Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
33 Cards in this Set
- Front
- Back
|
What is the general response of the lymph nodes to injury?
|
Cells of the monocyte-macrophage system are the first line of defense against noxious agents. As most of these agents arrive in the afferent lymph, the sinus macrophages (histiocytes) are the first to respond. This is evidenced by an increase in their number (so-called sinus histiocytosis) in the subcapsular, trabecular, and medullary sinuses. Additional inflammatory cells (e.g. neutrophils & monocytes) arrive in the blood and migrate to the parenchyma or into the sinuses.
Also antigens from incoming material will be presented to cells of the germinal centers, which will produce immunoblasts that migrate to the medullary cords, mature into plasma cells, and secrete a specific antibody. The concentration of plasma cells in the medullary cords correlates with the activity of the germinal center. The T lymphocytes also respond to injury by a limited degree of proliferation in the paracortical areas: T cell response in the paracortex is caused by stimuli that trigger the cell mediated immune response Molecules enter one of 2 ways: in the incoming lymph delivered by the afferent lymphatics to the subcapsular sinus or via the arterial blood supply. |
|
|
|
|
|
|
What causes reactive hyperplasia? What does it look like grossly? Histologically? Why does the lymph node enlarge?
|
What: response to chronic antigenic stimulation, in general in the organ they drain
GROSS: Enlargement of the node(s) = lymphadenopathy -may bulge on cut section HISTO: -proliferation of lymphoid follicles with prominent germinal centers +/- increased plasma cells in the medullary cords -tingible-body macrophages & dendritic cells containing nuclear debris of B cells which undergo apoptosis if they fail to produce antibody with high affinity for the antigen -proliferation of macrophages in the medullary sinuses, which are dilated and can be filled with fluid |
|
|
What are the different zones in secondary follicles?
|
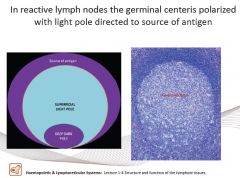
Dark zone - contains proliferating blastlike B cells
Light zone - composed of B cells with irregular of cleaved nuclear contours |
|
|
What causes atrophy of lymph nodes?
|
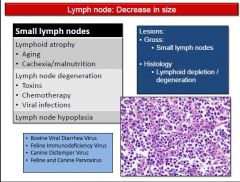
Lack of antigenic stimulation, cachexia, malnutrition, aging, and viral infections
|
|
|
What causes necrosis of the lymph node? What does it look like grossly? histologically?
|
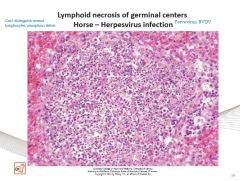
-consists of lysis of cells of lymphoid follicles
Causes: targeted necrosis of lymphoid tissue (lymph nodes, thymus, white pulp of spleen), occurs in foals affected with Equine Herpes virus. In the peyers patches of ruminants infected with BVDV In peyers patches of dogs infected with parvovirus *these viruses target cells of highly proliferative tissue compartments such as lymphoid tissue HISTO: characterysed by lymphocytolysis (lysis/fragmentation of lymphocytes), with abundant karyorrhexis (fragmentation of the nucleus) GROSS: lymphoid necrosis is not visible |
|
|
What can cause pigmentation in lymph nodes & what sort of discoloration occurs?
|
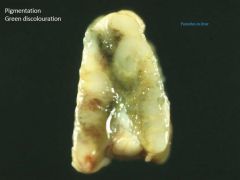
Melanin - e.g. chronic dermatitis → brownish
Haemosiderin & Hematin → brownish Carbon pigment can accumulate in the tracheobronchial lymph nodes with pulmonary anthracosis → black Eosinophilic inflammation → green discoloration |
|
|
What is lymphadenitis? What causes it? What does Acute lymphadenitis look like grossly? Histo? What are some examples of causes?
|
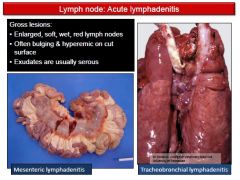
Lymphadenitis - is inflammation of the lymph nodes; the infectious agent is present in the lymph node (in reactive hyperplasia the node is immunologically reactive but free of local invasion). Lymphadenitis is the result of a regional lymph node draining and inflammatory site that has become infected.
