Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
101 Cards in this Set
- Front
- Back
|
SKELETAL MUSCLE ACTION POTENTIAL
- resting potential? - peak potential upon depolarization? - duration of 1 AP? |
-85 mV
+30 mV 2.5 ms |
|
|
SKELETAL MUSCLE ACTION POTENTIAL
- describe the graphic description of a single AP |
- resting potential @ -85 mV
- rapid upstroke - peak potential @ +30 mV - rapid downstroke back to resting potential - duration is 2.5 ms |
|
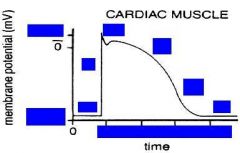
AP graph of Cardiac Muscle
|
|
|
|
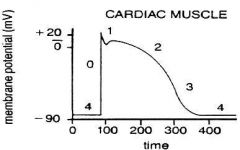
CARDIAC MUSCLE ACTION POTENTIAL
- resting potential? - phase # at the resting potential? - how many phases total? - depolarization peaks @ what mV? - duration of 1 AP? |
-90 mV to -85mV
- Phase 4 @ resting potential - Total of 5 phases (4, 0, 1, 2, 3) - (+20mV) - 400 ms |
|
|
SKELETAL AP vs. CARDIAC AP
- major differences? x3 |
- Skeletal is Biphasic
- Skeletal lacks phase 1 & 2 - Skeletal has very short duration |
|
|
CARDIAC AP
- Transmembrane potential exists due to? |
- Separation of Positive & Negative charges @ the membrane
|
|
|
CARDIAC AP
Describe: - Phase 0 - Phase 1 - Phase 2 - Phase 3 - Phase 4 |
- Upstroke
- Partial Repolarization (Overshoot) - Plateau - Repolarization - Resting Potential |
|
|
TEMPORAL RELATIONSHIP BTW
TENSION DEVELOPMENT & MEMBRANE POTENTIAL CHANGE - what PREcedes contraction? |
- Rapid Depolarization
|
|
|
TEMPORAL RELATIONSHIP BTW
TENSION DEVELOPMENT & MEMBRANE POTENTIAL CHANGE - completion of repolarization coincides with? |
- Peak Tension Development
|
|
|
TEMPORAL RELATIONSHIP BTW
TENSION DEVELOPMENT & MEMBRANE POTENTIAL CHANGE - Duration of AP parallels what? |
- Duration of contraction
|
|
|
TEMPORAL RELATIONSHIP BTW
TENSION DEVELOPMENT & MEMBRANE POTENTIAL CHANGE - reason for difference btw muscle twitch & AP is due to? |
- Excitation-Contraction Coupling
|
|
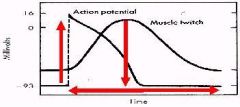
Temporal Relationship BTW
Tension Development & Changes in Membrane Potential |
UP ARROW
- Rapid Depolarization PRECEDES the Peak of Contraction DOWN ARROW - Completion of Repolarization COINCIDES with Peak Tension Development HORIZONTAL ARROWS - Duration of contraction PARALLELS the Duration of AP |
|
|
CARDIAC AP
- what are the 2 type of Cardiac AP's? |
- Fast Response
- Slow Response |
|
|
CARDIAC AP
- Fast response AP involves what anatomical structures? x3 |
- Atrial Myocytes
- Ventricular Myocytes - Purkinje Fibers |
|
|
CARDIAC AP
- Slow response AP involves what anatomical structures? x2 |
- SA node
- AV node |
|
|
CARDIAC AP
- major differences btw Fast response AP vs. Slow response AP |
(UREA)
During Fast Response - Upstroke Slope is greater - Resting Vm more negative - Extent of Overshoot greater - Amplitude of AP greater |
|
|
CARDIAC AP
- what variable changes accounts for the various phases of Cardiac AP? - how does the above have any effect? |
- Changes in PERMEABILITY of cell membrane
- Alters rate of ion passage across membrane |
|
|
CARDIAC AP
- when accounting for the various changes of cardiac AP, the cell membrane permeability involves the altering the rate of passage for what ions mainly? x3 |
- Na+
- Ca2+ - K+ |
|
|
CARDIAC AP
- define Permeability |
Net Quantity of Ion
that will Diffuse across each Unit Area of membrane per Unit Concentration Difference across the membrane per Unit Time |
|
|
CARDIAC AP
- define Equilibrium Potential |
Electrical Potential required
to Counterbalance Concentration Gradient so NO Net Ion Movement occurs |
|
|
CARDIAC AP
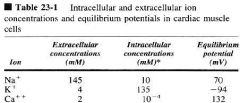
Equilibrium Potenital for: - Na+ - Ca2+ - K+ |
70 mV
- 94 mV - 132 mV |
|
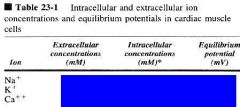
CARDIAC MUSCLES
Ion Concentration & Equilibrium Potential |
|
|
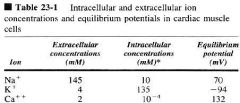
what does the -94 mV mean?
