![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
37 Cards in this Set
- Front
- Back
|
Feedback control |
Compare sensory inputs to desired state. Generates error signal that goes to controller - brain areas - and eventually goes to actuators that produce a movement. |
|
|
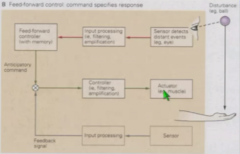
Feedforward control |
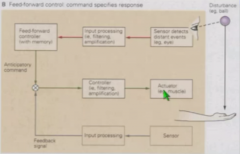
Sensory inputs are fed to feed-forward controller. Generates anticipatory command that is passed to actuator muscles. Feedback signaling necessary to adjust. |
|
|
EMG activity at biceps, triceps, wrist flexor, and wrist extensor when catching ball |
Bicep and wrist extensor EMG activity rises tens of milliseconds before ball arrives at hand - anticipatory activity to resist impact. Movement peaks only after ball hits hand. |
|
|
Basic of motor control for face and body |
Corticospinal tract upper motor neurons travel down ventral horn and synapse on lower motor neurons and spinal interneurons. Control of face - brainstem motor nuclei, not spinal cord lower motor neurons. |
|
|
Position of axial and appendicular |
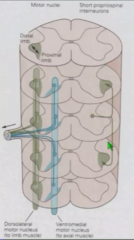
Lower motor neurons for axial muscles are in venteromedial, limb muscles are in dorsolateral part of ventral horn. |
|
|
Short propriospinal interneurons |
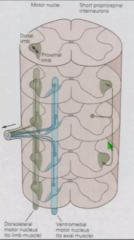
Spinal cord's own interneurons Go up and down several segments. Can be responsible for abnormal movements in just a few segments. |
|
|
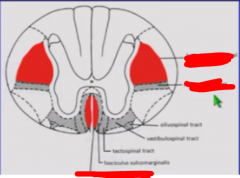
Medial brainstem pathways |

Project to venteromedial axial musculature lower motor neurons. Includes vestibulospinal tract, tectospinal tract, and reticulospinal tract. |
|
|
Tectospinal tract |

Tectum - primitive visual area that forms tectospinal tract. Connections go bilaterally to medial lower motor neurons although tectum fibers do cross over. |
|
|
Reticulospinal tract |

Tectum also projects to medial reticular formation, which forms reticulospinal tract that is involved in postural control. |
|
|
Vestibulospinal tract |

Input from inner ears feed into vestibular nuclei which controls ability of neck and body to resist changes in posture. |
|
|
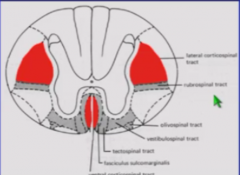
Lateral brain stem pathways |

Projects to dorsolateral appendicular musclature lower motor neurons. |
|
|
Rubrospinal tract |

lateral pathway. Projects from red nucleus, midbrain motor projection, contralaterally (just like motor cortex) down rubrospinal tract to control proximal musculature. |
|
|
Rubrospinal tremor |
Multiple sclerosis, coarse "wing-beating" tremor - if hold hands near nose, elbows tremor uncontrollably. |
|
|
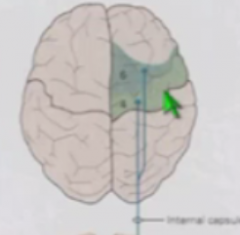
Ventral corticospinal tract |

Goes contralaterally through internal capsule, cerebral peduncles, pons. Ends in brainstem and lower axial motor neurons. May cross over at spinal cord level. |
|
|
Distinguishing hand area of precentral gyrus |

"Hand knob" Seen as upside down omega or episilon. Highly folded and expanded because of importance of hands. |
|
|
Precentral gyrus Brodmann areas |
Area 4, more anterior is Brodmann area 6. Broddman area 4 has Betz cells which control LMN through projections to corticospinal tract. Brodmann area 6 primarily project to propriospinal interneurons, not lower motor neurons. |
|
|
Lateral corticospinal tract |

