![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
25 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
All the Hepatitis Viruses are very different from one another. Some DNA/ some RNA etc.... WHAT DO THEY ALL HAVE IN COMMON? WHAT IS A SINGLE DEFINING FEATUERE OF THE HEPATITIS VIRUS? |
The Hepatitis Virus ONLY infects the LIVER
|
|
|
|
Which hepatitis types can you get vaccines for? Why not all of them?
Hint* A+B both have vaccines. What is it about the C virus that make it useless to make a vaccine. |
Hepatitis C virus (HCV) does not have a vaccine!
B/c it is an RNA VIRUS. (Unlike HAV and HBV which are both stable DNA virus types) -no protective immunity -RNA polymerase= no proofreading / high mutations - mutation too frequent-- antibodies are useless |
|
|
|
Someone comes in that you suspect may have Heptitis type A (HAV). What might they look like and how would you diagnose it?
|
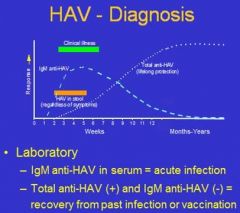
Clinical
i. Symptoms of actute hepatitis • not specific for HAV vs. other hepatitides • not always present ii. Patient history / social factors • Travel to endemic area • part of an outbreak Laboratory Diagnosis i. Tests for IgM and total anti-HAV antibodies • IgM anti-HAV (+) = acute HAV infection • IgM (-) + total anti-HAV (+) = past HAV infection or vaccination |
|
|
|
A patient comes in that you suspect may have Hep B virus. Which antigen/ antibodies would you use to diagnose for it (acute vs. chronic)? How do they symptoms present?
|
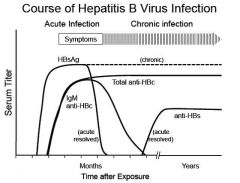
Diagnosis
Clinical: Symptoms of hepatitis • not specific for HBV vs. other hepatitides • not always present vi. Assess patient history for risk factors • HBV status of mother • Exposure (IV drug use, HBV-pos. sex partner) b. Laboratory Diagnosis of HBV infection requires analysis of more than one serum marker in order to differentiate current acute infection, previous resolved infection, chronic infection, and possibly vaccination status. The markers used and their utilities are as follows: • HBsAg (hepatitis B surface antigen) – the virus envelope protein – indicates presence of virus (acute or chronic infection) • anti-HBc (total antibody to the HBV core protein) – indicates current or past infection. (Antibody to the virus core protein (HBc) can coexist with chronic infection because this antibody does not bind to whole virus particles – the core protein is sequestered inside). • IgM anti-HBc (IgM antibody to the HBV core protein) – indicates current acute infection • anti-HBs (antibody to the hepatitis B surface antigen) – protective antibody generated following resolution of infection and by the HBV vaccine • HBe / anti-HBe (hepatitis B “e antigen”/antibody to hepatitis B e antigen) – mutually exclusive markers can be useful for assessing status of chronic infection (HBe pos = high levels of virus; anti-HBe = low levels of virus) |
|
|
|
When testing for Hepatitis B virus (HBV), how could you determine if the infection was acute or chronic?
• HBsAg • anti-HBc • IgM anti-HBc • anti-HBs • HBe / anti-HBe |
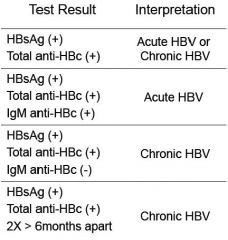
If we have the ANTIGENS for HBsAG and ANTIBODIES for the HB capsule antigen= (+) diagnosis for HepB.
**Again, when IgM present= ACUTE INFECTION*** Clear differential |
|
|
|
What the F*ck is the difference between HBsAg and HBcAg? And why the F*ck do we care?
(Hepatitis B SOLUBLE Antigen and Hepatitis B CAPSULE Antigen) |

Surface protien (Anti-HBs Ig is protective)
Core protein (Anti-HBc Ig is NOT protective) |
|
|
|
Describe differences between GM+ and GM- bacteria. Which stains purple/pink? Which one has teichoic acids? "O antigens"? Thick peptidoglycan layer? Periplasmic space?
|