|
EQUILIBRIUM POTENTIAL
is the charge (potential) needed to Keep All the K+ ions Inside the Cell (to counterbalance the Concentration Gradient) |
|
|
RESTING POTENTIAL: IONIC BASIS
- what are the 2 OPPOSING FORCES involved in moving ions, such as K+? |
- Chemical
- Electrostatic |
|
|
RESTING POTENTIAL: IONIC BASIS
- Cell Membrane is relatively permeable to what ion? |
K+
(Pk+ >> Pna+ , Pca++) |
|
|
RESTING POTENTIAL: IONIC BASIS
[K+]in >> [K+]out : this favors what? |
- Outward Diffusion
|
|
|
RESTING POTENTIAL: IONIC BASIS
- as K+ diffuses out, what is retained within cell? - with respect to outside, K+ diffusion leaves the cell interior in what state? |
- Anions retained withiin cell
- Electronegative interior (w/ respect to outside) |
|
|
RESTING POTENTIAL: IONIC BASIS
- at equilibrium, what is equal? |
Chemical forces = Electrostatic forces
|
|
|
RESTING POTENTIAL & K+
- what is Ek? (aka?) - how is above value obtained? |
- Electrostatic Force of Potassium
(Nernst potential for K+) - Nernst Equation |
|
|
RESTING POTENTIAL & K+
- Nernst Potential for K+ = Ek = ??? - Ek is oriented how? - Ek is required for? |
-90mV to -100mV
Oriented with INSIDE cell being more NEG. than outside Counterbalance the Chemical Potential for K+ |
|
|
RESTING POTENTIAL & K+
- Membrane Potential (Vm) at rest? - IF the K+ were the ONLY Permeant ion, then? |
-80mV to -90mV
Ek = Resting Vm |
|
|
RESTING POTENTIAL & K+
- which is more negative: Ek or Vm? |
Ek is more negative than Vm
|
|
|
RESTING POTENTIAL & K+
- since Ek (-90mV to -100mV) is more negative than Vm (-80mV to -90mV), what is the result? |
Small Potential (10 to 15mV) tends to Drive K+ out of cell
|
|
|
NA+ EQUILIBRIUM POTENTIAL
- what is the Ena? - above Electrostatic force is oriented how? - above Ena is required to do what? |
40mV to 70mV
Oriented with INSIDE of cell more POSITIVE than outside Required to counterbalance the Chemical Potential for Na+ |
|
|
NA+ EQUILIBRIUM POTENTIAL
- is Na+ concentration greater outside or inside? - what is the Vm? |
outside
-80 mV to -90mV |
|
|
NA+ EQUILIBRIUM POTENTIAL
Since [Na+]out >> [Na+]in, AND Ena = 40mV to 70mV AND the Vm is -80mV to -90mV, what is the result? |
There is a Large
Electrical & Chemical gradient tending to PULL Na+ INTO the Cell |
|
|
NA+ EQUILIBRIUM POTENTIAL
- is the permeability of Na+ high or low? - what is the consequence? |
- Low Na+ Permeability
- Na+ entry into cell is also very low |
|
|
NA+ EQUILIBRIUM POTENTIAL
Since Na+ has a large chemical & electrostatic gradient driving Na+ inside, BUT has a low permeability allowing low entry into cell, what is the result? |
Small inward CURRENT of Na+
|
|
|
NA+ EQUILIBRIUM POTENTIAL
- small inward current causes what? |
causes
Vm to be slightly LESS NEGATIVE than predicted value of Nernst Eq. for POTASSIUM (K+) |
|
|
NA+ EQUILIBRIUM POTENTIAL
- External Na+ concentration has very little effect on what? - External Na+ concentration has a very large effect on what? |
- Vm
- Active Membrane (Depolarizing Cell) |
|
|
GOLDMAN EQUATION
- Goldman Eq. explains what? - Thus, the Goldman Eq. will imply what? |
- how Permeability of More than One ION influences Membrane Potential
- RELATIVE (not absolute) Permeabilities determine Vm |
|
|
GOLDMAN EQUATION
- at rest compare the permeabilities of K+ and Na+ |
Pk is 100 times more than Pna
|
|
|
ACTIVE TRANSPORT'S ROLE
