Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
133 Cards in this Set
- Front
- Back
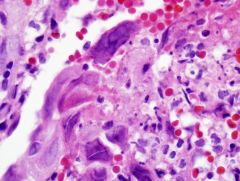
Rapid onset
|
Diffuse alveolar damage
Hyaline membranes Form of acute lung injury |
|
|
"Organizing pneumonia"
(aka BOOP, COP) Polypoid plugs loose connective tissue in alveoli INTRA-ALVEOLAR Form of acute lung injury |
|
Hazy ground glass opacities on radiology
|
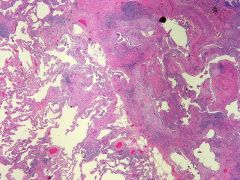
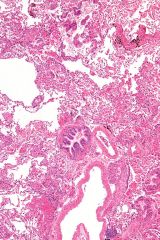
UIP
Temporal heterogeneity! HONEYCOMB FIBROSIS COLLAGENOUS SCARRING (subpleural) RECENT FIBROSIS (fb foci) Normal lung centrally |
|
|
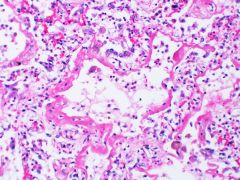
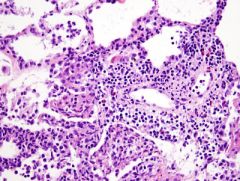
Diffuse thickening alveoli? with hyaline membranes?
|
ALI = DAD
thickening is NOT fibrosis! |
|
|
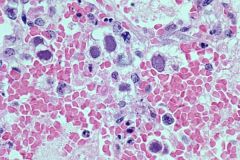
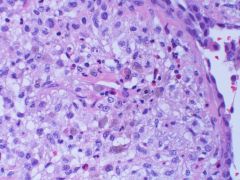
Alveoli filled with macrophages?
|
DIP
|
|
|
Bronchiolocentric fibrosis ddx
|
HP / inhaled
Smoking related Infection Airway disease CVD |
|
|
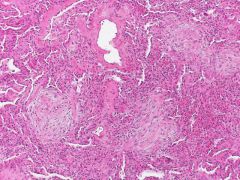
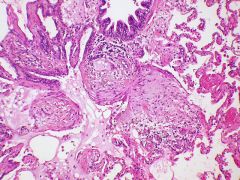
Fibroblastic foci of UIP
|
|
|
Microscopic honeycombing
|
irregular airspaces
lined by bronchiolar epith filled with mucus & macrophages surrounded by dense fibrosis smooth muscle metaplasia seen in UIP |
|
|
2 interstitial lung diseases associated with smoking
|
DIP
RBILD |
|
ground glass opacities in a smoker
stain? |
DIP
Uniform thickening alv septa will stain dusty blue with iron but NOT HEMORRHAGE |
|
uniform thickening.
causes? |
NSIP
temporal uniformity Alveolar septal thickening from CVD, drug, HP |
|
|
2 types NSIP?
|
Cellular: responds to steroids
Fibrosis: 40% 5-year survival |
|
|
Px in UIP?
|
Poor
20% 5-year survival |
|
This process was seen centrally but not peripherally
|
RBILD
(respiratory bronciolitis ILD) Filling of airspaces with pigmented macrophages Seen to an extent in every smoker Seen around respiratory bronchioles |
|
|
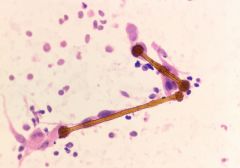
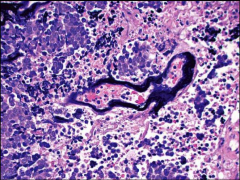
what is a ferruginous body?
