Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
214 Cards in this Set
- Front
- Back
|
What do the beta cells of the pancreas secrete?
|
Insulin
|
|
|
What do the alpha cells of the pancreas secrete?
|
Glucagon
|
|
|
Insulin
|
Dominates body when full.
Lets glucose into the cells via GLUT carriers. |
|
|
Glucagon
|
Dominates body when not eating.
Only targets liver. Makes it so that blood glucose levels don't crash at night. |
|
|
GLUT-2
|
Found in liver and pancreas.
NOT regulated by insulin |
|
|
GLUT-4
|
Found in muscle, heart, and adipose tissue.
Regulated by insulin. |
|
|
Type 1 diabetes physiology
|
Beta cells of pancreas do not secrete insulin, therefore glucose cannot get into the cells via GLUT-4 which causes increased fat catabolism and protein catabolism.
|
|
|
Type 1 diabetes pathology
|
zero insulin is produced
must inject insulin no insulin resistance b cells are impaired can go into ketoacidosis 1 mil. americans |
|
|
Type 2 diabetes pathology
|
excessive insulin production
might require insulin injections insulin resistant b cells are functioning, but target cells do not respond no ketoacidosis 20 mil. americans |
|
|
Gestational diabetes
|
excessive insulin production
no insulin injecting insulin resistant b cells are functioning no keotacidosis 2-5% of pregnancies |
|
|
Diabetes causes (long term):
|
Blood vessel damage (poor circulation and wound healing, retinal damage and blindness).
Nerve damage (neuropathy) CAD (MI and CVA) Renal failure |
|
|
Adrenal Cortex
|
Endocrine tissue
secretes steriods controlled by anterior pituitary |
|
|
Adrenal Medulla
|
neural tissue
secretes catecholamines controlled by NS |
|
|
Adrenal Medulla secretes:
|
Epinephrine 80%
Norepinephrine 20% Dopamine <1% Epi and Nor Epi come from tyrosine (all amines and neuro hormones) |
|
|
alpha-1 adrenergic receptor
|
IP3 pathway which is stimulated
found many places NE>E (slightly) |
|
|
Alpha-2 adrenergic receptors
|
cAMP pathway which is inhibited.
found many places NE>E (slightly) |
|
|
Beta-1 adrenergic receptors
|
cAMP pathway which is stimulated.
found in the heart E=NE |
|
|
Beta-2 adrenergic receptors
|
cAMP pathway which is stimulated.
Found in liver, lungs, and blood vessels in skeletal muscle and uterus E>>NE |
|
|
Beta-3 adrenergic receptors
|
cAMP pathway which is stimulated.
found in fat (adipose) tissue. E>NE |
|
|
Alpha receptor effects (NE>E slightly)
|
Smooth muscle contraction: vasoconstriction of blood vessels, dilation of pupils, sweating.
gluconeogenesis in liver |
|
|
Beta-1 receptor effects (E=NE)
|
Increase force of heart contractions
increase rate of heart contractions |
|
|
Beta-2 receptor effects (E>>NE)
|
Relaxation of smooth muscle:
vasodilation of blood vessels in skeletal muscle, dilation of lung bronchioles, relaxation of pregnant and non-pregnant uterus, glycogen catabolism in liver |
|
|
Beta-3 receptor effects (E>NE)
|
Fat catabolism
|
|
|
Effects of insulin deficiency #1
|
Decreased glucose absorbtion which causes hyperglycemia, glucosuria, diuesis, electrolyte loss.
|
|
|
Effects of insulin deficiency #2
|
Increased fat catabolism which causes increase in plasma free fatty acids, ketosis, and acidosis. Later leads to dehydration, coma and possible death
|
|
|
Effects of insulin deficency #3
|