ACUTE LYMPHADENITIS GROSS: enlarged, soft, wet, red lymph nodes -often bulging & hyperemic on cut surface -exudates are usually serous -associated engorged lymphatics or lymphangitis HISTO: neurophils & bacteria in cortical areas and medullary sinuses Cause: usually result of a regional lymph node draining site of inflammation EXAMPLE: Infection of tracheobroncheal lymph nodes in pneumonia - all species |
|
|
What is an example of Chronic suppurative lymphadenitis (lymph node abscess) in horses? What does it look like?
|
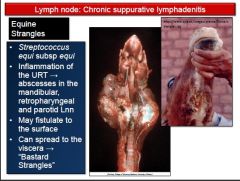
Streptococcus equi (strangles) - primary infection of the respiratory tract (nasopharyngitis, presenting with nasal discharge). Lymph nodes are involved early in the course of the disease (mandibular, parotid, & retropharyngeal lymphadenitis)
GROSS: enlarged & oozing creamy pus on cut surface |
|
|
What is an example of Chronic suppurative lymphadenitis (lymph node abscess) in pigs? What does it look like?
|
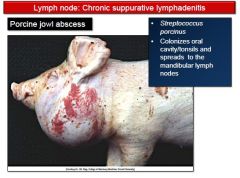
Streptococcus procinus (jowl abscess in swine) - the agent colonizes the oral cavity and tonsils and spreads to the regional lymph nodes
|
|
|
What is an example of Chronic suppurative lymphadenitis (lymph node abscess) in sheep? What does it look like?
|
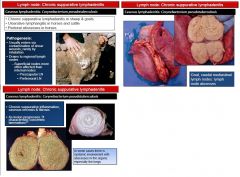
Corynebaterium pseudotuberculosis (pseudotuberculosis or caseous lymphadentisis) - mostly sheep, following wound infection (e.g. tail docking) followed by spreading to regional lymph nodes
GROSS: large abscesses with concentric lamellation (onion-like) due to progressive necrosis and reformation of the capsule. Can also occur in the spleen and lung, after spreading from LN |
|
|
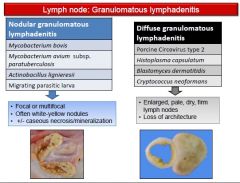
How do nodular vs diffuse chronic granulomatous and pyogranulomatous lymphadenitis look different grossly?
|
|
|
|
Provide an example of NODULAR granulomatous/pyogranulomatous lymphadenitis
|
Actinobacillus ligneresii (wooden tongue) - inflammation of the tongue and involvement of regional lymph nodes
Mycobacterium avium paratuberculosis (Johnes disease) - granulomatous enteritis with involvement of mesenteric lymph nodes |
|
|
Provide an example of DIFFUSE chronic granulomatous and pyogranulomatous lymphadentis
|
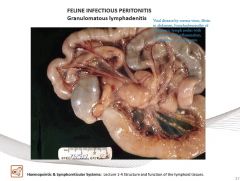
●Feline Infectious Peritonitis - granulomatous lesions in various organs, including eyes, CNS, intestine
-mesenteric lymphadenopathy with granulomatous inflammation is a common feature -lesions are also commonly found in the lymph node at the ileocecal junction ●Porcine circovirus-2 - agent of postweaning multisystemic wasting syndrome (PMWS) GROSS: Diffuse enlargement of the mesenteric lymph nodes HISTO: Granulomatous infiltration of the node with large botryoid intracytoplasmic viral inclusions |
|
|
What is the difference between lymphoma and leukemia?
|
Lymphoma - encompases malignancies in lymphoid tissues OUTSIDE the bone marrow
Leukemia - tumors arrising IN the bone marrow |
|
|
Is it only lymphoid organs that develop lymphoma?
|
NO! Vitually every organ containing lymphocytes can develop a primary lymphoma (intestine, heart etc....) BUT it occurs most frequently in primary and secondary lymphoid organs
|
|
|
How do we classify lymphomas?
|
●Anatomic location - multicentric, alimentary, mediastinal/thymic, other
●Immunophenotype - B lymphocyte vs. T lymphocyte vs. non-B/non-T ●Cellular morphology - size, nuclear features, mitotic rate ●Histologic pattern - diffuse vs. follicular ●Biologic behavior - firm low-grade (indolent) to high-grade (aggressive) tumors |
|
|
How does lymphoma look histologically? What classifies a low grade lymphoma vs. a high grade one?
