Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
82 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
what is a lymphoma?
|
proliferation of lymphocytes as discrete tissue masses
|
|
|
|
what is precursor B or T cell lymphoblastic lympohoma aka
|
ALL
|
|
|
|
how does lympohoma present
|
painless lymphadenopathy (swollen nodes)
constitutional or B symptoms:fever, loss of appetit, weight loss immunologic disturbances: autoantibodies, monoclonal protiens, recurrent infection extranodal masses: skin, gonads, testes, eye, brain |
|
|
|
what is walderyers ring?
|
a circle of lymphnodes that act as oral survalence, can be a sight of lymphoma
|
|
|
|
how is lymphoma diagnosed
|
must have biopsy of lymph node
preferably whole lymphnode |
|
|
|
what type of cell type is in most malignant lymphomas
|
b cells
|
|
|
|
what is hodgkin lymphoma
|
presence of hodgkin and reed-sternberg cells
nonneoplastic inflammartory cells migrate into nodes bc of RS cells RS cells are responsive to treatment but but the nodes dont shrink bc most of the cells in the swelling are inflammartory there are very effective treatment protocols which is why its important to get the diagnosis for it. |
|
|
|
what are the subytpes of hodgkin lympohoma?
|
nodular sclerosis
mixed cellularity lymphocyt rich lymphocyte depleted - the four above represent classical HL with RS cells lymphocyte predominant |
|
|
|
what are the two most common types of HL
|
nodular sclerosis
mixed cellularity |
|
|
|
what are the classificatino of lymphoid neoplasms
|
I precursor B cell neoplasms
II periperal B cell neoplasms III precursor T cell neoplasms IV peripheral T cell and NK cell neoplasms V Hodgkin lymphoma |
|
|
|
what is the difference between precursor and perhipheral neoplasms when refering to lymphoma?
|
precursor is mainly blasts
peripheral is more mature cells |
|
|
|
What are common lyphoid precurors(CLP)
|
the first cell in the develpment process of the lymphocyte found in the bone marrow
|
|
|
|
what can the Naive B Cell (NBC) give rise to
|
small lymphoctic lymphoma/leukemia
CLL |
|
|
|
What can the germinal center give rise to?
|
follicular lymphoma
Burkitt lymphoma diffuse large B cell lymphoma HODGKIN LYMPHOMA |
|
|
|
What can the marginal zone give rise to?
|
Diffuse Large B Cell lymphoma
marginal zone lympohoma small lymphocytic lymphoma CLL |
|
|
|
Where do T cell lymphomas arise
|
precursor T cell lymphoma arises in the thymus from DN cells
peripheral T cell lymphoma arise from the lymph node |
|
|
|
what defines a b cell lymphoid malignancies
|
monoclonal: that is a population all derived from one cell and produce all the same type of heavy or light immunoglobulin chains
so all look the same under a microscope |
|
|
|
what defines a T cell lymphoid malignanciy
|
also monoclonal but does not make immunoglobulins, so abnomal loss or gain of surface antigens, T cell receportor arrangement studies helpful.
|
|
|
|
what is the most common B cell lymphoma
|
diffuse large B cell lymphoma
|
|
|
|
what is the most common T cell lymphomas
|
periperal T cell lymphoma, NOS
|
|
|
|
What is the characterization of diffuse large B cell lymphoma?
|
a proliferation of large neoplastic B lympohid cells
- nuclear size equal to or exceding normal macrophage nuclei or more than twice the size o a normal lymphocyte have a diffuse not nodular growth pattern. |
|
|
|
immuno-histo chemistry of a B cell lymphoma would show what?
