![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
89 Cards in this Set
- Front
- Back
|
LC 2.2 Give the definition of puberty |
- reaching of sexual maturity, stage of gonad development where reproduction become possible, secondary sexual characteristics are shown and growth spurts |
|
|
LC 2.2 Give the basic order of events in puberty in girls |
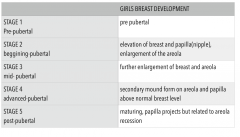
- breast bud forms - pubic and auxiliary hair starts to form - growth spurt - menarche - adult pubic hair - adult breast |
|
|
LC 2.2 Give the basic order of events in puberty of boys |
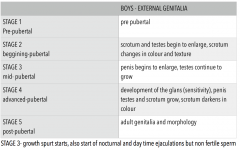
- testicular growth - growth of pubic and auxiliary hair - growth spurt - spermarche - adult morphology of external genitalia - adult pubic hair |
|
|
LC 2.2 List the tanner stages of male external genitalia growth |
|
|
|
LC 2.2 List the tanner stages of female breast development |
|
|
|
LC 2.2 What is the first hormonal initiating puberty? |
- pulsatile release of GnRH from hypothalamus |
|
|
LC 2.2 What chemical is thought to induce GnRH pulsatile release in starting puberty |
Kiss-peptin- 1 |
|
|
LC 2.2 In early puberty what is the general pattern on FSH release |
- pulsatile release of FSH during sleep - as time goes on pulses become large but difference between night and day decreases - LH release in girls is about a year after FSH release |
|
|
LC 2.2 What are thought to be the triggers/control when puberty starts? |
- genetics - environment - prime body weight / nutrition |
|
|
LC 2.5 What hormones cause bone growth? |
Oestrogen and pulsatile Growth hormone release |
|
|
LC 2.5 What part of the bone allows cell division for growth and where is it located? |
- the functional growth plate is the part of cell which has the ability to divide - This is located between the metaphysis (main body of body and the epiphysis (end of bone) - integrity of this growth plate determines if growth is possible |
|
|
LC 2.5 What are the 6 main areas of social and psychological development in puberty? |
1 - parental relationship 2 - autonomy vs dependancy 3 - identity 4 - relation to peers 5 - sexuality 6 - risky behaviour , try new experiences |
|
|
LC 2.3,4 What are the main functions of skin? |
- protection - UV light, immunological, waterproof - metabolism - vit D3 from cholesterol - thermoregulation - sweat, hairs , shivering - excretion - alcohol , spices - sensation - communication - sexual behaviours EG flush, with doctor EG jaundice |
|
|
LC 2.3,4 what are the layers of the epidermis and how are they specialised for function? |
OUTERMOST - stratum corneum - mainly keratin fibres, act as barrier and account for elasticity of skin - stratum granulosum - keratinocytes starting to lose nuclei, granules more to top of cell and provide waterproofing - stratum spinosum - prickle cell layer , aid flexibility of skin - stratum germinatum - basement membrane of dividing cells, basement ridges provide friction so sticks to dermis - this creates finger print pattern |
|
|
LC 2.3,4 What are the 2 sections to the dermis? what does the dermis contain? |
papillary dermis = upper layer reticular dermis = lower layer contains: sweat gland, sebaceous gland , subcutaneous fat , hair follicle, blood supply |
|
|
LC 2.3,4 Give an example of regional variation in epidermis and dermis |
Hands and feet : thick epidermis and thin dermis Back: thin epidermis and thick dermis |
|
|
LC 2.3,4 What are the two different types of sweat glands are what are the differences between them? |
Eccrine - isotonic secretion on to surface of skin Accrine - secrete on to hair follicle, in humans only found on side of nose, genitalia and armpits |
|
|
LC 2.3,4 What cells cause the pigmentation in skin? Where do these cells originate/develop from? How do they cause pigmentation |
-Melanocytes - develop from neural crest cells - melanocytes releases melanosomes containing melanin, melanosomes surround ketatinocytes (1 melanocyte every 5-10 keratinocytes) |
|
|
LC 2.3,4 How is a mole formed? |
proliferation of melanocytes |
|
|
What are the 2 types of melanin? Which is better at protecting for UV light? |
Eumelanin and pheomelanin Eumelanin is better at protecting for UV light rays as darker |
|
|
LC 2.3,4 What is vitaligo? |
autoimmune destruction of melanocytes causing local depigmentation |
|
|
LC 2.3,4 What is melasma? |
- gradual depigmentation of skin over time |
