Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
18 Cards in this Set
- Front
- Back
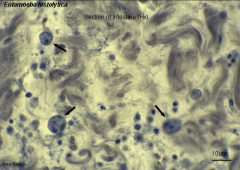
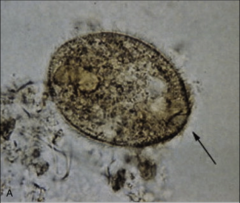
1. What organism are the arrows pointing to in the above picture?
2. What is the reservoir? 3. Where is it found? 4. How is it spread? |
1. Entamoeba Histolytica
2. Humans - Asymptomatic Carriers 3. Tropical and Subtropical Regions w/ poor sanitation and contaminated water --> Lower socioeconomic status 4. Ingestion of cysts in contaminated food/water |
|
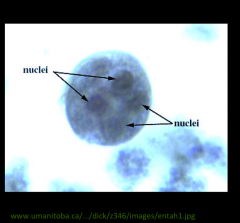
1. What organism is pictured?
2. What form is this and what part of pathogenesis is it responsible for? 3. Describe the morphology. 4. How do your treat this? |
1. Entamoeba Histolytica
2. Cyst Form - Infectious Form 3. 1-4 Nuclei 4. Metronidazole |
|
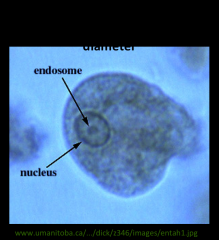
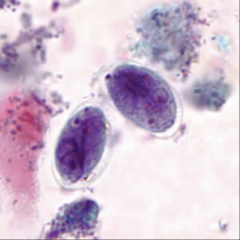
1. What organism is pictured?
2. What form is this and what part of pathogenesis is it responsible for? 3. Describe the morphology. 4. What is the lifespan of this form? |
1. Entamoeba Histolytica
2. Tropozoite Form - Responsible for tissue pathology 3. Amorphous Shape, 15-30microns 4. A few hours |
|
|
1. What is the lifecycle for Entamoeba Hystolitica?
2. How is it Diagnosed? 3. What does it cause if it goes into circulation? |

1. Ingestion of cysts by Human
2. Stomach acid stimulates Tropozoite release 3. Tropozoites released in duodenum 4. Division via Binary Fission - can cause pathology in the colon 5. Colonize Colon surface using Galactose-Inhibitable Adherence Protein 6. Breakdown of Mucous barrier, tissue, and ECM 7. CYTOTOXIN lyses Neutrophils and Epithelium --> Inflammation 8. Can invade mucosa and go into circulation. If not, they are passed in the feces Diagnosis by finding cysts and tropozoites in the feces If in Circulation --> Peritoneal Abscess or Liver, Lung, Brain, Heart involvement |
|

1. What is the black arrow pointing to and what organism causes this?
2. What are the 5 possible outcomes of infection? 3. Why does this get into your liver? |
1. Flask-shaped ulceration of the colon caused by the cytotoxin of Entamoeba Histolytica
2a. Amebiasis (Dysentery) - Localized destruction in the colon --> Bloody Diarrhea and Colitis 2b. Extraintestinal Amoebiasis --> Fever, Leukocytosis, Rigors 2c. Liver Involvement --> Hepatomegaly, Abscesses 2d. Pseudoappendicitis 2e. Asymptomatic --> Carrier 3. Tropozoites in the blood are removed as they pass through the liver |
|

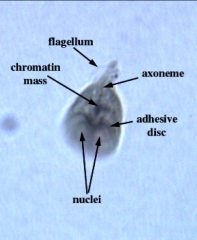
1. What organism is this?
2. Describe the morphology. 3. What forms does it take on? 4. Where is this found most often? 5. What are its hosts? |
1. Giardia Lamblia
2a. Tear-drop shape 2b. 4 flagella 2c. 2 nuclei w/ central Karyosomes --> look like eyeballs 2d. Adhesion disc on Ventral Side 3. Cyst and Tropozoite forms 4. Streams, Lakes, Mountain Resorts 5. Beavers and Muscrats |
|
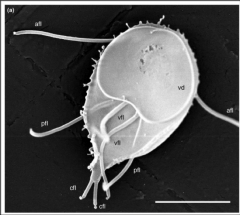
1. What organism is this?
2. Describe the morphology. 3. How does it move? 4. What populations are at risk? |
1. Giardia Lamblia
2a. Teardrop shape 2b. Ventral Sucker 2c. 4 flagella 2d. 2 nuclei with central Karyosomes that look like eyeballs 3. Flying Leaf Motility 4. Campers, Hikers, Daycare Centers, Places with poor sanitation |
|
1. What organism is this and describe the morphology.
2. Where does this rate among parasites in the US? 3. How is this transmitted/what is it's life cycle? |
1. Giardia Lamblia - Teardrop shaped, 4 flagella, 2 nuclei with central Karyosomes (eyeballs), and Ventral sucker
2. MOST COMMON PARASITE IN THE US 3a. Ingestion of cysts (fecal-oral) 3b. Gastric acid --> Excystation 3c. Release of Tropozoites in Duodenum and Jejunum 3d. Binary Fission Replication 3e. Ventral sucking disc sticks to intestinal villi --> Fat malabsorption 3f. Tropozoite absorbs nutrients via Pinocytosis 3g. Tropozoites and Cysts passed in feces |
|
1. What is this? Describe the morphology.
2. What are the possible symptoms of infection? 3. How is this diagnosed? 4. How is it treated? |
1. Giardia Lamblia - Teardrop, 4 flagella, 2 nuclei w/ central Karyosomes (eyeballs), and ventral sucker
2a. Asymptomatic --> Carrier 2b. Diarrhea and/or GI manifestation 2c. Steatorrhea from fat malabsorption 2d. Blood and Pus (RARE) 3. Diagnosed --> Stool samples and microscopy 4. Treat w/ Metronidazole |
|
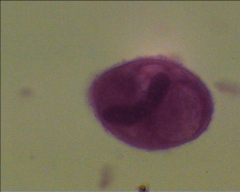
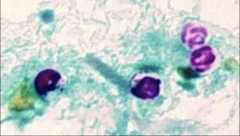
1. What organism is this and what form is it in?
2. Describe the morphology of this form 3. Describe the pathogenesis 4. How is this diagnosed? 5. How is this treated? |
1. Balantidium Coli - Tropozoite
2. Ovoid, Covered w/ Cilia --> Fuzzy appearance 3a. Fecal-oral transmission 3b. Causes ab pain and tenderness, Anorexia 3c. If invasive --> Bloody stools and pus 4. Cysts and Tropozoites in stool 5. Metronidazole OR Tetracycline |
|
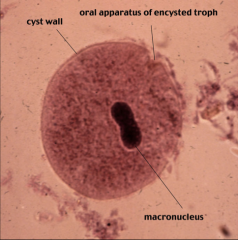
1. What form of what organism is this?
2. Describe the morphology 3. What are the reservoirs? 4. What population is at risk for this? |
1. Balantidium Coli - Cyst form
2. Spherical w/ distinctive cell wall 3. Pigs (100% infected), cows, horse, monkeys 4. Farmers |
|
1. What organism is this?
2. What form is it in? 3. Who is most at-risk for this and why? |
1. Balantidium Coli
2. Tropozoite form - Ovoid w/ Cilia (Fuzzy Appearance) 3. Farmers are at risk b/c 100% of pigs are infected |
|

