![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
183 Cards in this Set
- Front
- Back
- 3rd side (hint)

What is 1? |
Renal Column |
|
|

What is 2? |
Renal Pyramid |
|
|

What is 3? |
Minor Calyx |
|
|

What is 4? |
Major Calyx |
|
|

What is 5? |
Ureter |
|
|

What is 6? |
Renal Pelvis |
|
|

What is 7? |
Renal Vein |
|
|

What is 8? |
Renal Artery |
|
|

What is 9? |
Renal Capsule |
|
|

What is 10? |
Cortex |
|
|

What is 11? |
Interlobular arteries and veins |
|
|

What is 12? |
Arcuate arteries and veins |
|
|

What is 13? |
Interlobar arteries and veins |
|
|
|
Kidneys are bean shaped organs that are paired organs that are located along the _____ abdominal wall. |
Posterior |
|
|
|
Kidneys are peritoneal or retroperitoneal? |
retroperitoneal |
|
|
|
What is the length of normal kidneys? A. 8-10 cm B. 10 - 12 cm c. 13 - 15 cm D. 16 - 18 cm |
B 10-12 cm |
|
|
|
What extends from the medial aspect and includes the renal A., renal V, ureter, lymphatics, and nerves? |
Renal Hilum |
|
|
|
Kidneys are surrounded by a _______ capsule? |
fibrous |
|
|
|
What surrounds the kidneys capsule? |
perirenal/perinephric fat |
|
|
|
Where do adrenal glands sit? |
Superior, anterior and medial |
|
|
|
What encloses the kidney, adrenal gland and perirenal/perinephric fat? |
Gerota's Fascia |
|
|
|
What is the AKA for Gerota's fascia |
Renal fascia |
|
|
|
Kidneys can move up to __ to __ cm with respiration? |
3 to 4 cm |
|
|
|
What are the 2 important muscles and where are they located? |
1. Psoas Major: medially 2. Quardatus lumborum: posteriorly |
|
|
|
Urinary and reproductive systems develope from a mass of cells called? |
Mesoderm |
|
|
|
In males, the epididymis, ductus deferens, and ejaculatory duct form from the ? |
Wolffian duct |
|
|
|
In females, the Wolffian duct atrophies and the _____ duct forms the uterus and upper 2/3 of the vagina |
Mullerian duct |
|
|
|
Outer layer of renal parenchyma and extends from the capsule to base of the renal pyramids |
Renal Cortex |
|
|
|
What is the portion of cortex passing between the pyramids to sinus? |
Column of Bertin |
|
|
|
Inner layer of parnechyma, b/t cortex and sinus, 4-28 pyramids, cortex and medulla compose renal parrenchyma |
Medulla |
|
|
|
What is flat, funnel shaped cavity located medial to the hilum, has 8-18 minor calyces and 2-3 major calyces, and where urine exits kidney via ____ thru ureter urinary bladder and ultimately the urethra. |
Renal Pelvis |
|
|
|
What houses the minor and major calyces, renal artery, renal vein, lymphatics, fat and fibrous tissue? |
Renal Sinus |
|
|
|
What is the functional unit of the kidney, that consists of glomerulus, collecting tubules and blood vessels and located in the renal cortex |
Nephron |
|
|
|
Renal arteries arise from the ____ below the __. |
Aorta and SMA |
|
|
|
What renal artery is longer? Why? |
Right b/c it passes posterior to the IVC |
|
|
|
Venous blood returns via: _____ : ______ : ______ : ____ : ______ : ______ |
Interlobular vein, arcuate vein, interlobar vein, segmental vein, renal vein, IVC |
|
|
|
What renal vein is longer and why? |
Left, passes b/t the SMA and aorta |
|
|
|
At the renal hilum: What is anterior? Middle? and Posterior? |
Anterior: renal Vein Middle: Renal Artery Posterior: Ureter |
|
|
|
What is the function of the kidneys? |
produce urine Regulate water, electrolytes, acid/base content of blood and blood pressure. |
|
|
|
How many gallons of blood per day is processed by kidneys? How much urine is produced each day? |
45 and 11500 ml |
|
|
|
What are the lab values found with kidneys? |
Blood Urea Nitrogen (BUN), Creatinine, and Urine Protein |
|
|
|
Renal cortex appears ______ Pyamids appear ______ Renal sinus appears _____ due to fat |
Homogeneous, hypoechoic, and echogenic |
|
|
|
What is an anatomic variance that has a persistent portion of renal cortex and may cross b/t renal sinus? |
Column of Bertin |
|
|
|
What anatomic variance has an excessive fatty infiltration of the renal pelvis, anatomic variant due to age 6th-7th decade, assoc. w/obesity and parenchymal atrophy and has renal calculi assoc. 70% of cases |