|
|
LC 2.6 What type of epithelium secrete milk in breast tissue? |
cuboidal |
|
|
LC 2.6 Describe the micro-anatomical arrangement of breast tissue |
Each lactiferous ducts stems from a lobe of breast tissue. Within each lobe of breast tissues there are lobules which are from the tertiary (terminal) ductules. lobes n lobules contain the subcutaneous fat that surround them. between lobes and lobules there is dense cognitive tissue known as the suspensory ligaments of cooper at the end of each ductules there are alveoli of cuboidal epithileum surrounded by myoepithelial cells which can undergo peristalsis to aid lactation. each lobule proliferates during late stages of the menstrual cycle and pregnancy |
|
|
LC 2.6 Describe the embryological primary bud growth of the breast tissue |
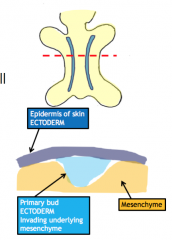
2 lines of ectodermal tissue form on the ventral side of the foetus - called milk lines proliferation of tissue here form ridge into underlying mesenchyme (*which differentiates to form underlying connective tissue of skin) Most of milk line will degenerate except for in mid thoracic region - in normal location of breast |
|
|
LC 2.6 How many secondary breast buds form? what is shown of surface at this stage of development? what do secondary buds develop into? |
15-20 mammary pit (indent on surface showing location of underlying breast development) lactiferous ducts **SAME IN MALE N FEMALE TO THIS POINT |
|
|
LC 2.6 What is it called where you have super numary nipples? what is it called where you have multiple formations of breast tissue (no nipple)? Where are these usually located and why is it that they form? |
- Polytheilial - Polymastia - fail in regression of milk line, 7-10cm down from normal breast tissue along milk line |
|
|
LC 2.6 Describe the lymphatic drainage of the breast What can this be used as/indicate clinically |
3 levels of nodes, first drains through level 1 nodes then level 2 ECT 13 Level 1 nodes - anterior axillary 5 level 2 nodes - lateral axillary 2-3 level 3 nodes - central axillary - can indicate the spread/progression of breast cancer |
|
|
LC 2.7 What is the difference between primary and secondary amenorrhea? |
PRIMARY - periods have never started SECONDARY - used to have periods before they stopped |
|
|
LC 2.7 What are the different types of "inconvenient bleeding" disorders in the menstrual cycle? |
Menorrhagia - excessive blood loss - v heavy metrorrhagia - periods last too long ( >7 days) polymenorrhea - cycles to short (<21 days) oligomenorrhea - cycles too long (>32 days) irregular menses - no regular cycle |
|
|
LC 2.7 what are the likely causes of inconvenient bleeding disorders of menstrual cycle? |
- idiopathic - fibroids - benign grown in myometrium of uterus - polyps - being growth in endometrium of uterus - endometrium hyperplasia - over growth of tissue - hormones |
|
|
LC 2.7 Which bleeding conditions of the menstrual cycle are considered suspicious? |
- intra-menstral - post coital - post menopausal |
|
|
LC 2.8,9 Describe the peritoneal covering of the rectum |
upper 1/3 = anterior and laterally middle 1/3 = anterior only lower 1/3 = no covering |
|
|
LC 2.8,9 What are the 5 lobes of the prostate? which enlarges in BPH? |
anterior, posterior, middle, x2 lateral * posterior and lateral are kind of same lobe bit weird middle lobe enlarges in BPH - benign prostatic hyperplasia |
|
|
LC 2.8,9 What ligament connects the bladder to the anterior abdominal wall? |
medium umbilical ligament |
|
|
LC 2.8,9 Describe the relationship between the ureter and vas deferens |
"bridge over water" the vas deferens loops over the ureter |
|
|
LC 2.8,9 instead of the lobar model of the prostate what can be a more usful model clinically? |
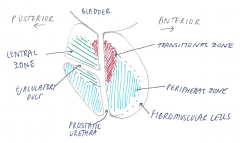
zone model - central zone (BPH) - peripheral zone (70% of prostatic cancers) - transitional zone (20% prostatic cancers) - fibromusclular zone |
|
|
LC 2.10,13 What is the origin of the male pudendal nerve and what is its path and branches? |
originates from S 2, 3, 4 exits above sacro-spinous ligament (greater siatic formen and reenters pelvis under the sacrospinous ligament (lesser siatic foramen) 1st branch is inferior rectal nerve (motor output and sensory input from anus and surrounding skin 2nd branch is posterior scrotal never (sensory input) 3rd branch is the multiple perineal branches which cover the rest of the perineum including the dorsal nerve of the penis * blood supply matches pudendal nerve course |
