![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
31 Cards in this Set
- Front
- Back

|
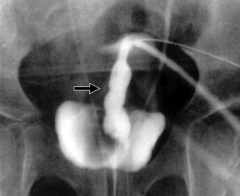
Bifid Ureter
*asymptomatic unless one kinks to cause an obstruction that can lead to hydronephros |
|

|
Extrophy of Bladder
*ant abdominal wall and bladder fail to close *Increased risk of colorectal & bladder cancer |
|

let's just say that his aim isn't the best |
Hypospadia
*urethra opens on ventral side of penis |
|
When this kids laughs, he pees out his belly button... how's that for a party trick! |
Persistent Urachus
*embryologically functions to connect bladder to allantois *risk of transforming into Primary Urachal Adenocarcinoma!!! |
|
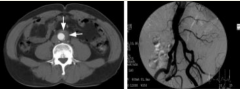
Pt found to have a clonal proliferation of IgG4 producing plasma cells |
Ormond's Disease (primary sclerosing retroperitoneal fibrosis)
*clonal cells produce pseudotumors of fibrosis that obstruct vasculature and ureters |
|

|
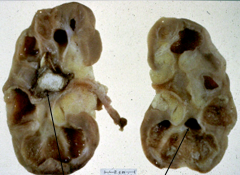
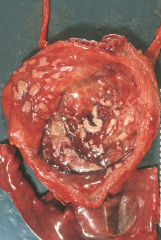
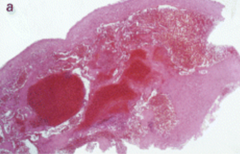
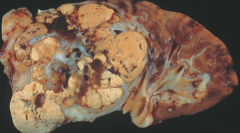
Hydronephrosis due to chronic obstruction
*cortex is atrophied and calyxes are dilated |
|
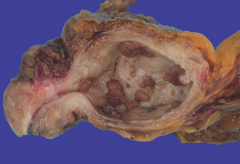
What infection did this pt most likely have? |
Proteus Infection (struvite stones associated w/) |
|
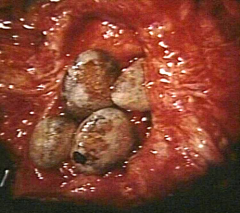
What is this pt at an increased risk of? |
Chronic Cystitis - bladder stones prevent complete voiding causing an increased risk of infection |
|
Pt has skunky urine & brown/curdeled ejaculate. What are they at increased risk of? |
Squamous cell carcinoma of bladder (pt has Schistosomiasis) |
|
|
Malacoplakia
*chronic cystitis in pt w/ macrophage defect causing plaques comprised of sheets of macrophages to form |
|
|
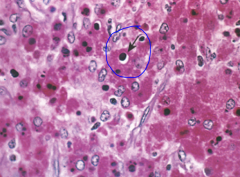
Michaelis-Gutman Bodies in Malacoplakia |
|
|
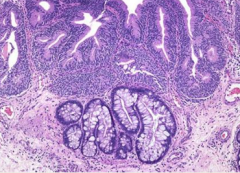
Cystitis Glandularis
*chronic cystitis w/ benign metaplastic changes of cysts lined w/ either urothelium or intestinal epithelium |
|
nodule found in bladder |
Polypoid Cystitis
*due to chronic irritation from indwelling catheter |
|
found on posterior lip of urethra |
Carbuncle
*benign, common after menopause, trx w/ drainage |
|
|
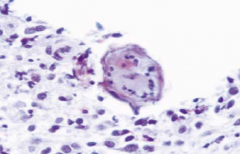
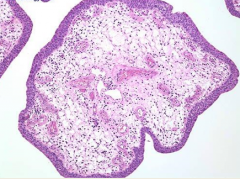
Urothelial Carcinoma - Papillary morphology |
|
|
Low Grade Urothelial Carcinoma
*typically papillary morphology, increased but normal mitoses |
|
|
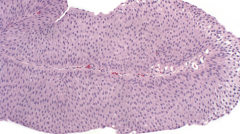
High Grade Urothelial Carcinoma
*usually flat morphology, atypical nuclei and mitoses |
|
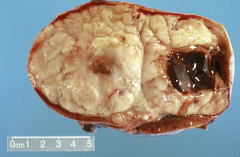
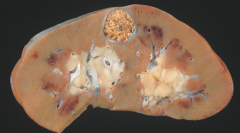
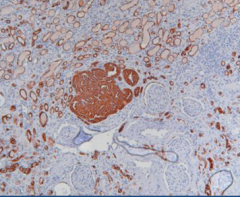
taken from kidney of a 4-year-old |
Wilms tumor (nephroblastoma)
*most common renal tumor in kids *mass will be large, solitary, tan, well-circumscribed |
|
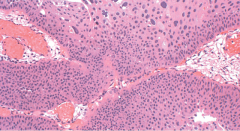
taken from a kidney mass in a 4-yr-old |
Wilms tumor (nephroblastoma)
*Blastema (sheets of small-blue cells), spindle stroma, immature tubules |
|
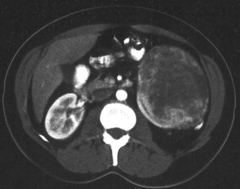
What triad of symptoms is this pt most likely experiencing? |
(Renal cell carcinoma) 1. Costovertebral pain 2. Palpable Mass 3. Microscopic Hematuria
(possible polycythmia due to paraneoplastic syndrome) |
|
What's the #1 risk factor for this condition? |
(Renal Cell Carcinoma)
SMOKING!!! |
|
How does this mass spread? |
(Renal Cell Carcinoma)
Via the veins (bypasses lymph nodes) |
|
taken from kidney mass |
Clear Cell Renal cell carcinoma
*most common subtype *due to deletion of VHL gene of short arm of chromosome 3p |
|
|
Chromophobe Renal Cell Carcinoma
*arise from CD *good prognosis |
|
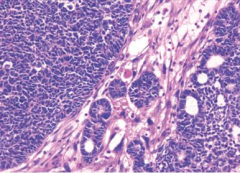
|
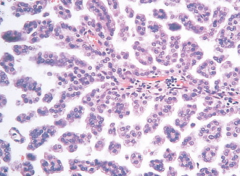
Papillary Renal Cell Carcinoma
*arises from CD |
|
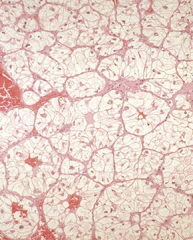
Mass is >0.5 cm |
Papillary Carcinoma
(if it were <0.5cm it would have been an adenoma) |
|

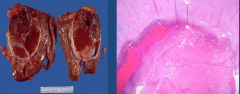
|
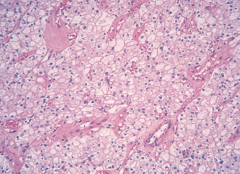
Renal Oncocytoma
*Benign, Mahogany brown w/ central scar *cells have pale granular cytoplasm full of mitochondria |
|

|
Angiomyolipoma
*bilateral tumor comprised of fat, blood vessels, and smooth mm |
|

What mutation causes this? |
(Angiomyolipoma)
*loss-of-fxn mutation in TSC1 or TSC2` |
|
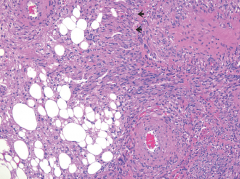
What condition is this associated with? |
(Angiomyolipoma)
*Tuberous Sclerosis |
|
|
Cystic Renal Carcinoma
*arises from benign renal cysts |