![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
38 Cards in this Set
- Front
- Back
|
What is respiratory diverticulum derived from |
Outgrowth of proximal foregut of endoderm |
|
|
What does respiratory diverticulum form |
tracheal bud which grows into splanchnopleuric mesoderm |
|
|
what happens to respiratory diverticulum in week 5 |
a septum grows, dividing trachea and oesophagus (tracheo-oesophageal septum). tracheal bud then grows into splanchopleuric mesoderm. |
|
|
what happens if tracheo-oesophageal septum fails to form |
tracheoesophageal fistula forms, linking the two -> infection - failure to thrive |
|
|
what does splanchnopleuric mesoderm form |
- lining and glands of respiratory tract - smooth muscle - blood vessels - cartilage - visceral pleura |
|
|
What is branching morphogenesis |
each lung bud divides many times to form the bronchial tree |
|
|
what are the 4 lung bud divisions |
1 = primary bronchi formation 2 = secondary bronchi (lobar) 3 = segmental bronchi 4 = intra segmental (bronchopulmonary segments) |
|
|
when do the 4 lung bud divisions occur |
primary = 28 days secondary = 33 days segmental = week 7 intra-segmental = |
|
|
when does respiratory epithelium appear |
week 26, appears in the terminal bronchiole sacs - thins to simple squamous epithelium to allow gas exchange |
|
|
when is surfactant produced |
6 months - allow air spaces to inflate |
|

|
|
|
|
surface markings of apex of lung |
2-3cm above medial one third of the clavicle |
|
|
surface markings of R lung |
apex ->4th cc -> 6th cc - moves away from midline -> 8th cc midclavicular line -> 10th cc midaxillary line - 10th rib posteriorly is the base |
|
|
surface markings of L lung |
apex -> 4th cc - moves away from midline (cardiac notch) -> 6th cc -> 8thcc midclavicular line -> 10th midaxillary line - 10th rib posteriorly |
|
|
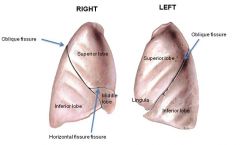
surface markings of the oblique fissure |
T3 to 6cc |
|
|
surface marking of horizontal fissure |
4cc to oblique fissure |
|
|
surface markings of pleura |
apex - 4thcc - 6cc - 8th rib midclavicular - 10th rib midaxillary - 12th rib posteriorly |
|
|
where is costodiaphragmatic recess |
v shaped recess in parietal pleura between thoracic wall and diaphragm - 5cm vertical between 8th and 10th rib on midaxillary line |
|
|
what is function of costodiaphragmatic recess |
for expansion during deep inspiration. fluids may collect here, pleural effusion. |
|
|
4 parts to parietal pleura |
1) cervical 2) diaphragmattic 3) mediastinal 4) costal |
|
|
3 points of pleural reflection |
1) sternal line - anteriorly 2) costal line - inferiorly 3) vertebral line - posteriorly |
|
|
which nerves supply parietal pleura |
diaphragmatic and mediastinal = phrenic nerve (C3, 4, 5) costal = intercostal nerves |
|
|
what holds the two pleural layers together |
surface tension |
|
|
tension pneumothorax |
deviation of trachea AWAY from side of tension |
|
|
where would you insert a chest drain |
ideally 5th or 6th intercostal space midaxilla or 2nd, 8th or 10th intercostal space if reasoning can be rationalised |
|
|
structures in the hilum |
bronchi pulmonary arteries and veins bronchial arteries and veins bronchopulmonary lymph nodes pulmonary plexus of nerves pulmonary ligament |
|
|
which nerve is anterior to hilum |
phrenic nerve |
|
|
which nerve is posterior to hilum |
vagus nerve |
|
|
Left Medial wall of the lung relations |
aortic arch descending aorta pulmonary trunk cardiac impression left braciocephalic vein oesophagus subclavian artery |
|
|
Right medial wall of the lung relations |
arch of azygos vein superior vena cava inferior vena cava right braciocephalic vein oesophagus |
|
|
which parts of the lung drain to right lymphatic duct |
right lung and left lower lobe |
|
|
which parts of the lung drain to thoracic duct |
left lung upper lobe |
|
|
what is the carina |
cartilaginous ring within trachea at site of tracheal bifurcation |
|
|
significance of carinal angle |
indicates carcinoma of carinal lymph nodes |
|
|
trachea anatomy |
starts at C6 (cricoid cartilage) bifurcates at T4 (sternal angle) enters hilum at T5/6 (left primary bronchus passes under arch of aorta) |
|
|
tracheal wall |
incomplete C shapes of hyaline cartilage plus trachealis muscle. become complete cartilage rings at hilum. |
|
|
function of trachealis muscle |
contracts during coughing - reducing size of tracheal lumen to increase rate of airflow |
|
|
tracheal nerve supply |
autonomic = CN X and sympathetic |