What is a significant #? |
Particle coated with iron by pulmonary macrophage
Marker of pneumoconiosis Asbestos, talc, Generally significant if >1/cm^2 |
|
|
Asbestos
Straight, transparent core |
|
|
What inhaled lung disease preferentially affects the lower lobes?
|
Asbestosis
|
|

|
Pleural plaque
think ASBESTOS First site of involvement by asbestos |
|
What types of asbestos are there?
|
6 types
Serpentine class (curly) - Chrysotile fibers are the only member of this class. Most of US forms. Less pathogenic. Amphibole (straight) - Amosite, crocidolite, tremolite, anthophyllite and actinolite |
|

Weakly polarizable
|
Silicosis
VERY FIBROGENIC! Scarred rounded nodules UL > LL |
|
|
Silica + Silicate = ?
|
Mixed dust fibrosis
Stellate nodules with needle shaped crystals |
|
|
Coal worker pneumoconiosis
Pigmented macrophages around bronchovasc bundle (DUST MACULE) leads to progressive massive fibrosis (>1cm!) collapse normal lung with scarring UL > LL |
|
"Cannibalistic giant cell"
|
Hard metal pneumoconiosis
aka giant cell interstitial pna (old name) Dusty cobweb fibrosis Cobalt tungsten Workers with sawblade sharpening, diamond blades |
|
What pneumoconiosis is indistinguishable from sarcoidosis on histology?
|
Berylliosis
Non-nec granulomas with lymphangitic spread Bronchovasc bundles, Interlobular septa, subpleural |
|
|
Specific test for dx berylliosis?
|
Lymphocyte proliferation test (send out)
|
|

|
IV Talcosis
Crushed drugs **Vasculocentric granulomas Chunky crystalline polarizable material |
|
Farmer
|
HP
Organizing pna in alv duct **Branching fibroblast foci** different than that of BOOP |
|
Bird owner
|
Hypersensitivity pneumonitis
|
|
|
Classic triad of HP?
|
Bronchiolocentric lymphocytic interstitial inflammation
Poorly formed granulomas (loose) Organizing pneumonia (often branching fb foci) |
|
|
What type of allergic rxn is HP?
|
Type 3 (Ab-Ag mediated)
& Type 4 (Tcell mediated) |
|
|
Eosinophilic pneumonia
eos, macrophages, fibrin in airspaces Frequently drug related |
|
|
What is the syndrome with eos in lung and parasitemia?
|
Loefflers syndrome
|
|
|
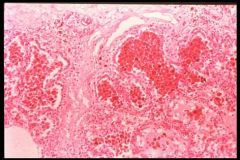
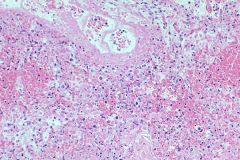
Diffuse alveolar hemorrhage
Many causes (Goodpasture, Wegeners, idiopathic) |
|
|
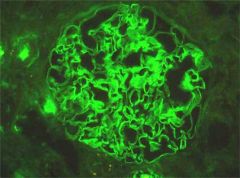
Anti-GBM
Linear staining IgG & C3 |
|
|
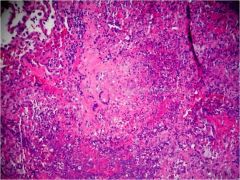
Wegeners granulomatosis
Geographic basophilic necrosis Scattered giant cells vasculitis neutrophilic abscesses |
|
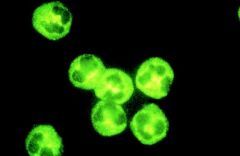
IF type?
Antibody to? |
cANCA in Wegeners
Anti-proteinase-3 |
|
|
Acute bacterial pneumonia
|
|
|
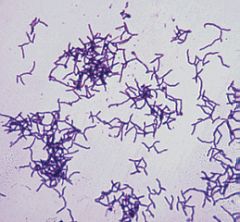
Sulfur granule actinomyces
|
|
|
Actino vs nocardia?
|
Both: Gram+ filamentous, GMS+
Actino: Sulfur granules Nocardia: weakly AFB+ |
|
|
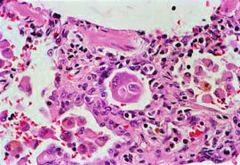
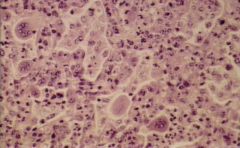
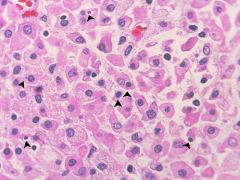
CMV
NUC & CYT inclusions |
|
|
Cowdry A vs Cowdry B inclusions?
|
Seems to be confusion about this in the literature. Cowdry A is known and defined, however Cowdry B was classically in polio as small round red inclusions, however it is though that these were not actually real. There is also talk of a intrnuclear BASOPHILIC inclusion as Cowdry B in adenovirus.