|
|
LC 2.10,13 in the male what glands lie lateral to the urethral opening in the perineal membrane? |
bulbo-urethral glands (cowpers) |
|
|
LC 2.10,13 Describe the anatomy of the origin of the penis |
bulbospongiosum muscle attaches to the bulb of the penis on the perineal membrane the ischiocavernosum muscles join to the crura, section of perineal membrane medial to ischial pubic bone bulbospongiosum muscle extends to the corpus spongiosum and the ischiocavernosum muscles extend to become the corpus cavernous muscles, together these 3 muscles make the free body of the penis |
|
|
LC 2.11 What are the 4 male androgen hormones and how potent is each? |
testosterone - 50% (5 alpha) dihydrotestosterone - 100% androstenedione - 8% dehydroepiandrosterone (DHEA) - 4% |
|
|
LC 2.11 Explain the progression of testosterone production in the leydig cell, starting with cholesterol |
cholesterol > pregnenalone > DHEA > (only some) androstenediol remaining DHEA > androstenedione androstenediol > testosterone by 3-beta-hydroxy-steroid-dehydrogenase (HSD) androstenedione can be converted to testosterone by 17 beta HSD |
|
|
LC 2.11 Inside the sertoli cells what enzymes can act on testosterone what will be the products of each reaction? What protein can prevent this? |
testosterone (or androstenedione) can be acted on by aromatase - produces estradiol (or estrone) testosterone can be acted on by 5-alpha-reductase to form DHT (dehydrotestosterone) 5alpha-reducatse action prevented by androgen binding protein (ABP) binding to testosterone |
|
|
LC 2.11 how is testosterone concentration maintained high in sertoli cell? why is this important? |
ABP and low concentration of aromatase enzymes because need high concentration of testosterone for spermatogenesis |
|
|
LC 2.11 What % of testosterone is circulating as free testosterone? what % and in what form is the rest circulating? |
2% free 60% bound by SHGB 38% albumin bound |
|
|
LC 2.11 What tissues does testosterone itself act on (without being converted to DHT or oestrogen)? |
RBC liver muscle abdominal fat bone larynx (+sertolli cells) |
|
|
LC 2.11 what is the majority of testosterone metabolised to? how is it mainly excreted? |
17-ketosteroids in urine and water soluble ** 2% of excreted testosterone is unchanged, but this is not representative of testosterone in blood |
|
|
LC 2.11 What cells does LH act on? what cells does FSH act on? What does it cause the production of in each? What are the effects of the product on the hypothalamic pituitary axis? What type of g protein receptor do they act on? |
LH > leydig - testosterone FSH > sertoli - inhibin B - negative feed back on ant. pituitary and hypothalamus - act on Gs protein bound receptor, using second messenger cAMP to activated enzyme transcription |
|
|
LC 2.11 clinically what is inhibin B used to indicate |
testosterone function |
|
|
LC 2.12 What is the path of sperm from seminiferous tubule to the outside world? |
seminiferous tubule > rete testis > efferent ductule > epididymis > vas deferens > ejaculatory duct > prostatic urethra > membranous urethra > penile urethra |
|
|
LC 2.12 What epithelium are shown in the epididymis and in the vas deferens? |
EPIDIDYMIS = tall columnar VAS DEFERENES = ciliated |
|
|
LC 2.12 what are the layers of the scrotal sac? |
skin dartos muscle colles fascia tunica vaginalis mesothelial cells tunica albugina tunica vasculosa (on outer edge of lobule) |
|
|
LC 2.14,15 What are the glands located on the inferior edge of the bulb of vagina called? |
greater vestibular glands |
|
|
LC 2.14,15 what muscles sit on the crura of the vagina? what do they join to form? what does this extend to? |
ischiocavernosum muscles join to form the body of the clitoris extends to become the glans clitoris |
|
|
LC 2.14,15 What 3 muscles help control continence in the deep perineal space/pouch? describe their position |
- compressor urethral muscle , lies over the urethra like a sheet/rod and can flatten it - external urethra sphincter - ring around the urethra - spincter urethrovaginalis - ring muscle from perineal body around the vaginal entrance |
|
|
LC 2.14,15 What is the main muscle in females that controls urinary continence? what muscle group does it belong to? how does it do this? |