Increased protein catabolism which causes abundant deamination, loss of amino acids, very high protein loss.
|
|
|
Circulatory effects of Epineprine
|
Peripherial resistance decrease
Heart contraction force increase Heart contraction rate increase Systolic pressure slight increase Diastolic pressure slight increase Cardiac output increase |
|
|
Circulatory effects of Norepinephrine
|
Peripherial resistance increase
Heart contractiocontraction rate force increase heart contraction rate decrease (baroreceptor reflex) Systolic pressure Increase Diastolic pressure increase Cardiac outupt decrease |
|
|
Pheochromyocytoma
|
Hyper-secretion of catecholamines caused by tumors in the medulla
Elevates both NE and E Causes: Hypertension, headaches, sweating, anxiety, orthostatic hypotension, weight loss |
|
|
Catecholamines in medicine
|
Increase blood flow (beta agonists)
Decrease blood flow (alpha agonists) Increase ventilation of alveoli (beta agonist) Anaphylaxis Examination of eye (alpha agonist) Pregnancy (beta agonist) |
|
|
Adrenal Cortex
|
Secretes glucocortocoids (21c), mineral corticoids (21 C), Androgens (19 C)
|
|
|
Glucocorticoids
|
Increase blood glucose
Increase fat catabolism increase protein catabolism suppress the immune system (cortisol and coricosterone ) |
|
|
Mineralocorticoids
|
Decrease Na+ excretion by the kidneys
(Aldosterone and deoxycorticosterone) |
|
|
Androgens
|
Produce pubic and axillary hair growth in females and contribute to sex drive
(Adrostenedione and dehydroepiandrosterone) |
|
|
Glucocorticoids
|
Primary: Cortisol
Secondary: Corticosterone Synthetics: Prednisone and dexamethasone |
|
|
Mineralocorticoids
|
Primary: Aldosterone
Secondary: Deoxycorticosterone |
|
|
Glucocorticoid secretion and function
|
Raises blood glucose (antagonistic to insulin)
Fat Catabolism Protein catabolism Supress the immune system |
|
|
Cortisol
|
Lets the body deal with chronic stress by supressing immune system.
|
|
|
Mineralocorticoid function
|
Maintain extracellular volume by stimulating Na retention by the kidneys.
Renin and ADH increase together |
|
|
Adrenogenital syndrome
|
Defective glucocorticoids and mineralocorticoid enzymes
No negative feedback > ACTH secretion rises Excessive ACTH results in adrogen synthesis> Masculinization of females (hirisutism, male pattern baldness, small breasts, heavy arms and legs, enlarged clitoris) |
|
|
Cushings syndrome (hyperglucocorticoidism)
|
Caused by over use of exogenous glucocorticoids
S/S: Rapid central obesity, thin limbs, thin skin (high protein catabolism), immunosuppression |
|
|
Addison's Disease
(hypocoricoidism) |
Deficiency of mineralocorticoids and glucocoricoids.
Usually due to autoimmune destruction of the adrenal cortex Reduced cortisol secretion cases and increase in ACTH which can increase skin pigmentation. S/S: hypoglycemia, hypotension and hypovolemia, disturbed mood and behavior. |
|
|
Neurons
|
Cells that transmit electrical signals.
Have various morphologies Axons of a single neuron can be quite long |
|
|
Glial cells
|
Outnumber neurons
Provide physical and metabolic support Assist in neuron repair, growth, and protection. |
|
|
Schwann cells
|
Glial cells of the PNS that produce myelin
|
|
|
Oligodendrocyes
|
Glial cells of the CNS that produce myelin
|
|

