|
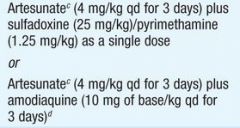
Treatment for sensitive P. falciparum malaria
|
|
|
|
Treatment for multidrug-resistant P falciparum malaria
|
Either artemether-lumefantrine (1.5/9 mg/kg bid for 3 days with food) or Artesunate (4 mg/kg qd for 3 days) PLUS mefloquine (25 mg of base/kg - either 8 mg/kg qd for 3 days or 15 mg/kg on day 2 and then 10 mg/kg on day 3)
|
|
|
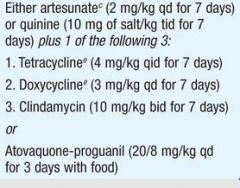
Second-line treatment/treatment of imported malaria
|
|
|
|
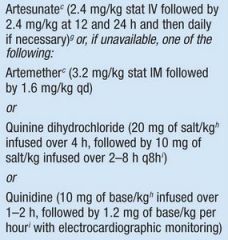
Treatment for severe falciparum malaria
|
|
|
|
Pts receiving _______ should undergo cardiac monitoring;
|
quinidine
|
|
|
Pts receiving quinidine should undergo cardiac monitoring; a total plasma level of more than 8ug/mL, increased QT intervals, or QRS widening by more than 25% is an indication for _____ the infusion rate.
|
slowing
|
|
|
______ is the drug of choice when available.
|
Artesunate
|
|
|
The WHO now recommends artemisinin combination regiments as first line therapy for _______ malaria in all tropical countries and advocates use of fixed-dose combinations.
|
falciparum
|
|
|
_____ and ____ should NOT be given to pregnant women or to children below 8 years of age.
|
Tetracycline ; doxycycline
|
|
|
Infusion rates for _____ and ______ should be carefully controlled.
|
quinine, quinidine
|
|
|
All pts with severe malaria should receive a continuous infusion of _____.
|
dextrose
|
|
|
Unconscious pts should have blood glucose levels measured every _____ hours
|
4-6
|
|
|
Parasite counts and hematocrits for pts with severe malria and pts with uncomplicated disease should be measured every ______ and ____ respectively.
|
6-12, 24
|
|
|
_______ (0.5 mg of base/kg for 14 days) eradicates persistent liver stages and prevents relapse in P vivas or P ovale infection. G6PD deficiency must be ruled out before treatment.
|
Primaquine
|
|
|
Peak feeding times
|
dusk and dawn
|
|
|
____ is the only drug advised for pregnant women traveling to areas with drug-resistant malaria and is generally safe in the 2-3 trimesters.
|
Mefloquine
|
|
|
Atovaquone/ proguanil (Malarone)
|
|
|
____ is contraindicated in persons with severe renal impairment. And should be taken with food or a milky drink.
|
Atovaquone/proguanil
|
|
|
_____ may exacerbate psoriasis.
|
Chloroquine phosphate
|
|
|
Chloroquine phosphate
|
|
|
Doxycycline
|
|
|
____ is contraindicated for children less than 8 years of age and for pregnant women.
|
Doxycycline
|
|
|
Hydroxychloroquine sulfate
|
|
|
Mefloquine
|
|
|
____ may exacerbate psoriasis
|
Hydroxychloroquine
|
|
|
Contraindicated in persons allergic to this drug or related compounds (eg quinine and quinidine) and in persons with active or recent depression, generalized anxiety disorder , psychosis, schizophrenia, other major psychiatric disorders or seizures.
|
Mefloquine
|
|
|
Use with caution in persons with psychiatric disturbances or a history of depression
|
Mefloquine
|
|
|
_____ is not recommended for persons with cardiac conduction abnormalities
|
Mefloquine
|
|
|
_________ is contraindicated in persons with G6PD deficiency.
|
Primaquine
|
|
|
_____ is also contraindicated during pregnancy and in lactation unless the infant being breast fed has documented normal G6PD level.