Renal Sinsus Lipomatosis |
|
|
|
What is the AKA for Renal Sinus Lipomatosis |
Fibrolipomatosis |
|
|
|
What anatomic variance is wedge-shaped hyperechoic defect in the anterior aspect near the upper and middle portions of the kidney? |
Junctional Defect |
|
|
|
What anatomic variance has an outward projection of normal tissue, usually seen at mid-pole - lateral border and may mimic a neoplasm? |
Dromedary Hump |
|
|
|
What anatomic variance is absense of one or both kidneys? |
Renal Agenesis |
|
|
|
What anatomic variance is an underdeveloped kidney, usually with compensated hypertrophy of opposite kidney |
Renal Hypoplasia |
|
|
|
What anatomic variance is more common in women, assoc. w/ development of renal diseases, and the most common congenital renal variant/anomaly ? |
Duplicated Collecting System |
|
|
|
What anatomic variance lies outside of the renal sinus, tends to be larger than the normal renal pelvis, central cystic area partially or entirely outside the kidney? |
Extrarenal Pelvis |
|
|
|
What anatomic variance is where there is more than 2 kidneys, usually ectopic? |
Supernumerary Kidneys |
|
|
|
What anatomic variance is where the kidney is located out of the expected anatomic location? |
Ectopic Kidney |
|
|
|
What anatomic variance has a fusion of the inferior poles that creates horshoe shaped kidneys that crosses the midline of the abdomen anterior to the great vessels and may present as a pulsatile mid-abdominal mass? |
Horseshoe Kidney |
|
|
|
What kidney disease is relatively common occurrence in newborns but is the most common cystic dysplasia, caused by a complete ureteral obstruction in utero, multiple cysts of various sizes. |
Multicystic Kidney Disease (MCDK) |
|
|
|
In Multicystic Kidney Disease, which kidney is often affected? |
Left |
|
|
|
In Multicystic Kidney Disease, on U/S multiple cysts which do not _______. |
communicate |
|
|
|
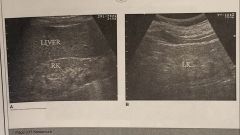
What kidney disease is present at birth as symmetrically enlarged echogenic kidneys, has microscopic cysts, difficulty to distinguish sinus from cortex and medulla, cortex will become anechoic and the medullary portion enlarges w/ the calyces and pelvis. |
Infantile Polycystic Kidney Disease |
|
|
|
What is the AKA for Infantile Polycystic Kidney Disease? |
Autosomal Recessive Polycystic Kidney Disease |
|
|
|
What kidney disease is relatively common, has unknown cause, accounts for 8-10% of those who require chronic dialysis or renal transplant, most are autosomal dominant trait, S&S by 4th decade and death occurs 10 years after onset of symptoms. |
ADPKD (Autosomal Dominant Polycystic Kidney Disease) |
|
|
|
What kidney disease has cystic dilatations in the prox convoluted tubles, Bowman's capsule and collection tubles. Cysts enlarge with age and renal function decreases and has assoc. complications w/: infection, calculi, cyst rupture, hemorrhage, and ureteric obstruction. |
Autosomal Dominant Polycystic Kidney Disease |
|
|
|
What kidney disease has a sonographic appearance of bilateral enlargement of kidneys, numerous cysts in cortex, poorly defined kidney margins due to peripheral cysts? |
ADPKD |
|
|
|
What should be also examined if ADPKD is identified? |
Liver, pancreas and spleen |
|
|
|
What kidney disease is non-inherited cystic disease of the collecting tubules/ducts, creates a sponge-like appearance of the medullary pyramids, increased incidence of kidney stones and rarely leads to serious conditions? |
Medullary Sponge Kidney |
|
|
|
What kidney disease in common in 50% of the population, arise from renal cortex, acquired condition d/t obstructed tubules, single/mult, many sizes, unilocular, asymptomatic. |
Simple Cyst |
|
|
|
What atypical cyst is 6% of simple renal cyst hemorrhage, occur with multicystic disease, appearence of age/stage of bleed, and increased risk of malignancy? |
Hemorrhagic Cysts |
|
|
|
What atypical cysts is 2.5% of cysts, fever and unilateral flank pain, resistent to antibiotic therapy, and u/s aspiration and drainage |
Infected |
|
|
|
What atypical cyst contains compartments or septa? |