What kind of Neuron is this?
|
Multipolar
found in efferent neurons and CNS neurons |
|

What kind of Neuron is this?
|
Multipolar
found in efferent neurons and CNS neurons |
|

What type of neuron is this?
|
Anaxonic
CNS neurons |
|

What kind of neuron is this?
|
Bipolar
afferent neurons |
|

What kind of neuron is this?
|
Pseudounipolar
afferent neurons |
|
|
Where do graded potentials occur?
|
Cell bodies of dendrites
|
|
|
Where do action potentials occur?
|
Axons
|
|
|
Afferent
|
PNS (sensory receptor) to CNS
|
|
|
Efferent
|
CNS to PNS
|
|
|
Neuron Electrical membrane potential
|
-70 MV (called the resting membrane potential)
Negative sign means that it is more negatively charged inside the cell versus outside of the cell |
|
|
at what charge does the concentration gradient cancel out for K?
|
-94 mV (called the equilibrium potential). At this point the amount of K that has had to leave the cell is minute.
|
|
|
at what charge does the concentration gradient cancel out for Na?
|
+60 mV (called the equilibrium potential). At this point the amount of Na that has had to enter the cell is minute.
|
|
|
Nernst Equation
|
E ion= (61 mV/ charge of ion)log (ion out/ ion in)
|
|
|
Depolarizing of cell
|
When cell goes toward the equilibrium potential of Na (+60)
|
|
|
Repolarizing of cell
|
When the cell goes toward the Equilibruim potential of cell (-70)
|
|
|
Hyperpolarizing of cell
|
When the cells electrical charge goes toward K's equilibrium potential (-94)
|
|
|
Graded potentials
|
input signals that get action potentials started and occur in the cell body and in the dendrites.
|
|
|
Action potentials
|
Transmission signals that are produced by graded potentials, travel over long distances, and are found in axons.
|
|
|
Graded Potentials: characteristics
|
Temporary change in membrane potential (+ or -).
Usually occurs in a dendrite or within the cell body. Degrades over a distance. Input signals that can lead to action potentials. |
|
|
Depolarizing Graded potentials
|
Stimulus causes an increase in Na permeability, resulting in Na influx.
|
|
|
Hyperpolarizing Graded potentials
|
Stimulus causes an increase in either K permeability (k efflux) or Cl permeability (Cl influx)
|
|
|
Spatial summation of graded potentials
|
Different graded potentials from different dendrites add up to cause an action potential or can subtract to cancel each other out (a+b= Action potential) (a+c= cancel each other out)
|
|
|
Temporal summation of graded potentials
|
Graded potential from same dendrite causes action potential (a+a= action potential)
|
|
|
Graded Potentials: characteristics
|
Temporary change in membrane potential (+ or -).
Usually occurs in a dendrite or within the cell body. Degrades over a distance. Input signals that can lead to action potentials. |
|
|
Depolarizing Graded potentials
|
Stimulus causes an increase in Na permeability, resulting in Na influx.
|
|
|
Hyperpolarizing Graded potentials
|
Stimulus causes an increase in either K permeability (k efflux) or Cl permeability (Cl influx)
|
|
|
Spatial summation of graded potentials
|
Different graded potentials from different dendrites add up to cause an action potential or can subtract to cancel each other out (a+b= Action potential) (a+c= cancel each other out)
|
|
|
Temporal summation of graded potentials
|
Graded potential from same dendrite causes action potential (a+a= action potential)
|
|
|
Graded potentials can trigger an ________ if the threshold membrane potential _____ is met in the ________
|
Action potiential
-55mV Axon hillock |
|
|
Action potentials can be triggered by _______ and are never triggered by _______
|
Depolarizing graded potentials(stimulating events)
Hyperpolarizing graded potentials (inhibing events) |
|
|
Action potentials are ________ carrying the impulse down the ______
|
Transmission signals
Axon |
|
|
Action potentials are triggered when _______________ are stimulated by reaching the threshold membrane potential______
|
Voltage gated ion channels
-55mV |
|
|
True or false Action potentials are all or none events
|
True, there is no such thing as half of an action potential
|
|
|
True or false Action potentials are capable of summation
|
False, they are incapable of summation
|
|
|
True or False action potientials can travel long distances without losing their signal strength or characteristics
|
True, they can travel the whole body without losing their signal strength or character.
|
|
|
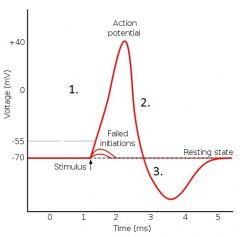
1. Depolarization
2. Repolarization 3. Hyperpolarization |
|
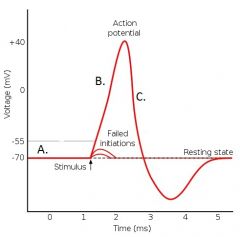
Explain the Na Channel function at A.
|

The activation gate is closed, and the inactivation gate is open. Membrane is polarized below threshold (-55 mV). The channel is closed.
|
|
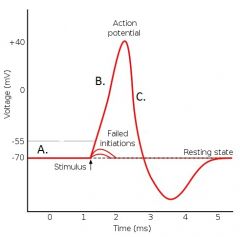
Describe the Na channel at B
|