|
brown staining of all cells
|
|
|
|
what is the marker used to identify B cell lymphoma
|
CD20 main one
CD19, CD22, CD79a |
|
|
|
what gene translocation can be present in B cell lymphoma and what is the difference btw them
|
bcl-2,t(14;18) occurs in 20-30% and usually indicates that this arose from a follicular lymphoma
bcl-6 gene, (3q27 rearrangment) occurs in 30% and usually indicates de novo developement caused by dysregulation of germinal centers. |
|
|
|
what stage is a lymphoma if there is bonemarrow involvment
|
stage 4
|
|
|
|
what are the two speacial subsets of diffuse B cell lymphoma
|
immunodeficiency associated
body cavity |
|
|
|
what is the cause in immunodeficiency associated diffuse B cell lymphoma?
|
sever T cell depletion allows emergence of malignant B cells
OFTEN assiated with EBV |
|
|
|
what is the cause of Body cavity associated diffuse B cell lymphoma
|
neoplasm arises in the body fluids,(plural, pericardial, abdominal, )
ASSOCIATED WITH KSH/HHV8/EBV viruses deadly only in AIDS patients with kaposi sarcoma. jellyfish like cells |
|
|
|
what is the second most common type of lymphoma in the western world
|
B Cell follicular Lymphoma characterized as being nodular rather than diffuse.
|
|
|
|
what is the prognosis of folicular lymphoma
|
not bad
the folicular lymphoma is indolent which means the cells are more mature when they become cancerous. |
|
|
|
what are the implications of indolent lymphoma
|
indolent means they are more mature which means they are much less agressive so they tend to cause less problems than other cancers. but because they are more mature they do not respond to most modern therapies that target rapidly dividing cells. so they are generally not curable.
|
|
|
|
what is a centrocyte
|
a cleaved follicle center
|
|
|
|
what is a centroblasts
|
a large noncleaved folicle center cell
|
|
|
|
how do you grade follicular lymphoma
|
grade 1 0-5 centroblasts per HPF
grade 2 6-15 centroblasts per HPF grade 3 >15 centroblasts per HPF basically the more centroblasts the higher the grade. |
|
|
|
what do higher grades of follicular lymphoma indicate
|
the higher the grade the more likely that the lymphoma will turn into diffuse B cell lymphoma which is much more dangerous.
|
|
|
|
how do you treat grade 3 follicular lymphoma
|
the same way you treat diffuse B cell lymphoma
|
|
|
|
what are the markers for follicualr lymphoma
|
all B cell markers are the same so just like DBCL there are (CD19,20,22,79a) but the one that is characteristic of follicular lymphoma is CD10 which indicates follicluar center origin
|
|
|
|
what other cancer can be identified by CD10 markers
|
precursor B acute lymphoblastic leukemia/lymphoma.`
|
|
|
|
what is the main gene translocation in follicular lymphoma
|
t(14;18)
BCL2 gene inhibits apoptosis, so follicular center cells have polonged survivial. |
|
|
|
what are the features of follicular lymphoma
|
exclusively to adults
indolent can progress to diffuse B cell lymphoma |
|
|
|
discribe the extranodal marginal zone b cell lymphoma of MALT
|
also called maltoma
orginates from marginal zone of lymphnoded then spreads out of lymphnode mostly seen in GI tract mainly in stomach can be caused by helicobacter pylori gastritis can be treated by antiboitic may progress to DLBCL with t(11;18) then resistant to antibiotics |
|
|
|
discribe the small lympocytic lympoma
|
same as CLL but all in the lymph node
mainly in male around 65yo |
|
|
|
What is mantle cell lynmphoma
|
B cell neoplasm composed of small to medium sized cells
most commin invovles lympnodes but may be extranodal in spleen bonemarrow gi or waldeyer ring male 60yo 3-5year survival |
|
|
|
what gene is associate with mantle cell lymphoma?