Septated/multiocular cysts |
|
|
|
What type of atypical cyst is 1-2 % of simple renal cysts that were prev. infected or hemorrhaged, and has a hyperechoic wall> |
Calcifications |
|
|
|
What atypical cyst is common, calyceal deposits of calcium carbonate crystals, symptomatic and acoustic shadowing is possible? |
Milk of Calcium Cysts (MOC) |
|
|
|
What cyst originates in renal parenchyma and protrudes into the renal sinus? (single,large, simple cyst) |
Parapelvic cyst |
|
|
|
What cysts is a true sinus cyst, small, mult, irregular border but anechoic and can be confused with hydronephrosis |
Peripelvic cysts |
|
|
|
T/F? Parapelvic and peripelvic cyst do communicate with the collecting system? |
False, they do NOT |
|
|
|
What is assoc. with renal cysts and neoplasms, mental retardation, seizures, and skin lesions, can occur sporadically or may be autosomal dominant, and where cysts do not usually cause severe renal impairment ? |
Tuberous Sclerosis |
|
|
|
What cysts assoc. with systemic disease: autosomal dominant, variable penetrance, clinically not evident until 3 or 5th decade, Assoc. w/pancreatic islet cell tumors, pheochromocytomas and epididyma cystadenomas, cerebellar/spinal cor hemangioblastomas and retinal angiomas are usually 1st recognized |
Von-Hippel-Lindau Disease |
|
|
|
What is the most common benign tumor, usually asymptomatic, common in men 50-60 years old, small tumor 1-3 cm, may cause painless hematuria, appears echogenic, similar to RCC. |
Adenoma |
|
|
|
What is a very large vascular adenoma (up to 26cm), asymptomatic unless large/hematuria, in men, well-defined hypechoic mass, central scar from hemorrhage, similar to RCC |
Oncocytoma |
|
|
|
What is benign, hamartomatous mass composed of fat, blood vessels and smooth muscle, has two types. |
Angiomyolipoma (AML) |
|
|
|
What type of AML is unilateral, solitary mass, women, occurs in 4-6th decade, not assoc. w/Tuberous Sclerosis. What type of AML is mult. and assoc. with Tuberous Sclerosis? |
Type 1 and Type 2 |
|
|
|
What kidney disease where patients are asymptomatic, if have will be (flank pain, hematuria, life threatening hemorrhage, hypertension, and renal failure), malignant transformation is very rare. |
Angiomyolipoma |
|
|
|
What kidney disease has a sonographic appearance of homogenous and echogenic, located in the cortex, acoustic shadowing (20-30%), and may mimic appearance of RCC? |
Angiomyolipoma |
|
|
|
What is the most common malignant tumor of the kidney? |
Renal Cell Carcinoma |
|
|
|
What is the AKA for Renal Cell Carcinoma? |
Hypernephroma or adenocarcinoma |
|
|
|
What age and who has more common findings? |
after 50, males |
|
|
|
Renal Cell Carcinoma has an increased risk with patients who have____, _____ and _____ |
Von Hippel-Lindau disease, ADPKD and Tuberous Sclerosis |
|
|
|
What are classic symptoms of RCC? |
Costo-vertebral angle pain, palpable mass, hematuria* |
|
|
|
What has a tumor size that varies, invades renal tissue and sometimes appear to have a capsule, spread into perinephric fat and renal veins, allows mets (75% to lungs) |
Renal Cell Carcinoma |
|
|
|
What stage of RCC: tumor within kidney |
1 |
|
|
|
What stage of RCC: Tumor in perinephric fat but confined to Gerota fascia |
2 |
|
|
|
What stage of RCC: Tumor in renal vein, regional lymph nodes, or vena cava |
3 |
|
|
|
What stage of RCC: Adjacent organ invasion, distant metastases, tumor in juxtaregional lymph nodes. |
4 |
|
|
|
What has an U/S appearance of may be highly vascular, may contain areas of hemorrhage, necrosis, or cystic changes, appear hyperechoic, 20-30% calcifications, extension into Rt. renal V (20-30%) and (5-10%) have renal thrombosis into IVC/ |
Renal Cell Carcinoma |
|
|
|
What is the most common malignant renal tumor in pediatric patients, second most common solid abdominal tumor in children, 3-4 years old |
Wilm's Tumor |
|
|
|
What is the AKA for Wilm's Tumor? |
Nephroblastoma |
|
|
|
There are cogenital malformations that increase the child's likelihood of developing Wilm's Tumore. What are they? |
1. Absent Iris 2. Beckwith - Wiedemann Syndrome 3. Denys- Dash Syndrome |