|
Primaquine
|
|
|
This therapy is indicated for persons who have had prolonged exposure to P vivax and/or P ovale. It is contraindicated in persons with G6PD deficiency as well as during pregnancy and in lactation unless the infant being breast-fed has a documented normal G6PD level.
|
Primaquine
|
|
|
primaquine
|
|
|
The process of reproduction of sporozoites in the hepatocytes of humans leading to production of merozoites.
|
Merogony/Schizogony
|
|
|
The dormant forms of P. vivax and P. ovale which cause relapse in people who are infected with these malarial species.
|
Hypnozoites
|
|
|
The arthropod host of plasmodium species.
|
Anopheles sp.
|
|
|
Aside from cytoadherence and agglutination, which other process plays a role in the sequestration of RBCs with mature P. falciparum parasites in the human vital organs?
|
Rosetting
|
|
|
Aside from failure of hepatic gluconeogenesis, what other mechanism is responsible for the hypoglycaemia seen in malaria?
|
Increased glucose consumption
|
|
|
Type of smear used in performing parasite count.
|
Thick blood smear
|
|
|
Type of smear used in identifying the malarial parasite species.
|
Thin blood smear
|
|
|
The drug of choice for severe falciparum malaria.
|
Artesunate
|
|
|
In patients with P. ovale or P. vivax, which agents address the hepatic stage of the parasite thereby preventing relapse?
|
Primaquine
|
|
|
The only antimalarial drug that can be given to a pregnant patient.
|
Mefloquine
|
|
|
Hepatic form of P. ovale and p. vivax
responsible for relapse. |
HYPNOZOITES
|
|
|
Give 1 principal Determinant of malarial
transmissibility: |
NUMBER/ DENSITY, HUMANBITING
HABITS, LONGEVITY OF ANOPHELINE MOSQUITO |
|
|
Sequestration of RBC with malarial parasite can
occur in all plasmodium species: |
False
|
|
|
Signs of severe malaria:
|
CEREBRAL MALARIA,
ACIDOSIS, RENAL FAILURE, ARDS/ PULMONARY FAILURE, SEIZURES OR CONVULSIONS, IMPAIRED CONSCIOUSNESS |
|
|
Tetracycline used in combination with
antimalarial. |
Doxycycline
|
|
|
DOC for radical cure of malaria.
|
Primaquine
|
|
|
What is the infective form of Plasmodium species to humans from the mosquitos
|
Sporozoites
|
|
|
What Plasmodium species causes relapse of malaria
|
P. vivax (in Philippines), P. ovale
|
|
|
For public health reason, what is the primary rationale why primaquine (which we actually for relapse), why do we give primaquine to patients with Plasmodium falciparum malaria
|
To eradicate gametocytes and to stop transmission from man to mosquito
|
|
|
In terms of proper clinical management, why primaquine is not given to patients with transfusion related malaria
|
No hypnozoites and no gametocytes in transmission-related malaria; No liver stage, no extraerythrocytic/ pre-erythrocytic cycle
|
|
|
What antimalarial drug causes worsening of hypoglycemia in severe malaria
|
Quinine or Quinidine
|
|
|
Complete name of the vector that transmits malaria:
|
female Anopheles minimus flavirostris mosquito
|
|
|
stage in the life cycle of plasmodium that is infective to
man |
sporozoite
|
|
|
Antibodies attach to __ to block cytoadherence
|
infected RBC or parasite antigen
|
|
|
Disease produced by this mode of transmission of
malaria does not have a pre-erythrocytic stage of development |
transfusion
|
|
|
Why does falciparum malaria have very high
parasitemia? |
Because it attacks all ages of RBC
|
|
|
Lab test that determines prognosis
|
thin blood smear
|
|
|
Drug for radical cure
|
primaquine
|
|
|
Drug that can produce a neuropsychiatric rxn
|
Mefloquine
|
|
|
yes/no: chemoprophylaxis for malaria is 100% effective
|
NO
|