GM+:
thick peptidoglycan teichoic/lipotechoic GM-: periplasmic space "O antigen" carbohydrate bilayer membrane |
|
|
|
Thinking purely about structure, Which type of bacteria have 90% of their dry weight as PEPTIDOGLYCAN ? Which one have the Lipopolysacharide (LPS) PAMP?
|
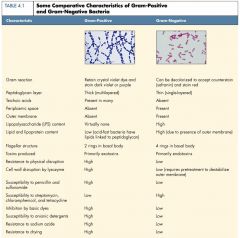
Gram+: 90% dry weight peptidoglycan
Gram -: has LPS |
|
|
|
How can we tell the difference between a bacteria and a virus? Which one do you need an ELECTRON MICROSCOPE to see?
95% of laryngitis are VIRAL infections! Why wouldn't an antibiotic work? |
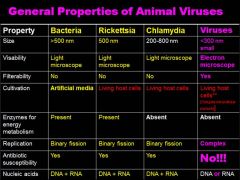
Animal Viruses: >300nm, viruses have FILTERABILITY because they are so small, viruses are NOT SUCEPTIBLE to antibiotics!! (duh) Not subject to the same replication patterns
|
|
|
|
What is the smallest virus? What property do all the small viruses have in common? How about smallest bacteria?
|
The small viruses do NOT HAVE ENVELOPES!
|
|
|
|
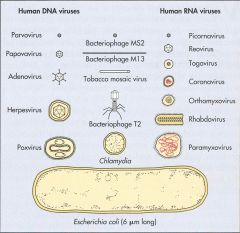
What are all the Human DNA viruses?
(smallest to largest) |
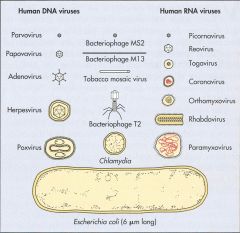
Parvoviridae
Papoviridae Hepadnaviridae Adenoviridae Herpesviridae Poxviridae |
|
|
|
Don't mess up CHICKEN POX and SMALL POX!!! Two different VIRUS types.
Which one is the POXVIRIDAE? What do they have in common? |

Small pox= Poxviridae
Chicken pox= herpesviradae (HHV3/ Varicella-zoster virus) *both linear dsDNA, both large and enveloped |
|
|
|
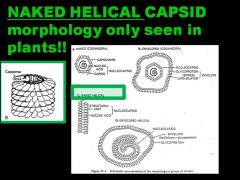
So viruses can come in all shapes and forms in nature: NAKED or ENVELOPED (bud off animal cells)
Different capsid assemblies: ICOSAHEDRAL or HELICAL shape But, what is one morphology that will NEVER BE SEEN IN HUMAN/ MAMMALIAN VIRUSES? |
|
|
|
|
What is it about the RNA viruses that makes it so difficult to find a cure (HIV, Hep C)? Why is their genome type important? What extra tools do they need to have to replicate?
|
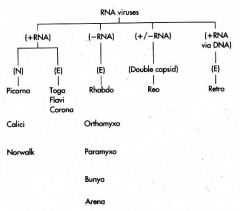
RNA viruses are very prone to mutation!
Cells cannot replicate RNA. RNA viruses must encode an RNA-dependent RNA polymerase The genome structure and polarity determine how viral mRNA is generated and proteins are processed RNA viruses, except (+)RNA genome, must carry polymerase Reoviruses (+/–) segmented DS RNA genome is template for mRNA. (+)RNA may also be encapsulated to generate the (+/–)RNA and then more mRNA Retroviruses (HIV) (+) retrovirus RNA genome is converted into DNA, which is integrated into the host chromatin and transcribed as a cellular gene Picornaviruses, Togaviruses, Flaviviruses, Caliciviruses, and Coronaviruses (+)RNA genome resembles mRNA and is translated into a polyprotein, which is proteolyzed. (–)RNA template is used for replication Orthomyxoviruses, Paramyxoviruses, Rhabdoviruses, Filoviruses, and Bunyaviruses (–)RNA genome is a template for individual mRNAs, but full length (+)RNA template required for replication |
|
|
|
Why is the capsule of the VIRUS so critical in determining the virus's ability to infect?
|
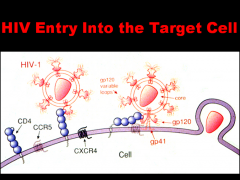
Attachment proteins and receptors are specific for certain viruses; without the proper combination, viruses cannot infect cells OR replicate
The viral envelope (if present) is removed during attachment and penetration A virus cannot be replicated if the capsid is not removed The receptors and attachment proteins are highly specific to certain viruses, the viral envelope is removed during attachment and penetration, and if the capsid is not removed, the virus will not replicate |
|
|
|
Viral phages can release new phage particles when they infect and BURST out of the cell like a motherfuc*er during LYTIC infection, and can VARY in the size of their progeny release.
Why is that? What factors/ length of different stages may cause the burst size to vary in the LYTIC infection? |
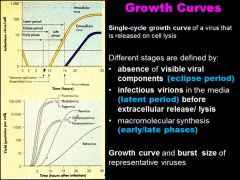
Both the type of virus can affect the burst size. and the length of the eclipse periods + latent periods can vary the amount of virus being made.
|
|
|
|
Retroviruses (RNA virus type) are freaking SCARY. We have the ONCOVIRINAE family that can cause CANCER (transforming virus) and then the LENTIVIRINAE family which is HIV (slow but certain death via immunosuppresion, cylindrical nucleocapsid).
WHY ARE RETROVIRUSES SO DAMN SCARY?! (And incurable) Also, what is the difference between a simple and complex retrovirus? What three elements do we need for this virus to be expressed? |