|
|
|
What has a sonographic appearance of large, well-circumscribed smooth mass, homogeneous, may contain hypoechoic or cystic areas, may arise from sinus and distort kidney, freq. invade the renal v. and extend into IVC or heart, mets to liver and lung |
Wilm's tumor |
|
|
|
What has s&S of Palpable abdominal mass, pain, fever, malaise, weight loss, hematuria, and hypertension? |
Wilm's Tumor |
|
|
|
What is a malignant tumor of the lining of the renal pelvis, calyces, ureter and bladder, 8-10% of all renal cancers, most are transitional, hematuria symptoms arise quickly, 5 year survival rate after removal is approx. 90% |
Urothelial Carcinoma |
|
|
|
What is 7% of all renal neoplasms, 90% of all primary renal pelvis tumors, painless hematuria, avg. age of diagnosis 61, males, variable appearance(too small to visualize to lare, bulky tumors) |
Transitional Cell Carcinoma |
|
|
|
What has splitting or separation of the central echo complex or hypoechoic lesions. If infiltration into renal cortex occurs it is difficult to distinguish from RCC and the color doppler is not very helpful in diagnosis. |
Transitional Cell Carcinoma |
|
|
|
What is highly malignant, mets early, poor prognosis, assoc. w/kidney stones and infection and has sono findings of calculi, marked hydronephrosis due to ureteropelvic junction obstruction. |
Squamous Cell |
|
|
|
What is due to blood flow, kidneys common location of mets, lymphoma non-specific, bilateral enlargement of the kidneys and can appear hypo to hyperechoic |
Metastastic Renal Tumors |
|
|
|
What is caused by inflammation, HTN, diabetes, transplant rejection, renal failure, increased BUN and creatine, and echogenic cortex |
Renal Cortex Disease |
|
|
|
What has a chemical imbalance of hyperuricemia, nephrocalcinosis, hypokalemia, and has echogenic pyramids? |
Renal Medullary Disease |
|
|
|
What Renal Medical disease has increased renal parenchyma, decrease in renal sinus fat echogenicity, and focal calcifications in the cortex and pyramids? |
AIDS |
|
|
|
What Renal Medical Disease casuses chronic renal failure, leading cause of death among diabetes, and renal vascular resistance. |
Diabetic Neuropathy |
|
|
|
What Renal Medical Disease is the destruction of the renal pyramids, common cause of death in drug over dose, may see hypoechoic medullary rims with anechoic spaces d/t necrotic papillae, and calcifications w/in the pyramids that may or may not shadow |
Papillary Necrosis |
|
|
|
What Renal Medical Disease is an autoimmune disease, female, and Lupus Nephritis (increased cortical echogenicity and small/large renal size) |
Systemic Lupus Erythematosus |
|
|
|
What is the inability of kidneys to excrete waste, concentrate urine and control electrolytes, pre-stage is renal insufficiency, end stage is ESRD, and may be acute or chronic. |
Renal Failure |
|
|
|
What is potentially reversible, kidneys appear normal or enlarged, oligouria, elevated BUN and creatine, most common cause is acute tubular necrosis(ATN), 60% mortality |
Acute Renal Failure |
|
|
|
What is irreversible, lab values steadily increase, caused by inflammation, diabetes, HTN and vascular disease, small and echogenic kidneys, and treatment is dialysis or transplant |
Chronic Renal Failure |
|
|
|
What is the treatment where urea and toxins are mechanically filtered from blood, has increased incidence of cysts and carcinoma, small and possibly cystic kidneys |
Renal Dialysis |
|
|
|
What is the treatment for irreversible chronic renal failure, kidney is placed in pelvis along iliopsoas margin, renal vessels are anastomosed with iliac vessels, native kidneys usually left in place |
Renal Transplant |
|
|
|
What are some renal transplant complications? |
infection, vascular compromise (occlusion or stenosis of artery/vein) and hydronephrosis |
|
|
|
What is the most common cause of failure AFTER 1st week of renal transplant? ( anechoic pyramids and increased echogenicity of cortex) |
Rejection |
|
|
|
What is the most common cause of failure in the 1st week? (U/s appears normal, oliguria and increased creatine) |
Acute Tubular Necrosis |
|
|