Cowdry A: large and usually eosinophilic intranuclear body surrounded by an empty narrow rim, which in turn is surrounded by a thickened nuclear membrane Intranuclear, eosinophilic. Seen in HSV, VZV, CMV Basically, for boards: Cowdry A: HSV, VZV; Cowdry B: Adenovirus, polio |
|
|
HSV
|
|
|
Adenovirus
Smudgy, Cowdry B Bronchiolonecrosis is helpful |
|
|
Adenovirus
|
|
|
RSV
|
|
|
Warthin Finkeldy Cell
Multinucleated giant cell Each nucleus has inclusion Also cytoplasmic inclusions |
|
|
Necrotizing granuloma
Fungal or mycobacteria |
|
|
hot tub lung?
|
MAI
Mycobacterium avium intracellulare Also causes cavitary disease in COPD |
|
|
Lade Windemere Syndrome
|
MAI in advanced AIDS patients
|
|

|
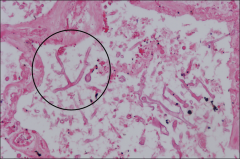
Aspergillus
Acute angle branching Septate hyphae Fungus ball ABPA Angioinvasive |
|
|
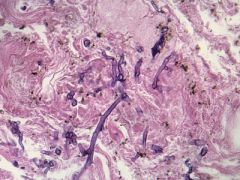
Mucor
Irregular ribbon like branching Empty appearing Non-septate hyphae Right angle branching |
|
|
Malakoplakia
|
|
|
What organism associated with malakoplakia lung?
|
RHODOCOCCUS EQUI
|
|
|

Dirofilaria
Dog heartworm / tapeworm |
|
|
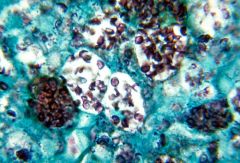
Histoplasmosis
MS River Valley 3-5um Calcified granulomas |
|
|
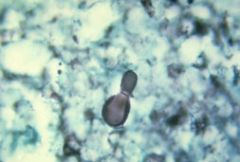
Blastomycosis
C & SE US Broad based buds <25um |
|
|
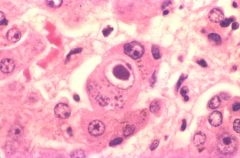
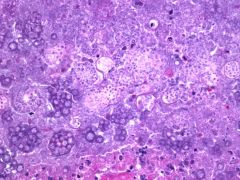
Coccidioides
SW US Endospores in large spherule 20-60um |
|
|
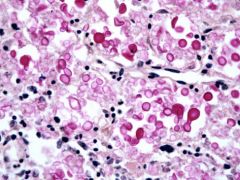
Cryptococcus
minimal inflammation MUCIN + CAPSULE 5-10um |
|

|
PCP
"Froth & dot" 7 um |
|
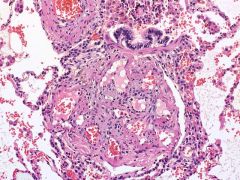
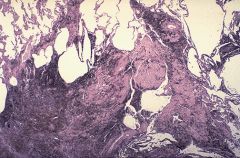
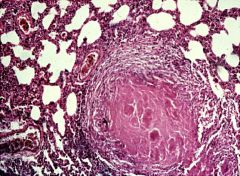
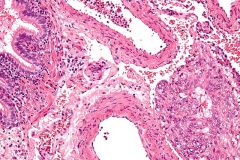
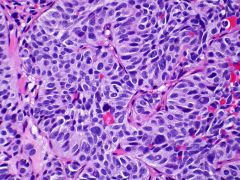
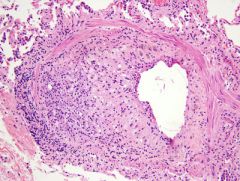
What is this lesion called?