This provirus INTEGRATES randomly INTO THE HOST CHROMOSOME and becomes a cellular gene!!!
SIMPLE RETROVIRUSES encode gag, pol, and env genes COMPLEX RETROVIRUSES also encode accessory genes (e.g., tat, rev, nef, vif, vpu for HIV) RNA-dependent DNA polymerase (reverse transcriptase) and INTEGRASE enzymes are carried in the virion-- Virus enveloped spherical virion containing two copies of the positive-strand RNA genome Replication proceeds through a DNA intermediate, termed the provirus Transcription of the genome is regulated by the interaction of host transcription factors with promoter and enhancer elements in the long-terminal repeat (ltr) portion of the genome Virus assembles and buds from the plasma membrane Final morphogenesis of HIV requires protease cleavage of gag and gag-pol polypeptides after envelopement |
|
|
|
If you suspect a patient may have herpes, what sort of lab test would you use to diagnose? What would you say if the test was negative?
|
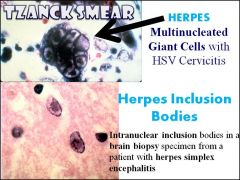
"Tzanck God I don't have herpes."
"Herpes is for life" Use the TZANCK smear to look for MULTINUCLEATED GIANT CELLS or INCLUSION BODIES |
|
|
|
So... herpes is your basic dsDNA virus, with a core, ICOSADELTAHEDRAL capsid, TEGUMENT, and envelope with glycoprotiens...but it can present in many different virus types, alpha, beta, and gamma (HHV 1-8) describe the different general features of each category.
|

|
|
|
|
"Herpes is for life"
- Maddie lee Why? Also, what about the mechanism of infection cause the symptoms? Which immune response (humoral or cell- mediated) are the most important for fighting a herpes infection? Why? |
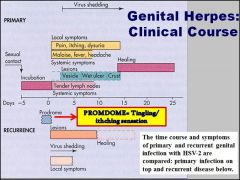
Once exposed to herpes, even though you may be asymptomatic, doesn't mean it infection wont reoccur in same site, reinfect a NEW site, or still be able to transmit the disease to others.
The diesase is spread via SYNCYTIA (cell to cell). During reexposure, viruses hide in cells, so antibodies (B cells) not very effective. CELL MEDIATED (T-CELLS) IMMUNITY IS REQUIRED FOR CONTROL. Virus is reactivated by stress. |
|
|
|
Viruses can jump from animal reservoir hosts in to humans, and then MUTATE (genetic changes occur) to efficiently become more infectious.... What do we call these types of viruses that jump from animals to human? What kind of animal sources do we seem them from?
|
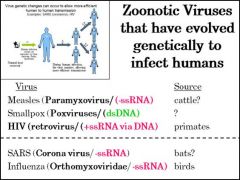
All sort of flavors of Zoonotic viruses
|
|
|
|
What is the difference between a HOST and a NATURAL HOST RESERVOIR for a disease with very little human to human transmission? |
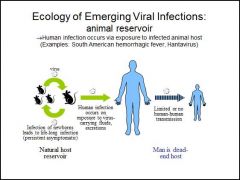
Host reservoir = life long infection (persistent asymptomatic) |
|
|
|
What are the challenges for containing zoonotic/ emerging viruses like EBOLA? Why is CONTAINMENT the most viable option for combating the spread of the virus? |
3 weeks isolation kety! soo unpredictable. Very high nonsocomial transmission. (people also end up being freaked out to go to hospitals!!) |
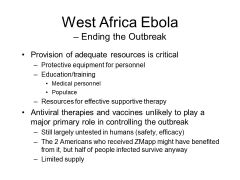
best/ fastest option is to figure out where virus is coming from! |
|
|
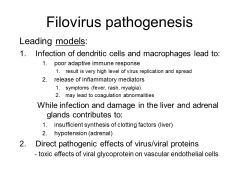
Filovirus (EBOLA) is so freakin scary. It infects the DENDRITIC CELLS and MACROPHAGES. What consequences does this have in the body |
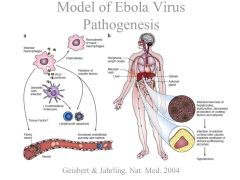
You need both antibody and cell mediated immunity to fully combat the virus!! high viremia, |
|
|
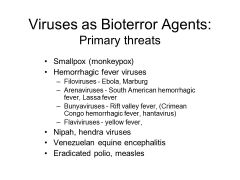
Viral hemmoragic fever can be caused by many different types o viruses, not just ebola (marbug, lassa fever (arenavirus) South American HFV, Rift valley fever, Congo HF, Hantan virus)... what about their symptoms makes them so hard to identify...? |
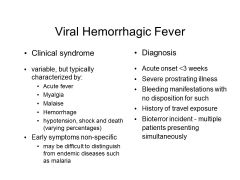
non specific, difficult to ID in areas not endemic to ebola, THE FIRST CASES IN AN OUTBREAK ARE FREQUENTLY MISDIAGNOSED!!! |
|