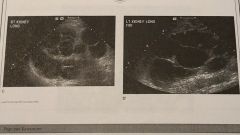
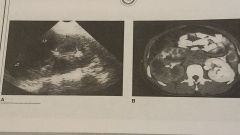
What is this? |
Column of Bertin |
|
|

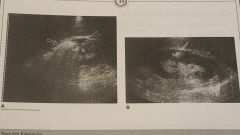
What is this? |
Junctional Defect |
|
|

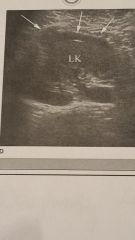
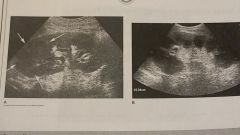
What is this? |
Dromedary Hump |
|
|
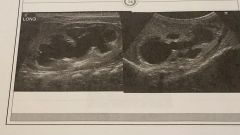
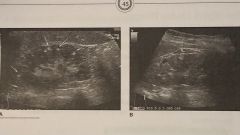
What is this? |
Duplicated Collecting System |
|
|

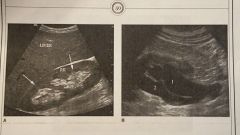
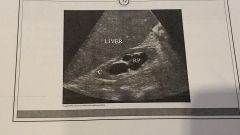
What is this? |
Extrarenal Pelvis |
|
|
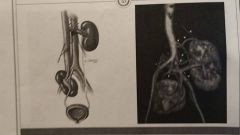
What is this? |
Supernumerary Kidneys |
|
|
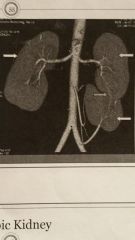
What is this? |
Ectopic Kidney |
|
|