1. What organism is this?
2. What stage is this in and how can you tell? 3. Describe the pathogenesis. |
1. Cryptosporidium Parvum -
2. Sporozoite - Sticks to Intestinal epithelium 3a. Ingestion of Oocyst (fecal-oral) 3b. Excystation in GI tract 3c. Sporozoites attach to intestinal epithelium 3d. Sticks straw in and sucks nutrients out 3e. Wraps cell membrane around itself (Like Sleeping Bag) 3f. Asexual Repro --> Schizogeny/Merogeny 3e. Sexual Repro --> Gametogeny (Micro/Macrogamonts = M/F) - Fertilization of Macrogamonts 3f. Oocysts produced and either autoinfect or are excreted |
|
1. What organism is this?
2. What stage is it in and how can you tell? 3. Where are these found and why are we still exposed to it? 4. What population is this fatal in? 5. How does it get nutrients? |
1. Cryptosporidium Parvum
2. Oocyst Stage - Thick walled and Acid Fast 3. In water - Runoff into municipal supply and resistant to purification via Chlorine 4. Immunocompromised 5. Sporozoite form uses a straw to suck nutrients from intestinal epithelium |
|
1. What organism is this?
2. What form is it in and how can you tell? 3. What does this cause in Immunocompetent people? 4. What does this cause in Immunocompromised people? 5. What population is this seen most in? 6. How do you diagnose it? |
1. Cryptosporidium Parvum
2. Oocyst - thick walled and acid fast 3. Competent - Mild/Perfuse Watery Diarrhea w/ Vomiting and Malabsorption (Self-limiting Gastroenteritis) 4. Compromised - Cholera-like diarrhea and dehydration 5. Seen in HIV patients 6. Acid Fast Stain or Immunofluorescence |
|
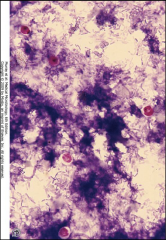
1. What organism is this and what form is it in?
2. How can you tell what form this is? What other form is there? 3. What population is at risk for this? 4. What are the clinical signs of this infection? 5. How is it diagnosed and treated? |
1. Isospora Belli - Oocyst
2. Oocysts are elliptical in shape. The other form is Coccidia 3. HIV/Immunosuppressed 4. Malabsorption and Hemorrhagic, Severe Diarrhea 5a. Diagnosis: Acid Fast Stain of the Stool for cysts. 5b. Treatment: TMP-SMX |
|

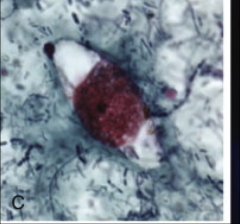
1. What organism is this?
2. Describe the morphology. 3. What form is this in? 4. How is this transmitted? 5. What infection are carriers of this at increased risk for? |
1. Trichomonas Vaginitis
2. Flagellate protozoa with and Undulating membrane and lashing flagella for motility 3. Tropozoite - ONLY SEEN AS A TROPOZOITE 4a. STD - In urethra, prostate, vagina 4b. Mechanical irritation and inflammation through microulcerations of tissues by flagella 5. HIV b/c of microulcerations caused by flagella |
|
1. What is this symptom and what causes it?
2. What else does this organism cause? 3. What is the pH here? 4. How is this diagnosed? 5. How is this treated? |
1. Strawberry Cervix (inflammation, irritation, sores) - Trichomonas Vaginitis
2a. Vulvar itching and burning 2b. Frothy skin discharge 2c. Rancid odor 2d. Dysuria, Dyspaneuria 3. Vaginal pH goes above 4.5 4a. Tropozoites Corkscrew motility in Methylene Blue 4b. Microscopic Exam of Discharge for Tropozoites 4c. Vaginal pH test (>4.5) 5. Metronidazole |