|
Plexiform lesion of pulmonary hypertension
TUFTED lesion with small endothelial channels Recanalized More often seen in PRIMARY pHTN |
|

|
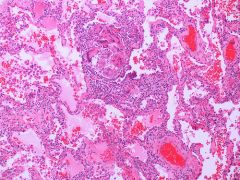
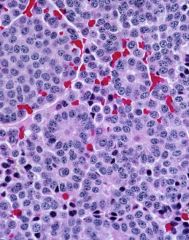
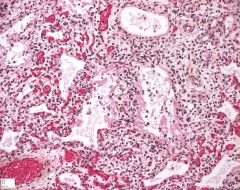
Classic wedge-shaped distribution of hemorrhage in a pulmonary infarct (due to dual blood supply)
|
|
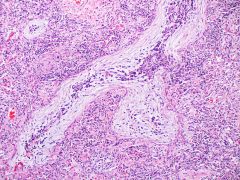
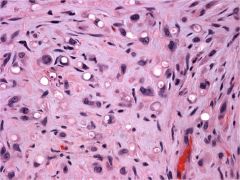
dx?
|
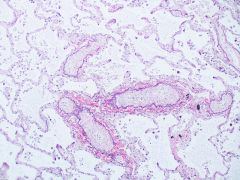
Pulmonary veno-occlusive disease
A very difficult dx to make! Simulates fibrosis Fibrous obliteration; thickened vessels (P.Veins located in septae) ALVEOLAR SIDERPHAGES elastin stain highlights |
|
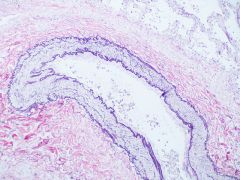
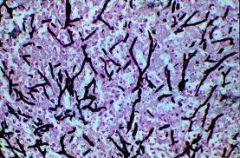
Elastin stain showing?
|
Normal pulmonary artery
Unique - has internal elastic lamina AND external The external elastic lamina is not present in muscular arteries in the systemic circulation |
|
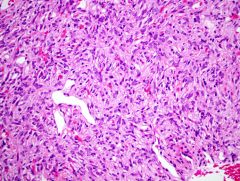
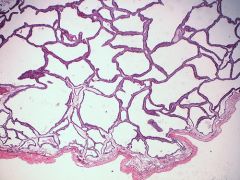
30F with hemoptysis
stains? |
LAM
(lymphangioleiomyomatosis) Cystic disease of lung lined by smooth muscle present with hemoptysis, PTX, chylothorax 50% 10year survival slowly progressive +ER +HMB45 +SMA |
|
|
Who gets LAM?
|
Young to middle-age females
AND patients with TS (TSC1&2 gene) |
|
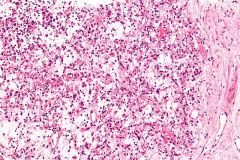
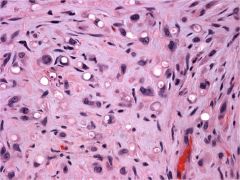
Apical nodule in a smoker
|

Langerhans cell histiocytosis
BRONCHIOLOCENTRIC Coffee bean shaped nuclei Eosinophils Can present with cystic disease S100, CD1a+ |
|
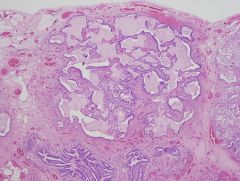
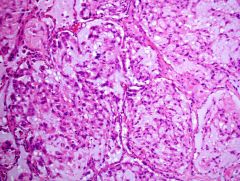
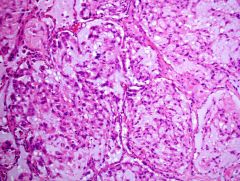
stain?