T/F: the Cell is in Equilibrium for K+ and Na+ |
False
(K+ and Na+ is NOT in equilibrium) |
|
|
ACTIVE TRANSPORT'S ROLE
- the active transport will counter what? x2 - what is the important active transport called? |
- Loss of K+
& - Gain of Na+ - Na+/K+ ATPase |
|
|
ACTIVE TRANSPORT'S ROLE
- Na+/K+ ATPase requires what? - for what? |
- Energy required
- to Move Na+ against EC gradient |
|
|
ACTIVE TRANSPORT'S ROLE
- Na+/K+ ATPase does what? x2 - what is the effect of above? |
Pumps 3 Na+ OUT
& Pumps 2 K+ IN Makes cell INSIDE more NEGATIVE (b/c Eq. Potential for Na+ = +70mV & K+ = -94mV) |
|
|
ACTIVE TRANSPORT'S ROLE
- Na+/K+ ATPase effects on membrane? - via what process? |
- Depolarizes membrane
- Partial Pump Inhibition (depolarize membrane by dissipating the EC gradient) |
|
|
ACTIVE TRANSPORT'S ROLE
- Na+/K+ ATPase activity is increased how? x2 |
- Increase in Na+ INSIDE
OR - Increase in K+ OUTSIDE |
|
|
FAST RESPONSE: IONIC BASIS
- Threshold needed for? - what is the Threshold for Cardiac Fast Response? |
Potential needed to generate AP
-75 mV |
|
|
FAST RESPONSE: IONIC BASIS
Threshold Potential is the Potential at which ______ generated by _______ are sufficient enough to initiate __________ in which subsequent _______ becomes _____________ of the _________. |
- Inward Currents
- Membrane Depolarization - REGENERATIVE AP's - Depolarization - INDEPEDENT - of the Initial Stimulus |
|
|
PHASE 0 : UPSTROKE
- what does gNa mean? |
- Sodium Conductance
(thru fast sodium v-gated channels) |
|
|
PHASE 0 : UPSTROKE
- Upstroke is due to what? thru what? |
Sudden Increase
in Sodium Conductance thru Fast Sodium Channels |
|
|
PHASE 0 : UPSTROKE
- Fast Sodium Channels are what kind of mediated channels? |
- Voltage Gated channels
|
|
|
PHASE 0 : UPSTROKE
- as gNa suddenly increases, what happens to gK? - gCa? |
- Suddenly drops, plateaus, then returns to baseline
- Slowly goes up, than drops to baseline even slower. |
|
|
PHASE 0 : UPSTROKE
- thus the ionic etiology of the Phase 0 rapid upstroke is? |
- rapid increase in gNa
|
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
- Channels involved? - Na+ Activation gate called? - Na+ Inactivation gate called? |
- Fast Sodium Channels (V-gated)
- m gate - h gate |
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
CELL @ REST Resting cell Vm? [Na+]out =? [Na+]in = ? Ena = ? (what kind of force is this?) (what does this force favor?) |
-90 mV
145 mM 10 mM 60 mV (Chemical Force) (Favors Na+ Inward Flux) |
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
CELL @ REST - since the Vm = -90mV, what can be said about the Electrical Force? |
90 mV of Electrical Force favors INWARD Na+ Flux
|
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
CELL @ REST - Chemical Force? Favoring? - Electrical Force? Favoring? - Total EC Force? Favoring |
Chemical Force = Ena = 60 mV
(favoring Na+ INFLUX) Electrical Force = -90 mV (favoring Na+ INFLUX) Total EC Force = 60 - (-90) = 150 mV (favoring Na+ INFLUX) |
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
CELL @ REST - Despite the Total EC Force for Na+ being really high (150 mV), why would there by virtually no Na+ movement across the resting cell membrane? |
- Closure of m gates
thus the gNa is very low |
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
CELL @ REST - Closure of which gate implies a very low gNa+? |
- Closure of m gates.