pubovaginalis levator ani changes the angle between the urethra and bladder, upon relaxation the angle becomes more flat so urine is able to flow |
|
|
LC 2.14,15 Describe the path of the pudendal nerve from its origin to its 3 main branches in females |
exits S2,3,4 and exits pelvis through greater siatic foramen and re-enters through the lesser siatic foramen 1st branch is the inferior rectal never to anús 2nd branch is posterior labial nerve 3rd branches are for the perineal |
|
|
LC 2.16 What are the 4 phases of the male sex response? |
1 - desire 2 - arousal 3 - orgasm 4 - resolution |
|
|
LC 2.16 What are the excitatory and inhibitory neurotransmitters/hormones for the desire phase of the male sexual response? |
EXCITATORY : dopamine, oxytocin, testosterone INHIBATORY : serotonin |
|
|
LC 2.16 What chemicals mediate the muscle relaxation allowing a erection? |
nitric oxide release activates granulate cyclase which causes cGMP production, cGMP causes reduction in intracellular Ca2+ concentration in corpus cavernous muscles, allows increased inflow from pudendal artery |
|
|
LC 2.16 What sphincters are opened/closed during ejaculation? what muscles contract? what nervous system does this? |
sympathetic nervous system preprostatic urethral sphincter closes urethral sphincter opens pelvic floor muscles and ejaculatory duct SMa nd seminal vesicle SM contract |
|
|
LC 2.16 What is priapism? what are the two types? what is the difference between them? **HINT related to male sexual dysfunction |
- persistence of erection over 4 hours with no sexual behaviour - high flow priapism - arteriole blood trapped and is painful - low flow " - venous blood trapped and is not painful - caused by projectile drugs |
|
|
LC 2.22 Describe the 3 models of female sexual response? who created each? |
MASTERS AND JOHNSONS - most basic, liner model, excitation>plateau>orgasm>resolution BRASH MCGEER AND WHIPPLE previous model represented in no linear form, so resolution to next desire = libido, acknowledges previous sexual experiences influence next BASSON cyclical model which accounts emotional intimacy and relationship satisfaction feeding in to the sexual response |
|
|
LC 2.22 What hormones and neurotransmitters stimulate the female sexual response? which inhibit? |
STIMULATE : dopamine, oxytocin ,oestrogen, progesterone, testosterone INHIBIT: serotonin, prolactin (inhibits dopamine action) |
|
|
LC 2.22 What occurs in the genital tissues and peripheral system during arousal in women? |
GENITALIA the uterus begins to elevate so vagina becomes extended labia minora encourages with blood, becomes pinker labia manjora encourage with blood and swell and flatten to reveal vulva clitoris begins to swell n encourage with blood glands and epithelium begin to secrete mucus PERIPHERAL - increase BP - respiratory changes - nipple erection |
|
|
LC 2.22 What occurs in the genital during plateau phase of women sexual response? |
clitoris retracts under clitoral hood so it can take more stimulation labia minora continue to swell with blood, narrows lumen of vagina and creates orgasmic platform vagina is fully distended from uterus elevation |
|
|
LC 2.22 During orgasm describe a women muscle contraction pattern |
oxytocin release causes muscle contraction contraction starts 2 seconds after orgasm begins in lower 1/3 of vagina rhythmic contractions occur every 0.8 seconds , rest of body shows contraction also |
|
|
LC 2.22 What hormones/neurotransmitters are elevated during resolution in female sexual response ? |
prolactin and noradrenaline |
|
|
LC 2.22 What is dyspareunia? what are the 2 different types and what are common causes of each? HINT : in female sexual response |
pain while having sex DEEP: related to pelvic pathology, endometritis SUPERFICIAL: STI, menopause |
|
|
LC 2.17 What develops first in development of the gonads embryologically and when does this occur? |
urogenital ridge , week 5 |
|
|
LC 2.17 What cells migrate into the gonadal ridge during gonad development ? when? where do they originate from and what do they migrate through? |
germ cells , week 6 , originate in the yolk sac and migrate through the mesentery of the mid gut |
|
|
LC 2.17 describe the development of germinal epithelium during the indifferent phase of gonad development? |