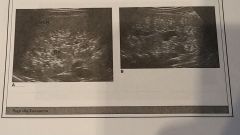
What is this? |
Multicystic Dysplastic Kidney Disease |
|
|
What is this? |
Infantile Polycystic Kidney Disease |
|
|
What is this? |
ADPKD |
|
|

What is this? |
Medullary Sponge Kidney |
|
|
What is this? |
Simple Cyst |
|
|

What is this? |
Parapelvic Cysts |
2 |
|
What is this? |
Tuberous Sclerosis |
2 |
|

What is this? |
Renal Adenoma |
|
|

What is this? |
Oncocytoma |
|
|

What is this? |
Angiomyolipoma |
|
|

What is this? |
Renal Cell Carcinoma |
|
|

What is this? |
Wilm's Tumor |
|
|
What is this? |
Transitional Cell Carcinoma |
|
|
What is this? |
Renal Cortex Disease |
|
|
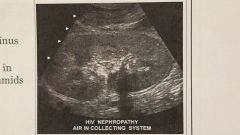
What is this? |
AIDS |
|
|

What is this? |
Diabetic Neuropathy |
|
|

What is this? |
Papillary Necrosis |
|
|
What is this? |
Chronic Renal Failure |
|
|
|
What is the obstruction of urine outflow, that can occur at any age, anywhere in urinary tract? |
Obstructive Uropathy |
|
|
|
Complete obstruction causes irreversible damage to the kidneys after how many weeks? |
3 |
|
|
|
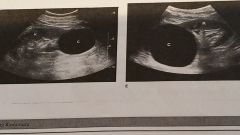
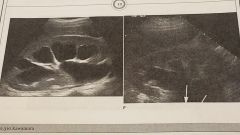
What is the dilatation of the renal pelvis and calyces, cystic areas communicate, if severe causes atrophy of renal parenchyma and loss of function. |
Hydronephrosis |
|
|
|
Calculi w/in or tumor Urinary tract, blood clot, stricture, ureterocele, and pyelonephritis are intrinsic or extrinsic causes of hydronephrosis? |
Intrinsic |
|
|
|
Surgery, trauma, neurogenic bladder, tumor, benign prostatic hyperplasia and pregancy are intrinsic or extrinsic causes of hydronephrosis? |
Extrinsic |
|
|
|
3 stages of hydronephrosis: mild moderate and severe. 1. ___ - anechoic separation of the entire sinus 2. Slight separation of the sinus echoes 3. ___ extensive separation of the central sinus and calyces w/thinning of the cortex |
1. Moderate 2. Mild 3. Severe |
|
|
|
What is one way to distinguish hydronephrosis when evaluating? |
Make sure 'cysts' communicate |
|
|

What is this? |
Grade 1 Hydronephrosis |
|
|
What is this? |
Grade 2 Hydronephrosis |
|
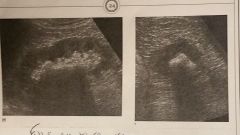
|
What is this? |
Grade 3 Hydronephrosis |
|
|
|
What is calculi w/in the urinary system, common in males, 20-50 years old, family history, previous infections, hot climates |
Urolithiasis |
|
|
|
What is where stones may be single or mult, cause partial or total obstruction, can remain in the kidney or if small can be passed, most stones are calcium oxalate and calcium phosphate, asymptomatic, hematuria, back pain, lower quadrant |
Nephrolithiasis |
|
|
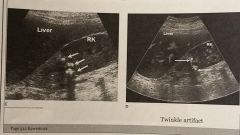
What is this? |
Nephrolithiasis |
|
|
|
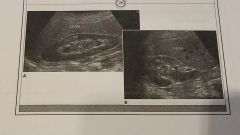
What is large irregular stone in shape of collecting system? |
Staghorn Calculi |
|
|
What is this? |
Staghorn Calculi |
|
|
|
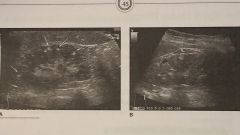
What is renal parenchyma calcium deposition in the cortex or medulla, bilateral and diffuse, metabolic syndromes and hypercalcemia, difficult to distinguish from large renal stones, calcifications in the renal cortex that may shadow |
Nephrocalcinosis |
|
|

