Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
43 Cards in this Set
- Front
- Back
|
What subfamily does EBV belong to?
|
Gammaherpesvirinae
|
|
|
Gamma herpes viruses are characterized by:
- infection - cell target |
Latent
B-cells (proliferation) |
|
|
HHV-4 is also known as?
|
Epstein Barr Virus
|
|
|
HHV-8 is also known as?
|
Kaposi's Sarcoma Herpes Virus
|
|
|
T/F - EBV is the most prevalent of human virues.
|
True
|
|
|
EBV transmission. Describe
|
Typical direct, close personal contact
- saliva - blood - tissue transplant - sexual |
|
|
EBV:
- genome type - linear or circular - capsule - envelope - unique structure |
dsDNA
Linear (becomes circular in cell) Icosohedral envelope tegument |
|
|
EBV will INITIALLY infects what cells?
EBV eventually ENDS UP infecting what cells? Expansion of viral genome done through what? How long does it stay in host? |
Oropharyngeal epithelium
B-cells Forced proliferation of B-lymphocytes Lifetime |
|
|
List two benign diseases of EBV and describe their association with patients.
|
Infectious Mononucleosis (IM)
- targets immunocompetent Oral Hairy Leukoplakia (OHL) - targets immunosuppressed |
|
|
What is the classic triad for EBV induced IM?
|
Fever
Sore throat (pharyngitis) Cervical lymphadenopathy |
|
|
What is the hematological finding associated with EBV induced IM?
|
Greater than 10% ATYPICAL lymphocytes
|
|
|
What is the serotological finding associated with EBV induced IM?
|
Transient HETEROPHILE antibodies
Permanent EBV-sprecific antibodies |
|
|
When EBV infects a resting B-cell, describe the receptor interactions for:
- binding - fusion/entry |
B-cells CD21 receptor binds to viral gp350
B-cell HLA class II (HLA-DR) coreceptor binds to viral gp42-gL-gH |
|
|
When progeny viruses leave the resting B-cell, why do they lack a gp42?
What is the consequence of this? |
The gp42 will bind with the internally synthesized cellular HLA-DR. This causes them to become degraded along the proteolytic pathway.
Thus only gL-gH is found on the progeny virus. This is beneficial b/c epithelial cells will not allow entry to viruses with gp42, but will allow gL-gH entry. EBV can then make new progeny with gL-gH AND gp42 b/c epithelial cells do not have HLA molecules for it to bind to. |
|
|
EBV replication:
- rate - requires what? why? - depends on what enzymes |
Once per cell cycle
EBNA-1 b/c it binds to EBV origin of replication Cellular enzymes |
|
|
Why would acyclovir not work on EBV induced IM?
Can acyclovir be used at all when dealing with EBV diseases? |
Because this is a disease of latency and is dependent on cellular enzymes.
ACV is used to target viral polymerase and to inhibit lytic viral diseases Yes, can use with Oral Hairy Leukoplakia. |
|
|
EBV-Specific Cytotoxic T-cells:
- infected with EBV? - targets what - eliminates what |
Non-infected
EBV latency proteins (EBNAs & LMPs) proliferatint B cells |
|
|
T/F - Heterophile antibodies react with EBV antigens.
|
False.
These Ab target the massive random antibodies created by the proliferating B-cells. |
|
|
What test will detect heterophile antibodies?
How does this test work? |
Monospot test
These antibodies are IgM class that agglutinate sheep RBC's. |
|
|
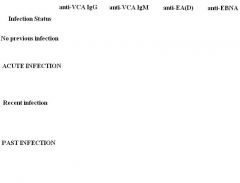
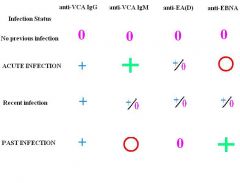
EBV-specific antibodies:
- persist for how long? - useful for what kind of infection? - essential for diagnosis? |
For LIFE
Acute Rarely, but can be used to distinguish for leukemia |
|
Question
|
Answers
|
|
|
What is the average incubation period for IM?
|
50-60 days
|
|
|
What organ complication can occur with the overload of B-cells in IM?
|
Splenic rupture.
|
|
|
What are the hematological complications of IM?
|
Hemolytic anemia
Thrombocytopenia Neutropenia |
|
|
What is the most frequent cause of death in IM complications?