|
cyclin D1(11)-promotes G1 to S phase
t(11;14)(q13;q32) |
|
|
|
discribe Burkitt's lymphoma
|
highly agressive
doubles overnight all cells dividing seen with EBV same cell found in ALL found extranodally |
|
|
|
what are the three types of burrkitts lymphoma
|
endemci-starts in jaws and facial bones found in africa with EBV
sporadic - presents with abdominal masses immunodeficiency associated with AIDS nodal loclization and bone marrow. |
|
|
|
what is tumor lysis syndrome
|
when cells are so sensitive to chemotherapy that it produces rapid cell death and hyperkalemia
can be found in burketts lymphoma |
|
|
|
what is the morphology of Burkketts lymphoma
|
clear halo around the cells
called stars in the sky lots of mitotic figures |
|
|
|
what is the gene most often afected in burketts lymphoma
|
c-MYC gene- thought to affect progression from G2 in cell cycle
t(8;14), t(2;8, t(8;22) |
|
|
|
what are some characteristics of mature T and NK cell neoplasms
|
usually agressive
more common in asia, carribean and Mexico only 5 year expected survival classified by flow cytometry clicical presention and t cell receptor rearrangements |
|
|
|
what are the defining elements of the reed sternberg cells of Hodgkins lymphoma?
|
reed sternberg cells that draw reactive inflammatory cells into lymphnodes
RS typically binucleated but can be mono or multi nucleated as well all nuclei have a single larg eosinophilic neucleoli inflammatory cells that surround the RS cells are benign lymphocyts, macrophages, granulocytes, eosinophils |
|
|
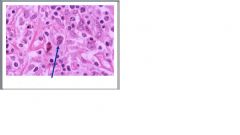
what is this?
|
reed sternberg cell
|
|
|
|
what lineage of cell type does the reed sternberg cell come from?
|
B cell
|
|
|
|
what are the typical clinical features of Hodgkins lymphoma?
|
nodal based disease with contiguous spread(spreads from node to node in close proximity as opposed to malignant lymphoma which will spread all over above and below the diagphram, HS typically is either above or below the diaghram.)
painless enlargment of lymphnodes fever nightsweats unexplained wieghtloss |
|
|
|
what are the B symptoms?
|
fever night sweats unexplained wieght loss
|
|
|
|
what two thing determine prognosis for hodgkins lymphoma?
|
subtype and staging
|
|
|
|
what is the order of subtypes by worsening prognosis
|
excellent: lymphocite rich
nodular sclerosis good; mixed cellularity intermediate to unfavorable: lymphocyte depleted |
|
|
|
what is the most common subtype of HL
|
nodular sclerosis Hodgkins lymphoma
|
|
|
|
what is the character of Nodular sclerosis Hodgkin lymphoma?
|
collagen bands that surround nodules and lacunar type HRS cells
28yo mediastinal invovlment usually presents stage 2 |
|
|
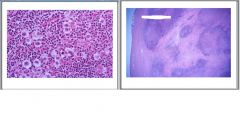
what do these two pictures portray?
|
Nodular sclerosis hodgkins lymphoma
|
|
|
|
what are the characteristics of mixed cellulartiy HL
|
37yo
male presents stage III or IV B symptoms(fever, nighsweats, weightloss) periperal lymph node invovlement |
|
|
|
where do plasma cells come from?
|
lymphocytes
|
|
|
|
what is a plasma cell neoplasm
|
neoplastic plasma cells secreting an intact monoclonal immunoglubulin or fragment (M protein)
|
|
|
|
what are the subtypes of plasma cell neoplasms
|
plasma celll myelomo(multiple myelomo)
lymphoplasmactyic lymphoma/waldentrom macroglobulinemia solitary myeloma(plasmacytoma) monoclonal gammopathy of uncertain significnace (MGUS) |
|
|
|
what is the most common of the plasma cell neoplasms
|
MGUS
|
|
|
|
what are the characters of multiple myeloma
|
its is a neoplasm of a mature plasma cell
produces IgG or IgA 65-70yo more common in AA clincical findings due to the immunoglobulins can infiltrate the bone marrow and cause anemia/thrombocytopenia. |
|
|
|
what causes bone pain in multiple myeloma?
