Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
32 Cards in this Set
- Front
- Back
|
1. What are the etiologies of HF that lead to a depressed EF?
|
a. CAD
b. Chronic pressure overload c. Chronic volume overload d. Non-ischemic cardiomyopathy e. AND MORE |
|
|
2. What are the etiologies of HF that lead to a conserved EF?
|
a. Pathologic hypertrophy
b. Aging c. Restrictive cardiomyopathy d. Endocardial disorders |
|
|
3. What is NYHA class I HF?
|
a. Cardiac disease
b. No limitation of activity c. Ordinary activity does not cause symptoms |
|
|
4. What is NYHA class II HF?
|
a. Slight limitation of activity
b. Ordinary activity causes fatigue, palpitations, dyspnea, and angina |
|
|
1. What is NYHA class III HF?
|
a. Marked limitation of physical activity
b. Less than ordinary activity causes fatigue, palpitations, dyspnea, and angina |
|
|
6. What is NYHA class IV HF?
|
a. Inability to carry on any activity without discomfort
b. Symptoms such as angina may be present at rest c. Symptoms worse with any degree of physical activity |
|
|
7. What is systolic HF?
|
a. Decreased pumping of LV
b. LV remodeling |
|
|
8. What is the tx focus for systolic HF?
|
a. Prevention of LV remodeling
|
|
|
9. What is diastolic HF?
|
a. Due to decreased myocardial relaxation
b. Due to structural changes due to fibrosis or cardiomyopathy c. Can be due to a-fib with RVR |
|
|
10. What are the ssx of HF?
|
a. Dyspnea
b. Orthopnea c. Paroxysmal nocturnal dyspnea d. Cheyenne-Stokes respirations e. Acute pulmonary edema |
|
|
11. What are Cheyenne-Stokes respirations?
|
a. Periodic or cyclic respirations present in advanced HF
b. Rapid respirations followed by apnea |
|
|
12. What are the PE findings of HF?
|
a. Varying BP
b. Rapid respiration c. JVD d. S3/S4 e. Hepatomegaly, ascites, tenderness f. Symmetric peripheral edema |
|
|
13. What does S3 indicate?
|
a. Volume overload
|
|
|
14. What does S4 indicate?
|
a. Diastolic dysfunction
|
|
|
15. What are the two important natriuretic peptides in HF?
|
a. BNP
b. Pro-BNP |
|
|
16. When is BNP/pro-BNP released?
|
a. During ventricular stretch or pressure
|
|
|
1. What happens to BNP/pro-BNP levels with age?
|
a. Increase
|
|
|
18. In what types of disorders are the natriuretic peptides elevated?
|
a. Preserved EF patients
b. Right-side heart failure c. Women |
|
|
19. What is the usefulness of natriuretic peptides in order to titrate tx?
|
a. Not very useful
b. Tx should be directed to reduction symptoms and maximizing CO |
|
|
20. What is the ECG evidence of LVH?
|
a. Tall R wave in aVL,
b. ST changes in V3-V6 and precordial leads |
|
|
21. What are some signs of HF on a CXR?
|
a. Enlarged silhouette
b. Cephalization c. Edema d. Pleural effusions e. Prominent hilar vessels f. Full, fuzzy hilum and basal congestion |
|
|
22. What is the CXR evidence of cardiomegaly?
|
a. Transverse diameter of heart is larger than the diameter of hemithorax
|
|
|
23. What is the CXR evidence of pulmonary edema?
|
a. Butterfly appearance
|
|
|
24. What are two ways to assess LV function?
|
a. Left ventriculogram during cath
b. 2D echo with doppler |
|
|
25. What is the effect of eccentric hypertrophy on EF?
|
a. Causes decreased EF
|
|
|
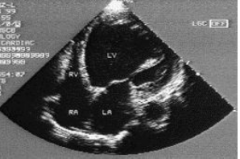
26. What does systolic dysfunction look like in a HF patient?
|
|
|
|
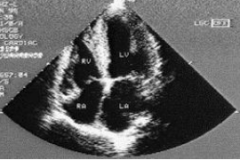
27. What does a diastolic dysfunction look like in a HF patient?
|
|
|
|
28. How do you tx HF?
|
a. Tx underlying condition
b. Exercise c. Restriction of Na d. Rx e. Device tx |
|
|
29. What pharm agents can be used to tx HF?
|
a. Diuretics
b. ACE inhibitors c. ARBs d. BB |
|
|
30. When is cardiac resynchronization indicated?
|
a. Patients on optimal medial tx AND→
b. EF< 35% c. QRS>120 ms d. NYHA class III or IV |
|
|
31. When is an implantable cardiac defibrillator indicated?
|
a. NYHA II-III with→
b. EF< 35% c. Maximal medical tx |
|
|
32. When can BiV pacer and ICD be combined?
|
a. NYHA class III-IV
|