|
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
- when would you have activation (opening) of m gates? |
when membrane depolarizes to -65 mV
|
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
- Activation (opening) of m gates is ___ dependent. - M gate opening is _______ process |
- Voltage Dependent
- Regenerative Process |
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
- as m gates open, Na+ enters the cell and does what to the charges inside? - this causes what effect on Vm |
- Neutralizes negative charges
- Reduces Vm |
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
- as m gates open, the influx of Na+ will reduce the Vm initiating what? x2 |
- Further opening of m gates
leading to - Further reduction in Vm |
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
- as m gates open, and Na+ enters cells what is the effect on the gradients? |
- Electrical gradient REDUCED as Na+ moves into cell
- Concentration gradient is not affected much |
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
T/F : the concentration gradient of K+ is appreciably affected by the inward flux of Na+ when m gates open. |
False
(both concentration gradients of Na+ and K+ is not affected appreciably) |
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
- with Na+ influx (via m gate openings), the Vm approaches 0, causing the Electrical gradient to have what influence on Na+ influx? |
- Electrical gradient exerts PROGRESSIVELY less influence on Na+ influx
(as Vm approaches 0) |
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
- with m gates open, Na+ enters cell via what gradient primarily? |
- Concentration gradient
|
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
- the continued influx of Na+, as Vm approaches 0, leads to what event? |
- POSITIVE Overshoot
|
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
- what terminates the Na+ influx? |
- Closure of h gates
|
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
- h gates are ______ dependent |
- voltage dependent
(just like m gates, dependent on membrane potential) |
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
- m gates open at what general rate? - h gates open at what general rate? |
- rapidly (0.1 to 0.2 ms)
- slowly (>1 ms) |
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
- H gates remain closed until? - above occurs in what phase? |
- cell has partially repolarized
- phase 3 |
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
- Until the H gates partially open, the cell remains in? - By the above mechanism, what is prevented? |
- Refractory mode to further excitation
- Sustained, Tetanic Contractions of Heart are prevented |
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
- Even after the Electrical gradient is dissipated, the Chemical gradient drives what? - until? - what cellular condition closes the h gates? |
- Na+ INFLUX
- Net ElectroNeutrality - ElectroPositivity (Vm = +30 mV) |
|
|
SODIUM (Na+) MOVEMENT @ PHASE 0
- what event completes Phase 0? |
- h gate closure
|
|
|
PHASE I : EARLY REPOLARIZATION
- Phase I reflects what initial influence? |
- Inactivation of Fast Sodium Channels
|
|
|
PHASE 2 : PLATEAU
- Phase 2 is mainly due to? - Phase 2 is also due to? |
- Influx of Ca2+
- also Na+ influx |
|
|
PHASE 2 : PLATEAU
- Ca2+ & Na+ influx is achieved via what type of channels? |
- Slow channels
|
|
|
PHASE 2 : PLATEAU
- what currents are created by Ca2+ and Na+? |
- Slow, Inward Ca2+ & Na+ currents
|
|
|
PHASE 2 : PLATEAU
- Slow, inward Ca2+ and Na+ currents are balanced by? - thus producing what? |
- Small, OUTWARD K+ current
- Maintaining Prolonged Plateau |
|
|
PHASE 2 : PLATEAU