|
tumor cells release ctyokines to upregulate RANKL to activate osteoclasts this can lead to hypercalcemia, urinary stones
most common bones invovled are vertebral bodies, ribs, skill, pelvis, femur, clavicle, scapula |
|
|
|
what are the clincical symptoms of multiple myeloma?
|
bonemarrow infiltration leads to symptoms of anemia, weakness, fatigue
RBC rouleaux:stack of coins -RBC get stuck together by extra protiens in the blood recurrent bacterial infections renal insufficiency: immunoglobulin fragments toxic to kidney(bencejones protienuria) spinal cord compression neurologic, due to amyloid infiltration into nerves parasthesias, mental alterations, neuroligc effects of hypercalcemia |
|
|

what does this picture show
|
RBC rouleaux
indicative of multiple myeloma |
|
|

review this chart
|
what are the four things that multiple myeloma causes and what are their consequences?
|
monoclonal protein
-positive electrophoresis -bencejones proteinura -renal failure -hyperviscosity -amyloidosis immune deficiency -decreased IgG -infection anemia -caused by bonemarrow infiltration bone destruction -fractures -punched out radiographic bone lesions -bone pain -hypercalcemia -urninary stones -neurologic issue |
|
|
what is the diagnostic triad for multiple myeloma
|
punched out lytic bone lesions
monoclonal protien on electrophoresis:restircted mobility plasmacystosis of bone marrow aspirate |
|
|

what does this electrophoreis represent?
|
monoclonal antibodies because of the single line instead of blurred lines from multple cell lines.
|
|
|
|
what are the molecular abnormatlities for multiple myeloma
|
Ig heavy chain rearragnement on 14q32
dyreg of D cyclins deletion of 13q |
|
|
|
what is the major treatments for MM
|
bone marrow transplant
chemotherapy thalidomide |
|
|
|
describe lymphoplamacytic lymphoma
|
a lymphoma of Bcells that are turning into plasma cells but arent there yet
they secrete IgM incurable and progressive Hyperviscosity (waldenstrom macroglobinemia):super thick bc IgM is so large leads to visual problems bc retina vein congestion, neuroligic headaches dizziness, deafness, bleeding due to intereference with clotting factors, and cryoglobulinema which is precipitation fo IgM at low temps ie Raynaud's and cold urticaria |
|
|
|
how is lymphoplasmacytic lymphoma treated
|
plasmapheresis
anti CD20 antibody presents as lymphoma with no lytic bone lesions |
|
|
|
discribe MGUS
|
monoclonal immunoglobuin in blood, urine, or both
no clinical signs or symptoms of plasma cell myeloma or lymphoma. serum M protein level less than 3gm/dL plasma cells show same chromoaslma trnasloactions as full blown MM this is most likly an early stage of MM. |
|
|
|
how is MGUS followed up
|
close monitoring for monoclonal protiens watch for bence jones proteinura
1% / year convert to MM |
|
|
|
what are the groups of MGUS
|
group 1: no significant increase M protien(10%)
group 2: M protein increased to > 3g/d:(11%) no plasma cell dyscrasia developed group 3: died of unrealted cause (53%) group 4: develped MM or realtead disease median of 10 years. |
|
|
|
what two thing help us classify if a patient with MGUS is in class 4 and may have a risk of progressing to MM
|
IgG M protein
abnormal serum kappa:lambda light chain ratio |
|
|
|
discribe solitary myeloma(plasmacytoma
|
a variation where the plasma cell has an unusual adhesion marker so it stays in one place
can arise in soft tissue or bone -bone: same places as MM is found -soft tissue: lung, oronasopharnx, nals sinuse bone location usually progress to MM soft tissue usually doesnt and can be resected with high chance of cure |
|
|
|
discribe plasma cell leukemia
|
a secondary condition to MM where the disease has progressed so far that the plasma cells spill out in into the blood
poor prognosis treate with aggressive chemo and bone marrow stem cell transplant. |
|