What is the recovery prognosis for such a complication? |
Encephalitis/Meningitis
85% complete recovery |
|
|
IM usually manifests how for children:
- usually what symptoms during seroconversion? - any atypical presentations? |
Usually asymptomatic seroconversion
Neutropenia Periorbital swelling Rash Respiratory infection |
|
|
What is so unique about the serology of IM children?
|
50% - HETROPHILE NEGATIVE !!!!
(80% when less than 4 y.o.) |
|
|
IM manifestion for young adults:
- symptomatic association - serology |
50% symptomatic at primary infection
90% heterophile positive |
|
|
IM manifestation for elderly:
- common symptoms x3 |
Fever
Abdominal pain Hepatic abnormalities |
|
|
T/F - For IM, is acyclovir used?
why or why not? |
Not indicated
It inhibits EBV replication, yet IM is a disease associated EBV LATENCY! |
|
|
What is the best treatment for IM?
|
Supportive
|
|
|
When would you use corticosteroids for IM? x3
|
Impending airway obstruction
Severe thrombocytopenia Hemolytic anemia |
|
|
List all the EBV associated disease that involve B-cells.
|
Burkitt's Lymphoma
Hodgkin's Lymphoma IM PLTD (post transplant lymphoproliferative disorder) |
|
|
Describe the genetic association with Burkitt's Lymphoma.
|
Associated with a translocation involving chromosome 8 (c-myc gene)
AND chr 2, 22, 14 |
|
|
EBV Latency proteins
- how many LMPs (latent membrane proteins) - how many EBNAs (Epstein Barr Nuclear Antigens) |
3
6 |
|
|
EBV latency proteins are:
- critical for what in vivo - required for what in vitro |
B-cell proliferation
Cell transformation |
|
|
What is unique about the total CD8+ T-cell pool in association with EBV?
|
EBV-specific CD8+ T-cells constitute 5%
|
|
|
Specify the EBV latency proteins in the tumor tissues associated with the following:
- Post transplant lymphomas - Nasopharyngeal Carcinoma (NPC) - Gastric Carcinoma - Hodgkin's Lymphoma - Burkitt's Lymphoma |
All 9
EBNA-1, LMP-1, LMP-2 EBNA-1, LMP-1, LMP-2 EBNA-1, LMP-1, LMP-2 Only EBNA-1 |
|
|
In order to survive T-cell detection, EBV will do what?
|
Downregulate latency proteins to just EBNA-1, LMP-1, and LMP-2
|
|
|
Describe the latency proteins associated with exploiting the physiological B-cell pathway.
|
EBNA-1 : maintains episome in cell
LMP-1 : Mimicry of CD40 receptor LMP-2 : Mimicry of B-cell receptor/surface immunoglobulin |
|
|
List the EBV associated disease that involves epithelial cells. x3
|
Nasopharyngeal carcinoma (NPC)
Oral Hariy Leukopenia (OHL) Gastric Carcinoma |
|
|
Nasopharyngeal Carcinoma (NPC)
- prevalent population - characterized by what type of infection - symptom |
Southern Asia + Alaskan eskimos
Latency Highly metastatic beginning in the OROPHARYNX, and may travel to cervical. |
|
|
Oral Hairy Leukoplakia (OHL)
- prevalent population - characterized by what type of infection - Symptom - Can look like what other syndrome? |
Immunosuppressed patients (AIDS)
Active Viral Replication Benign hyperplastic lesion of epithelial cells in tongue Candida |