- the balancing of Ca2+ & Na+ small inward currents, with a small outward current of K+, will maintain a prolonged plateau @ what Vm? |
- Vm close to 0
|
|
|
PHASE 2 : PLATEAU
- slow channels open at what threshold? - once slow channels open, describe the movement of ions. - what gradient is involved above |
- 30 to -40 mV
Ca2+ and Na+ begin to move into cell via Electro-Chemical gradients (but Chemical gradient is primary) |
|
|
PHASE 2 : PLATEAU
- After Phase 1 early repolarization, Vm is roughly 0, so ______ gradient for Ca2+ & Na+ provide ______ for ______ via ______ |
- Chemical
- Primary Force - Ca2+ & Na+ INFLUX via -Slow channels |
|
|
PHASE 2 : PLATEAU
- what ion and channel is involved in Excitation-Contraction Coupling? |
- Ca2+ that enter via Slow Channels
|
|
|
CALCIUM INDUCED CALCIUM RELEASE
- Excitation-Contraction coupling implies what? - what is DHP? - DHP function? - where do you find DHP's? |
- by the time you complete AP, you have greatest contraction
- Voltage Gated Calcium Channel - allows for Ca2+ influx - surface of Cardiomyocytes |
|
|
CALCIUM INDUCED CALCIUM RELEASE
- what is RYR? - where would you find RYR's? - Ca2+ binding to RYR does what? |
- Ligand-gated Ca2+ channels
- Sarcoplasmic Reticulum - Release large amount of Ca2+ from SR stores. |
|
|
CALCIUM INDUCED CALCIUM RELEASE
- what does it mean for Ca++ induced Ca++ release? |
- Ca2+ influx via DHP will enter cell and bind to RYR, thus triggering a large release of Ca2+ from SR stores
|
|
|
CALCIUM INDUCED CALCIUM RELEASE
- why is the usage of RYR so important in contraction? |
- 90% of Ca2+ needed for cardiomyocyte contraction come from SR stores.
|
|
|
ISOLATED EFFECTS:
GUINEA PIG PAPILLARY MUSCLE - experiment showed factors influencing what? |
- Factors influencing SLOW, INWARD Current
|
|
|
ISOLATED EFFECTS:
GUINEA PIG PAPILLARY MUSCLE - what are the factors/drugs that influenced the Slow, Inward, Current? x2 |
- Catecholamines
- Calcium Channel Blockers |
|
|
ISOLATED EFFECTS:
GUINEA PIG PAPILLARY MUSCLE - Catecholamines do what effect? x2 - List 2 examples of Catecholamines that do this? |
- Increase Slow Inward Ca2+ current
- Increase Contractability - Epinephrine - NE |
|
|
ISOLATED EFFECTS:
GUINEA PIG PAPILLARY MUSCLE - Calcium Channel Blockers do what effects? x2 - List 3 examples of Calcium Channel Blockers |
- Decrease the Slow, Inward Ca2+ current
- Decrease Contractability (DNV) - Diltiazem - Nifedipine - Verpamil |
|
|
CALCIUM CHANNEL BLOCKERS
- application of Diltiazem will have what effect on AP? - Force of Contractility? |
- Decrease AP
- Decrease Force |
|
|
CALCIUM CHANNEL BLOCKERS
- increasing the dosage of Diltiazem will effect AP and Force of Contractility how? |
- will Progressively DECREASE both.
|
|
|
ANOMOLOUS RECTIFICATION
- in NERVE cells, increased gK contributes to? - in HEART cells, what happens with gK? |
- Rapid Repolarization
- gK decreases after initiation of propagated AP |
|
|
ANOMOLOUS RECTIFICATION
- in the Heart, the decrease in gK after AP will have what effect on K+ rate? - this causes what? |
- Reduces rate at which K+ leaves the cell
- Prevents Repolarization of Cell during Plateau phase |
|
|
ANOMOLOUS RECTIFICATION
- what balances the Slow, Inward currents of Ca2+ and Na+? - this balance allows for? |
- Outward, Slow K+ current
- Maintenance of the prolonged plateau (seen in phase 2) |
|
|
PHASE 3 : REPOLARIZATION
- Phase 3 depends on what 2 processes? |
- Increased gK
- Inactivation of Slow, Inward Ca2+ & Na+ currents |
|
|
PHASE 3 : REPOLARIZATION
- in phase 3, gK is increased or decreased? - characterize the gK in Phase 3. x2 |
- Increased gK
- Voltage Dependent - Self-Regenerative |