|
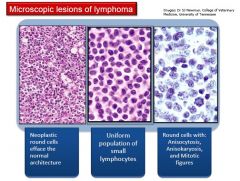
It is characterized by:
-a loss of tissue architecture -infiltration of tissues by large amounts of round cells arranged in sheets NOTE: lymphomas of small, well differentiated cells with low mitotic rate are low-grade, whereas lymphomas of large, poorly differentiated lymphocytes (blasts) with high mitotic rate are high-grade |
|
|
What is the gross appearance of lymphoma in multicentric lymphoma, the spleen & liver, thymic lymphoma, and renal lymphoma?
|
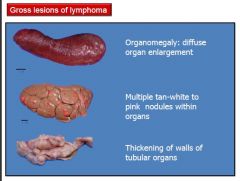
Multicentric lymphoma - enlarged lymph nodes that bulge on cut section and are gray-white to light tan or reddish
-in advance cases, normal architecture distinction between the cortex and medulla is obliterated Spleen & Liver - infiltration can result in diffuse enlargment or nodules Thymic lymphoma - large, gray, soft mass in the cranial mediastinum Renal lymphoma - often affects both kidneys and is evident as bilateral diffuse organomegaly |
|
|
How do we diagnose lymphoma?
|
-often suspected on the basis of organomegaly (e.g. generalized lymph node enlargement) or abnormal ultrastructural findings (e.g. thickened intestines with abnormal echogenicity)
-initial diagnosis typically is made based on aspiration cytology, biopsy and/or histopathology, or both, of the affected organs -the type of tumor and extent of the disease may be characterized further by immunophenotyping and clinical staging -immunophenotyping is done to determine whether a tumor is of B-lymphocyte or T-lymphocyte origin (this distinction cannot be made reliably based on routine staining) -clinical staging includes examination of aspirates of bone marrow and other enlaged organs (e.g. spleen, liver, and other lymph nodes) |
|
|
What are the clinical signs of lymphoma?
|
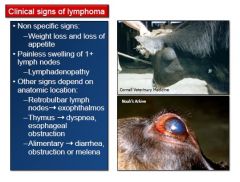
-hypercalcemia is often associated with lymphoma due to production of parathyroid hormone related peptide (PTH-rP) by neoplastic cells
-occurs in 20% of lymphomas in dogs -hormone increases serum calcium levels by increasing calcium release from bone, enhancing resorption of calcium in the kidneys, and stimulation of absorption of calcium in the intestine -such paraneoplastic hypercalcemia (humopral hypercalcemia of malignancy) may lead to pathologic calcification and related complications (e.g. renal failure) |
|
|
DOGS, how common is lymphoma? What form is more common? What are the clinical signs?
|
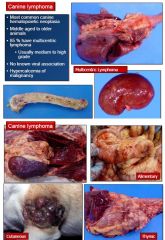
-common, represents 7-9% of all malignancies and the large majority of hematopoietic malignancies
-no retroviral cause -disease of middle-aged to older dogs -MC is multicentric lymphoma (80-85% of all cases of canine lymphoma) with PROMINENT lymph node involvement -approx 80% are intermediate- or high-grade tumors -other less common forms (in decreasing order of frequency) are alimentary, cutaneous forms (mycosis fungoides or epitheliotropic T cell lymphoma), mediastinal (thymic) and sporadically occuring forms in virtually every concievable location -70-80% are of B-lymphocyte origin Clinical signs: may be referable to the specific organ systems affected, but are usually absent or non-specific when lymphoma is first diagnosed -approx 15% of dogs with lymphoma, and 40% with mediastinal lymphoma are hypercalcemic -splenic and hepatic involvement is common in cases of canine multicentric lymphoma |
|
|
What are the most common forms of lymphoma in cats?
|

Feline Leukemia Virus (FeLV) causes lymphoma in cats in 10-20% of cases
-the lymphoma is likely to develop at a younger age, and cats are more likely to develop certain types of lymphoma - especially mediastinal and multicentric T-lymphocyte forms -than FeLV negative cats -at present approx 80-90% of cats with lymphoma are FeLV-negative, and the majority of lymphoma cases are the alimentary form -mediastinal and multicentric forms, all though less common now, are still more likely to occur in younger cats, whereas the alimentary form typically develops in older cats (>10 years of age) -the neoplastic cell type also tends to vary by anatomic location -alimentary lymphoma in cats is predominantly a B-lymphocyte disease, whereas mediastinal lymphoma is predominantlu a T-lymphocyte disease -leukemia and bone marrow involvement are common in all forms -most cats die within 8 weeks if untreated CLINICAL SIGNS: nonspecific e.g. weight loss, anorexia |
|
|
What are the most common forms of lymphoma in horses and how common is lymphoma in these animals?
