![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
23 Cards in this Set
- Front
- Back

Symptoms arose and disappeared in 24 hrs |
Uticaria (Hives)
*Type 1 HS rxn w/ localized degranulation of mast cells *Red, Itchy, edmeatous plaques *Causes: IgE-Dep. Allergy, IgE-indepen rxn to opiates or curare, hereditary angioneurotic edema due to C1 comp def |
|

|
Atopic Dermatitis
*Type of eczema that is a Type 1 HS rxn part of "Atopic Triad" (asthma, hay fever, eczema) *Itchy, red, scaling, weeping skin *Gets better w/age |
|

|
Contact Dermatitis
*Type of eczema that is a Type IV HS rxn in response to poison ivy, nickel, irritants, meds |
|
|
Microscopic appearance of "Spongiotic Dermatitis" is associated with what skin condition? |
Acute Eczema Dermatitis
*Intercellular edema and perivascular inflammation |
|

|
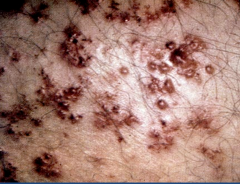
Erythema Multiformes
*HS rxn to HSV infxn, Adverse drug rxns (ie Steven Johnson synd), autoimmune d/o, and malignancies *Multiple targetoid lesions |
|
taken from a targetoid lesion |
Erythema Multiformes
*Sub-epidermal bullae *Epidermal necrosis (white center of target) surrounding by erythema |
|
|
Febrile Pt presents w/ target-like lesions along entire body, especially oral mucosa that progresses to diffuse sloughing of his skin. He recently took Allopurinol to treat his gouty toe. |
Steven Johnson Syndrome (type of severe erythema Muliformes)
*Other drugs that can cause this include: Febuxostat, Probenacid, Rasburicase, Pegloticase |
|
|
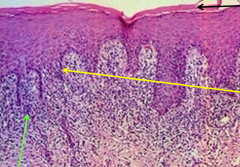
Psoriasis
*Green - elongation of rete pegs *Black - Munro Microabscess (neutrophil collection in corneum layer) *Yellow - hyperkeratosis *Red - Parakaratosis (retention of nuclei in corneum layer) |
|
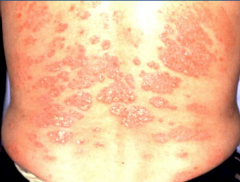
Lesions are puretic and scale |
Psoriasis
*Comp. mediated rxn against stratum corneum leading to increased keratinocyte turnover *Salmon-colored itchy plaques w/ silvery scales |
|

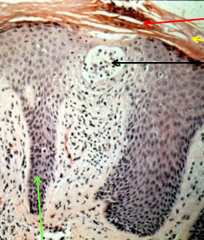
Lesions are pruritic |
Lichen Planus
*5 P's: Pruretic, Polygonal, Planar, Purple, Papule *Common on skin and oral mucosa |
|
|
Lichen Planus
*Sawtooth pattern and D-E jxn *green = lymphocytic infiltrate *Yellow = degeneration of basal keratinocytes *Black = hyperkeratosis |
|
|
What causes the discoid rash of Lupus erythematosis? |
Hyperkeratosis w/ keratin plugging of hair follicle and lymphocytic infiltrate along the D-E jxn |
|

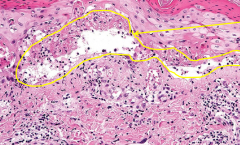
Bullae are easy to burst, causing the pt to become severely dehyrdated |
Pemphigus Vulgaris
*Autoimmune attack of desmosomes *Bullae also present in oral mucosa |
|
|
Pemphigus Vulgaris
*Supra-basal Blisters where basalis layer separates from rest of epidermis (acantholysis) |
|
|
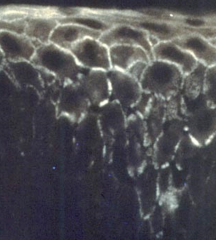
Pemphigus Vulgaris
*Fishnet IF pattern of anti-IgG against desomosomes (surround keratinocytes to hold to together) |
|

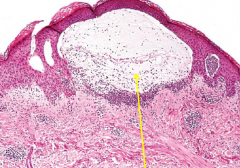
Bullae are tense and difficult to rupture |
Bullous Pemphigoid
*Autoimmune attack of hemidesmosomes **No bullae in oral mucosa** |
|
Pt has large tense bullae |
Bullous Pemphigoid
*Sub-Epidermal blisters where balasis layers lifts completely off of dermis |
|

|
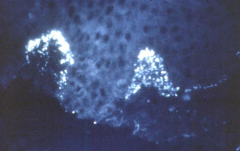
Bullous Pemphigoid
*Linear IF pattern of anti-IgG against Hemidesmosomes that hold basalis to BM |
|
Pt also has celiac's disease |
Dermatitis Herpetiformis
*IgA deposition due to autoantibodies against retaslin (anchoring fiber) creating groups of itchy HSV-like vesicles *associated w/ other IgA-opathies such as celiacs |
|
Pt has groups of small itchy vesicles |
Dermatitis Herpetiformis
*Sub-Epidermal Vesicles |
|
|
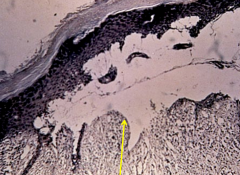
Dermatitis Herpetiformis
*IgA deposition at tips of dermal papillae |
|
|
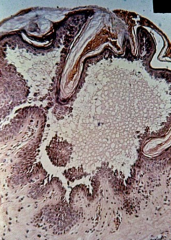
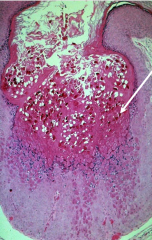
Molluscum Contagiosum
*pox-virus spread by direct contact creating cup-shaped lesions with Mollusum body cytoplasmic inclusion bodies (arrow) |
|
|
Pt w/ IBS comes in with painful red nodules with surrounding paler red skin. Microscopic examination shows panniculitis and edema. |
Erythema Nodosum
*Inflammation of sub-Q fat associated w/ IBS, malignancy, ifxn, drug reaction |