Input from precentral gyrus (Brodmann 4 and 6) plus postcentral gyrus sensory areas. Almost completely crosses over at pyramidal decussation, innervates LMNs for limbs/appendicular. |
|
|
Where are Betz cells located? |
Primarily Brodmann area 4, but a few in Brodmann area 6 and some in postcentral gyrus as well. |
|
|
Comparison of corticospinal tract in human and rat |
Rat has dorsal corticospinal tract instead of lateral corticospinal tract Still has ventral corticospinal tract |
|
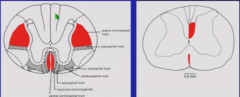
Cross section of human spinal cord |
Lateral corticospinal tract Rubrospinal tract below it Ventral corticospinal tract in completely different location |
|
|
UMN lesion symptoms |
Weakness Spasticity - increased motor output with stretch or constantly, because loss of inhibitory input from UMN to LMN, increase in reflexes, and increase in LMN excitability in absence of UMN input Increase in reflexes Loss of fine motor control - measured by inability to tap finger and thumb together |
|
|
Causes of UMN Lesion Symptoms |
Loss of descending inhibition Increased gain of spinal reflexes |
|
|
Extrapyramidal lesions |
Not in pyramidal tract but in basal ganglia. Leads to abnormal motor output in form of: Rigidity - Increased activity in multiple muscles Tremors - Patterns of abnormal motor activity Slowness Postural instability - Inability to compensate for postural changes. |
|
|
Rigidity vs spasticity |
Spasticity is increased motor output in response to stretch, Rigidity is increased activity in multiple muscles |
|
|
Babinski reflex |
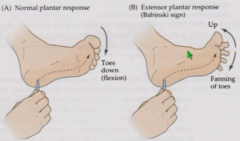
Normal plantar reflex - if stroke bottom of foot, toes flex down. Positive Babinski reflex - Big toe goes up and other toes fan down. Normal in babies but suppressed by upper motor neurons throughout most of life. Reliable sign of damage to corticospinal tract. |
|
|
|
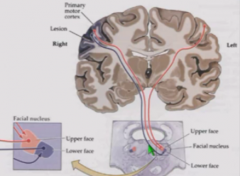
Lower motor neurons for face are in brainstem - facial nucleus contains motor neurons for lower and upper face. For upper face, facial nucleus gets input from both motor cortices. For lower face, facial nucleus gets input from contralateral motor cortex. |
|
|
Upper motor lesion on one side of facial nucleus |
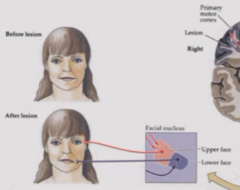
Preserved strength in upper face usually because facial nucleus for upper face gets input from both motor cortices. Lower face gets facial droop because input from only contralateral cortex. |
|
|
How can spinal reflexes be modified? |
Development (Babinski) Experience/conditioning |
|
|
Learning postural reflexes - move platform backwards |

Gastrocnemius (plantar flexor that extends ankle) Place subject on platform that suddenly moves backwards, causing subject to lean forward. Activity in gastrocnemius seen in EMG becomes earlier and increases. Body sway goes down. Result of upregulating reflex that is usually inhibited when walking. |
|
|
Learning postural reflexes - move platform forwards |

Must use tibialis anterior to respond, not gastrocnemius. Gastrocnemius is activated at first but activation decreases with successive repetitions. |
|
|
Concussions and sway |
Concussions affect postural control. Football players with concussions have sway similar to MS or peripheral neuropathy. Worse when eyes are closed. |
|
|
Adaptation of posture |
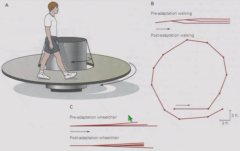
Walk on turntable - must take longer steps on side moving faster to stay in same place. After walking on turntable with eyes closed, walk on circle. Effect lasts for several minutes. Does not occur with person in wheelchair - adaptation is not to circling environment but to specific motor activity of walking. |
|
|
Central pattern generation |
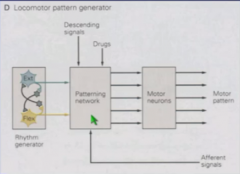
Network of neurons with inhibitory connections where one type of movement inhibits another. Output goes into patterning network that produces motor pattern via motor neurons. Exists for a variety of activities. |
|
|
Where in brain is CPG for walking? |
Cannot pin down one place |
|
|
Stimulating motor activity in people with spinal cord injury. |
Can implant or place sticky electrodes to activate rhythmic activity in spinal cord Continuous high frequency stimulation of increasing intensity can yield increasing muscle activity. Can generate gait like patterns of activity in multiple muscles with combination of stimulation and treadmill stepping. |
|
|
Cortical role in motor control |
Neuroinfraspectroscopy - look at brain activity while walking.
Multiple areas including primary sensory, primary motor, and supplemental motor area (brodmann area 6, head of prefrontal cortex) are activated while walking. Brodmann area 6 is a midline area important in bilateral control. |
|
|
Effect of counting or chewing gum while walking |
Higher cortical activation |