What is this? |
Nephrocalcinosis |
|
|
|
70% of renal capsule and parenchyma trauma is due to ____ trauma? |
blunt force |
|
|
|
What is a result of trauma to kidney, occurs b/t cortex and capsule, most common complication of renal biopsy? |
Subcapsular Hematoma |
|
|
What is this? |
Subcapsular Hematoma |
|
|
|
What is very common and has potential to spread to kidneys, common in young women, bacteria spreads with urinary retention, stasis, incomplete emptying, outlet obstruction? |
UTI |
|
|
|
What is where bacteria can ascend urinary tract w/in by lymphatic route, or spread thru bloodstream, and E Coli is the most common bacteria? |
UTI |
|
|
|
What is inflammation including renal pelvis, calces, and renal parenchyma, unilateral/bilateral, starts as UTI, women 15-35, symptoms of dysuria, frequency, urgency, chills, fever, back ache. Lab values of leukocytosis and pyuria, treatment of antibiotic |
Acute Pyelonephritis |
|
|

What is this? |
Acute Pyelonephritis |
|
|
|
What is recurrent infections cause scarring of the kidney, unilateral/bilateral, symptoms same as APN w/ polyuria and nocturia, HTN and Renal failure assoc. Labs: Leukocytosis and pyuria. |
Chronic Pyleonephritis |
|
|

What is this? |
Chronic Pyleonephritis |
|
|
|
What is a type of CPN, rare, normal renal parenchyma is replaced by lipidladen macrophages, plasma cells, and multinucleated giant cells. Common w/obstruction of UPJ and Staghorn Calculi. Common in women and diabetics |
Xanthogranulomatous Pyelonephritis (XGP) |
|
|
What is this? |
XGP |
|
|
|
What is a type of CPN, considered a life threatening illness, middle-aged diabetic patients, immunosuppressed patients and women w/urinary tract obstructions. E coli most common cause. |
Emphysematous Pyelonephritis |
|
|
What is this? |
Emphysematous Pyelonephritis |
|
|
|
What is usually pus-filled, renal carbuncle. Sym: flank pain, chills, fever. May require surgical drainage. |
Renal Abscess |
|
|

What is this? |
Renal Abscess |
|
|
|
What is the presence of pus in collecting system, check for debris w/in dilated renal pelvis |
Pyonephrosis |
|
|
What is this? |
Pyonephrosis |
|
|
|
What has candida albicans as most common, in premature infants w/long standing catheters, patients w/diabetes, leukemia, lymphoma, chronic illness, IV drug use, AIDS. Sono appearance: mimic APN, fungus balls. |
Fungal infections |
|
|

What is this? |
Fungal Infection |
|
|
|
What is where the kidneys may appear normal or demostrate ureteral obstruction and hydronephrosis, calcifications maybe seen in bladder or wall |
Schistosomiasis |
|
|
|
What manifests 10-20 years after initial infection, correlates u/s to clinical history!, may mimic XGP |
Tuberculosis |
|
|
What is this? |
Renal Tuberculosis |
|
|
|
What is rare, granulomatous inflammatory disease, yellow plaque like deposits in urinary system, middle aged women, recurrent UTI, Unilateral enlargement of kidney w/ poorly defined hypovascular cortical masses |
Malakoplakia |
|
|
|
What is the normal RI? |
.58-.64 RI >.70 is diagnostic of renal vessel obstruction |
|
|
|
What is caused by trauma, dehydration, pregnancy, surgery, CHF, tumor invasion, or renal disease? |
Renal Vein Thrombosis |
|