|
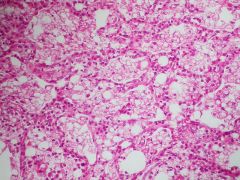
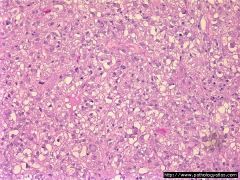
Pulmonary alveolar proteinosis
Surfactant accumulation Congenital form: surfactant B deficiency Kids acquired: immune deficiencies Adult form: antibodies to GMCSF PAS+ |
|
|
Exogenous lipoid pneumonia
pt taking mineral oil before bed ASPIRATION PNA |
|
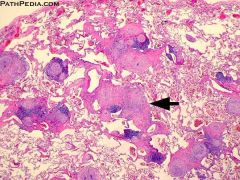
what is this
|
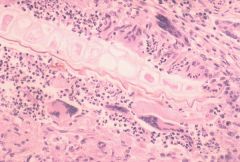
Aspiration pneumonia
Vegetable material in lung WILL STAIN WITH GMS WATCH OUT "Pulse granulomas" |
|
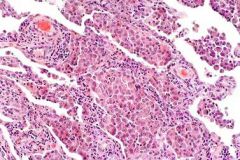
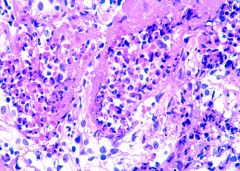
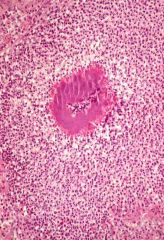
What is this
|
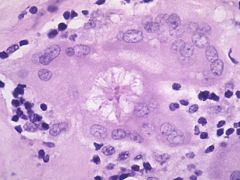
Asteroid body
Stellate inclusions in giant cells Classically seen in sarcoid but not specific |
|
What is this
|
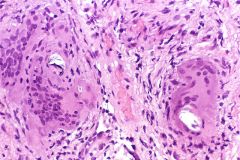
Schaumann Body
Laminated calcifications in granulomas Sarcoid but not specific |
|
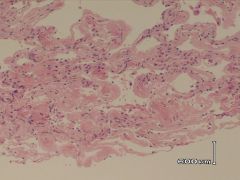
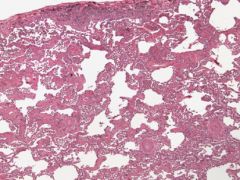
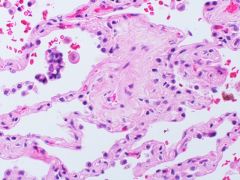
Ground glass opacities
|
Amyloid
|
|
|
Is AL or AA amyloidosis more common?
|
AL amyloidosis
"amyloid light chain amyloidosis" most commonly affects kidney Abnormal light chains come together to form deposits "BENCE JONES PROTEIN" when in blood or urine |
|
|
What is AA amyloidosis?
|
In AA amyloidosis, the deposited protein is serum amyloid A protein (SAA), an acute-phase protein which is normally soluble and whose plasma concentration is highest during inflammation.
It is therefore a complication of inflammatory diseases and infections, such as RA, ankylosing spondylitis, Crohn's, UC, Tb, bronchiectasis, chronic osteomyelitis, and the inheritable condition called familial Mediterranean fever. It can also be caused by HL and RCC. usually liver, spleen and kidney (can cause nephrotic syndrome) |
|
|
What type of amyloid is seen in Alzheimer's?
|
A-beta
|
|
|
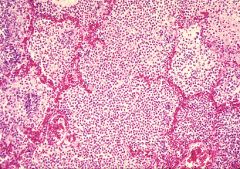
Sarcoidosis is mainly a bronchiolocentric lesion. T/F?
|
False.