- indifferent means only genetic sex has been determined not physical sex - germinal epithelium develops into chords/projections - start at edge of gonadal ridge and project in - germ cells have migrated to gonadal ridge by not further into germinal epithelium - around week 6 |
|
|
LC 2.17 Describe the development of germinal epithelium of males from week 8 in the embryo, what controls this? |
- controlled by SRY , if SRY is positive then will become male, SRY negative will become female , occurs around week 8 - the cortex of germinal epithelium in the gonadal ridge starts to degenerate and the medulla proliferates - start to show signs of tubes and tunica albuginea - germinal epithelium proliferates around germ cells |
|
|
LC 2.17 Describe the development of germinal epithelium of females in the embryo, what controls this? |
SRY , if no SRY present as no Y chromosome will be female at week 10 the medulla of the gonadal ridge starts to degenerate , leaves embryological remnant - the rete ovarii the germ cells migrate into the chords of germinal epithelium at week 14 the chords start to degenerate but in doing so they cuff the germ cells and coat them, this creates the primordial follicles |
|
|
LC 2.17 what are the names of the 2 developmental urogenital tracts? which degererates in the male due to what chemical? |
mesonephric/wolffian paramesonephric/mullerian paramesonephric degenerates due to mullein chemical |
|
|
LC 2.17 what chemical causes differentiation of the different parts of the male urogenital tract? |
testosterone |
|
|
LC 2.17 What does the paramesonephric duct develop into? |
uterine/follopian tube |
|
|
LC 2.17 What guides the decent of the testis? what space are they guided into? |
guided by gubernaculum into vaginalis process |
|
|
LC 2.17 in development of the external genitalia what folds to encompass the urethra in males? what chemical mediates this? what is hypospadias? |
uro-genital folds DHT hypospadias is the failure of urethral closing on the the dorsal (underside) of the penis |
|
|
LC 2.17 What is testicular feminisation ? how does it occur? |
male phenotype, confirmed through presence of leydig cells either leydig cells are unable to produce testosterone or testosterone receptors are faulty as testosterone/DHT needed for male external genitalia development this means this doesn't occur if no testosterone female external genitalia is default, therefor will develope female genitalia even though genitally male and have male internal gonads |
|
|
LC 2.20 what are the 4 types of progesterone only contraception? How does each work? |
IMPLANT - inserted sub-dermally into arm - inhibits LH release preventing ovulation, alters cervical mucus and surpasses endometrium preventing implantation PILL - alters cervical mucus, surpasses endometrium and alters utero-tubular fluid - prevents 60% (90% if desogestel) of ovulations INTRA-UTERINE DEVICE - doesn't effect hypo-pit axis - alters cervical mucus, utero tubular fluid INJECTABLE - suppress LH release stopping all ovulation - also alters cervical mucus and endometrium - effective 8-13 weeks |
|
|
LC 2.20 What are the 3 types of combined oral contraception? |
patch, ring , and pill - all prevent ovulation of the first 7 days and maintain ovulation for the next 14 days |
|
|
LC 2.20 When can't you take combined contraception? |
- BMI >35 - over 35 years old and smoke - recently had breast cancer - hypertensive - suffered with thromboembolisms previously |
|
|
LC 2.20 What are the 2 types of emergency contraception? how does each work? |
HORMONAL - prevent ovulation INTRA-UTERINE COPPER DEVICE - inserted into endometrium and alters compostion so no implantation can occur , effective 5 days after ovulation and for 5 days after insertion |
|
|
LC 2.21 Name the non-hormonal methods of contraception |
- withdrawal - spermicide - barrier methods - natural family planning - cycle times - intra-uterine copper device - sterilisation |
|
|
LC 2.19 Define infertility |
the inability to successfully reproduce after 12 months of unprotected regular sex |
|
|
LC 2.19 What are the main causes of infertility? What % do they account for? |
ovulatory disorder - 25% tubal factor - 20% uterine - 10% male - 30% unknown 25% adds to 110 :'( |
|
|
LC 2.19 what does ICSI stand for? ( related to IVF) |
intra-cellular sperm injection - used when sperm isn't motile |
|
|
LC 2.17 What are the 3 parts of the SRY gene? |
SP1, SF1 , WT1 |