|
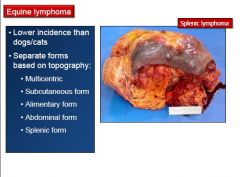
-uncommon in horses, represents <5% of all neoplasms
-multicentric lymphoma is the most common form, and alimentary (involves upper small intestines & regional lymph nodes), cutaneous, and other forms may also occur -most are of intermediate of low-grade |
|
|
What is enzootic bovine lymphoma? What age does it occur & what is it associated with?
|
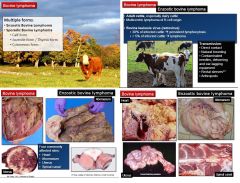
ENZOOOTIC BOVINE LYMPHOMA
-primarily a multicentric B-lymphocyte disease of adult cattle (5-8 years old) and is strongly associated with BLV infection and BLV related persistent lymphocytosis -approximately 30% of cattle infected with BLV develop non-neoplastic persistent lymphocytosis, and of these, less than 5% develop lymphoma -BLV is a retrovirus that persists within lymphocytes for the life of the infected animal -transmission of the virus is mostly horizontal due to transmission of infected lymphocytes as opposed to free virus in secretions via arthropods, natural breeding, and accidentral transmission by needles, ear tagging equip etc. -more common in dairy cattle -involves other location in addition to the lymph nodes: abomasum, vertebral canal, kidney, heart (right atrium), and uterus -enlargement of the superficial lymph nodes is common, and enlarged pelvic and abdominal lymph nodes are often found on rectal palpation |
|
|
What is spooradic bovine lymphoma? What types do we have & what ages do they occur?
|

SPORADIC BOVINE LYMPHOMA
The thymic form is characterized by large cranial thoracic and lower cervical masses, respiratory distress, and weight loss in cattle <2 years of age The sporadic multicentric form is characterized by disseminated disease in claves 3-6 months of age. Affected calves have widespread lymph node enlargment in addition to hepatic, splenic, and renal involvement. Marked blood and bone marrow involvement may occur. The cutaneous form is rare, occurs in young cattle, and consists of discrete cutaneous plauqes or large scabby lesions. |
|
|
What kind of lymphoma is common in pigs? How common is it?
|
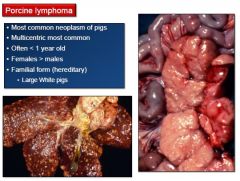
Lymphoma is the most commonly reported malignancy in pigs and may be more likely to affect females rather than males
-multicentric lymphoma is the most common form of the disease in pigs -lymph node enlargement is more common in visceral than peripheral nodes -lymphoma often affects animals <1 yea of age, and the mediastinal form of lymphoma tends to affect younger pigs more commonly than the multicentric form |
|
|
What metastatic tumors can occur in lymph nodes?
|
●Carcinomas (via lymphatic vessels)
●Mast cell tumors. High grade mast cell tymors can metastasize to the regional lymph nodes ●Soft tissue sarcomas (rarely metastasize, via hamtogenous route) |
|
|
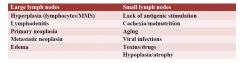
What differential diagnoses do we have for large and small lymph nodes?
|
|
|
|
What is lymphedema? What can cause it?
|
Lymphedema is feined as swelling of a part of the body by an increased quantity of lymph due to a lymphatic system disorder. It can be primary (congenital) or secondary, from obstruction due to inflammation or neoplasia
|
|
|
What is lymphangectasia? What is the cause?
|
Lymphangectasia is the dilation of a normally developed lymphatic vessel, and almost invariably results from some form of obstruction that leads to the accumulation of excess interstitial fluid in the drainage area. Intesinal lymphangectasia (protein loosing enteropathy) is the most common form; it is also commonly associated with Johnes disease
|
|
|
What is chylothorax? What is the cause?
|
Chylothorax is the result of leakage or rupture of the thoracic duct. Causes of chylothorax include neoplasia and right sided CHF.
|
|
|
What is lymphangitis? What is the cause?
|
Lymphangitis can occur when lymphatic vessels rupture and release their content in the extracellular space. Lymphangitis with anatomic specificity is also a prominent feature of some specific diseases: bovine farcy, sporadic lymphangitis in horses, ulcerative lymphangitis in horses (Corynebacterium pseudotuberculosis) and epizootic ymphantitis in horses and mules (Histoplasma capsulatum var. farciminosum)
|