Lymphangitic pattern |
|
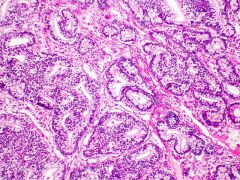
Patient with obstructive airways on clinical exam.
|
Asthma
Obstruction of the lumen of the bronchiole by mucoid exudate, goblet cell metaplasia, epithelial basement membrane thickening and severe inflammation of bronchiole. Smooth muscle hyperplasia EOS |
|

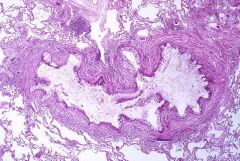
Process?
|
Bronchiectasis
Mucostasis & infection Bronchi are dilated, inflamed, and easily collapsible, resulting in airflow obstruction and impaired clearance of secretions |
|
Who gets bronchiectasis?
|
Many many causes
Patients with CF Kartagener syndrome |
|
|
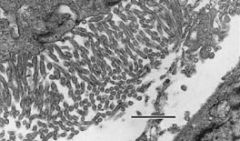
What is Kartagener syndrome?
Defect? |
AR
Immotile cilia syndrome / Primary ciliary dyskinesia PLUS situs inversus, bronchiectasis, chronic sinusitis Abnormal Dyenin arms of cilia |
|
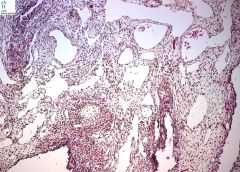
|
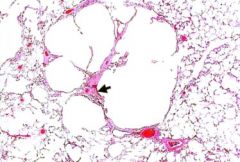
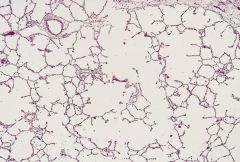
Centriacinar emphysema
Associated with smoking |
|
Defect?
gene? |
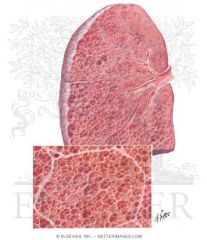
Panacinar emphysema
alpha-1-antitrypsin deficiency Entire acinus and entire lung involved Chromosome 14 PiMM: nl PiZZ: Poor px |
|
|
What is the Reid ratio?
|
Ratio of mucus gland:wall ratio
Used to dx Chronic bronchitis Nl is <0.25 |
|

|
Centriacinar emphysema
|
|
|
Panacinar emphysema
|
|
|
Fibrosing disease that leads to constrictive scarring of small airways?
|
Bronchiolitis obliterans
(NOT THE SAME AS BOOP) Associated with chr lung rejection, GVHD, connective tissue disease |
|
|
Asian patient with inflammation of terminal bronchioles and foam cell deposition
Treatment? |
Diffuse panbronchiolitis
(aka Japanese panbronchiolitis) Treatment with LOW DOSE MACROLIDE ANTIBIOTICS |
|
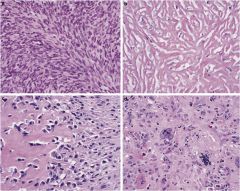
Lesion attached by pedical to pleura
stains? malignant features? |
Solitary Fibrous Tumor
Spindled HPC-like blood vessels CD34+ Malig: necrosis OR >4mits/10hpf |
|
|
Mesothelioma
Long microvilli |
|
Pleural based mass
|
Sarcomatoid mesothelioma
|
|
|
Types of mesothelioma
IHC? |
Epithelioid (60%)
Sarcomatoid (10%) Desmoplastic (5%) BIPHASIC (20%) +Calretinin, CK5/6, Vimentin, WT1, EMA - CEA, MUC31, BerEp4 |
|
|
Pulmonary hamartoma
|
|
ALK+
|
Inflammatory myofibroblastic tumor
aka: inflammatory pseudotumor |
|
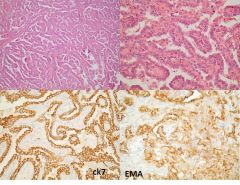
40year old female, incidental 2cm lung nodule
|
Sclerosing hemangioma aka "pneumocytoma"
Benign, well-circumscribed NOT a vascular tumor but thought to be Type2 pneumocytes Epith & stromal component, both stain with EMA but epith only with Cytokeratin, TTF1 |
|
|
Clear cell "sugar" tumor
PEComa HMB45+ PAS+ Simple excision DDx: clear cell carcinoma (RCC, etc) |
|
|
What lung tumors stain with TTF1?
|
Small cell (90%) (EVEN EXTRAPULMONARY!)
Adenoca (75%) Large cell (40%) Squamous (5%) |
|
|
Carcinoid vs atypical carcinoid
|
Both: organoid pattern, uniform nuclei, granular
chromatin. Atypical: Mitoses and some necrosis |
|
|
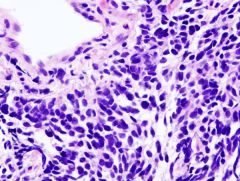
Small cell carcinoma
MOLDING Mitoses Necrosis LACK NUCLEOLI Azzopardi phenomenon Apoptotic cells TTF1+ |
|
|
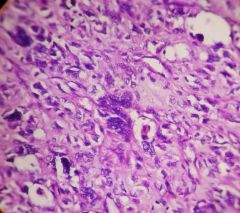
Large cell neuroendocrine carcinoma
Large cells, more cytoplasm, prominent nucleoli, numerous mitoses, and prominent necrosis. |
|
|
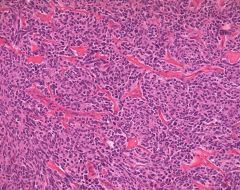
atypical carcinoid
|
|
|
atypical carcinoid
|
|
|
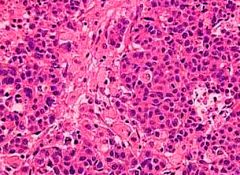
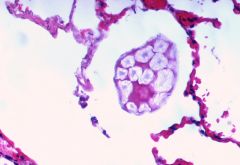
Carcinoid
|
|
|
What lung tumor is most closely related to smoking?
|
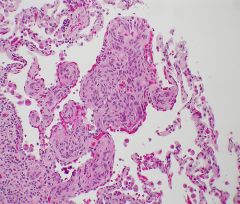
Squamous cell carcinoma
|
|
|
Which lung tumors are predominantly central?
|
Squamous cell carcinoma
Small cell carcinoma Carcinoid |
|

What is this called and how can these patients present?
|
Pancoast tumor
SMOKING HISTORY + APICAL LUNG MASS Horner's syndrome (compresses sympathetic ganglion) -Miosis, anhidrosis, ptosis Hoarseness from compression of recurrent laryngeal nerve SVC syndrome by compressing SVC leading to facial edema |
|
|
Epithelioid hemangioendothelioma
"LG epithelioid angiosarcoma" +CD31, CD34 |
|
What is this referred to and when is it seen?
|
Azzopardi phenomenon
seen in small cell ca ‘‘this deposition of DNA in the vessel wall is presumably the result of liberation of nucleic acids in large amounts from degenerating neoplastic tissue.’’ |
|
|
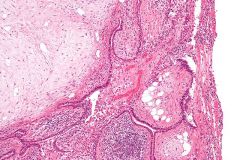
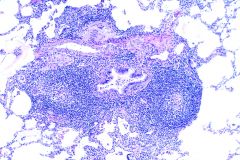
Follicular bronchiolitis
Germinal centers around airways Benign associated with collagen vasculitis diseases, immunodeficiency state, hyperimmune state, and hereditary factors |
|
IHC for large cells in this lesion?
|
EBV+ B cells
Lymphomatoid granulomatosis Looks like necrotizing granuloma but ghost-like blood vessels within granuloma, Tcell rich |
|
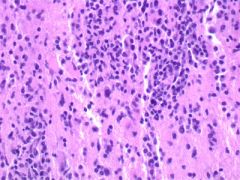
Grade this rejection in lung transplant
|
A3!
A1; Thin cuff A2: Thick cuff A3: Into interstitium A4: DAD |
|
Lung transplant. What is this?
|
Bronchiolitis obliterans
Most important complication to limit long term survival following lung transplantation. =CHRONIC AIRWAY REJECTION, GRADE C 45% overall 5 year survival rate |
|
|
What drug causes small granulomas that mimic hypersensitivity pneumonitis?
|
Methotrexate
|
|
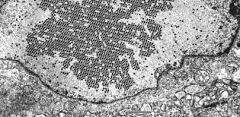
What drug causes foamy macrophages, scar tissue, and has lamellar bodies on EM?
|
Amiodarone
|
|
|
What drug causes bizarre hyperchromasia of type II pneumocytes?
|
Busulfan
|
|
|
What changes are seen with radiation?
|
Acute: DAD
Chronic: fibrosis; foam cells in intima of pulmonary vessels |
|
Premature baby
|
Hyaline membrane disease
Caused by lack of surfactant. Can lead to bronchopulmonary dysplasia if untreated |
|
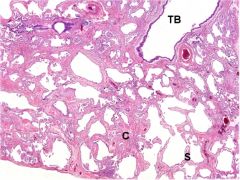
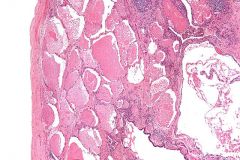
What type of CCAM?
|
CCAM2
Congenital cystic adenomatoid malformation Types 0-4 Type 2: uniform small cysts |
|
|
What are the types of CCAM?
|
0 Solid, diffuse. acinar agenesis. Cilia, cartilage, goblet cells.
1** MOST COMMON: large cyst with mucin or cartilage 2 uniform small cysts 3 solid bulky lesion with cuboidal small cysts (fetal alveoli) 4 multilocular large cyst, flattened epith. can look like pleuropulmonary blastoma. |
|
|
What tumor is least likely to cause a pulmonary effusion?
|
Squamous cell carcinoma
|
|
tumor in 30-year-old
|
epithelioid hemangioendothelioma
sometimes regarded as LG-angiosarcoma very rare |
|
|
a medical condition wherein a piece of tissue that ultimately develops into lung tissue is not attached to the pulmonary arterial blood supply
|
Pulmonary sequestration
|
|
|
Which is more common: intralobar or extralobar sequestration?
|
Intralobar (75%). Portion of lung that has systemic blood supply, but located within a normal lobe and does not have own pleura. Congenital vs acquired.
Extralobar (25%): Has own pleura. 80% MALE! Related to L hemidiaphragm. CONGENITAL |
|
Rare aggressive malignancy in adults
|
Pulmonary blastoma
biphasic malignant neoplasm occurring in adults that contains an epithelial component (usually fetal adenocarcinoma) and a sarcomatous component |
|
Cystic malignant lesion in kids < 4y
|
Pleuropulmonary blastoma is an aggressive tumor characterized by mesenchymal elements (including undifferentiated blastema and often cartilaginous, rhabdomyoblastic, or fibroblastic differentiation) and epithelium-lined spaces.
|
|
|
Pulmonary disorders that follow a lymphangitic pattern?
|
Sarcoid
Lymphoma Kaposi sarcoma Lymphangitic carcinoma LCH |
|
|
ABPA is which hypersensitivity type?
|
Type I
High IgE & periph eos! Eosinophilic pneumonia, granulomatous inflammation |
|
|
Dieterle stain for?
|
Legionella (causes bronchopneumonia and DAD)
|
|
|
Non-neoplastic mass lesion in lung, occurring posteriorly in lower lobes, from adhesion from parietal pleural plaque and visceral lung pleura.
|
Rounded atelectasis
Reinflates when adhesions are lysed pleural plaques are often result of asbestos exposure |
|
|
Parasites in lung
|
Strongyloides: can see larva, hemorrhage, neutrophils. Eggs NOT in lungs.
Paragonimus: worms & eggs in lung Echinococcal cyst: THICK walled, multi-lamellated Cryptosporidia: epithelial Dirofilariasis: dog heartworm; dead parts embolize to lung. |
|
|
Panbronchiolitis histology?
|
Peribronchiolar interstitial macrophages
JAPANESE treat with macrolides |
|
|
Lung changes in scleroderma?
|
Pulmonary HTN
NSIP or UIP patterns |
|
|
Lentil! legume aspiration. Can form "pulse granuloma"
|
|
|
Minute pulmonary meningothelial-like nodule of the lung
aka chemodectoma small, 1-3mm, can be multiple, incidenta, women EMA+ |