Threshold of -55mV ismet and the activation gates begin to open, whilethe inactivation gate remains open. Na flows into the cell. The channel is open.
|
|
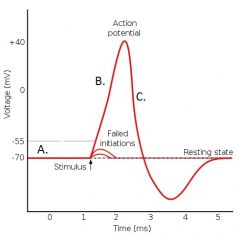
Describe the Na channel at C
|
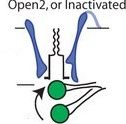
After about 0.5 ms delay, the inactivation gate closes and Na influx stops. The channel is closed. Membrane permeability to K increases causing K to flow out of the neuron and membrane repolarizes.
|
|
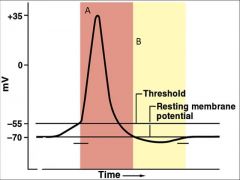
What is A?
|
Absolute refractory peroid. During this period stimuli of any intensity cannot stimulate another action potential. Neuron is unresponsive.
|
|
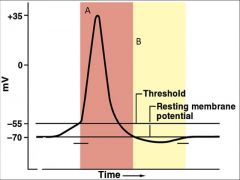
What is B?
|
Relative refractory period. During the relative refractory period only stimuli of higher intensity (bigger depolarizing graded potential) can stimulate another action potential.
|
|
|
Continuous conduction
|
Na channels open as the action potential goes down the axon. One channel causes the rest to open. Like the wave at a football game.
|
|
|
Salatory conduction
|
action potentials jump as they go down the axon due to glial cells surrounding the axon (schwann cells in the PNS or oligodendrocytes in the CNS). Which causes the action potential to speed up.
|
|
|
What are the two ways you can speed up the conduction of an action potential down the axon?
|
Mylenation
Increased diameter of axon. |
|
|
Demyelination
|
Without myelin current (charge) will leak out of the axon and the next node may not reach the threshold.
|
|
|
Multiple Sclerosis
|
Autoimmune of demyelination of the CNS neurons. WHich is the loss of oligodendrocytes.
|
|
|
adrenoleukodystrophy
|
Sex-linked genetic disorder caused by inability to break down fatty acids. The accumulation in these fatty acids in the blood will cause solubilizing and disolving the schwann cells.
|
|

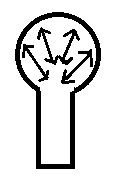
What is this?
|
Convergence of neurons
|
|
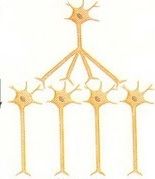
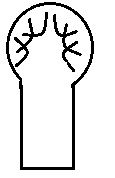
What is this?
|
Divergence
|
|
|
EPSP
|
Excitatory post synaptic potential is equivalent to a depolarizing graded potential
|
|
|
IPSP
|
Inhibitory post synaptic potential is equivalent to a hyperpolarizing graded potential
|
|
|
Super threshold stimulus
|
Many action potentials are produced
|
|
|
Threshold stimulus
|
one action potential produced
|
|
|
Sub-threshold stimulus
|
no action potential produced
|
|
|
Types of neuron symaptic junctions
|
Neuron - Neuron
Neuron - Muscle (neuromuscular) Neuron - Gland Neuron - Organ |
|
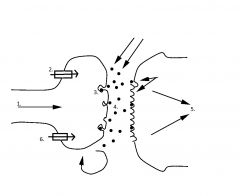
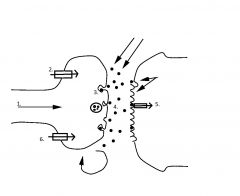
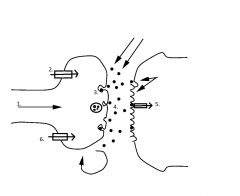
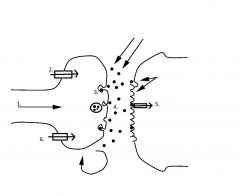
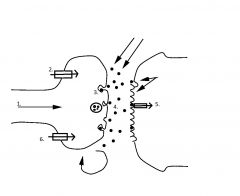
What is happening at 1?
|
Action potential arrives at the synaptic knob.
|
|
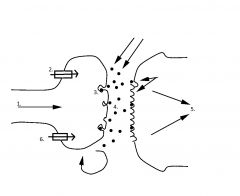
What is happening at 2?
|
Ca channels open, allowing Ca influx
|
|
What is happening at 3?
|
Exocytosis of neurotransmitter into the synapse
|
|
What is happening at 4?
|
Neurotransmitter diffuses across the synapse and binds to a receptor.
|
|
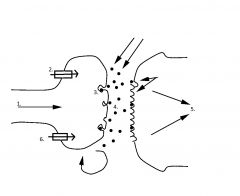
What is happening at 5?
|
neurotransmitter/ receptor complex causes a response in the post synaptic cell.
|
|
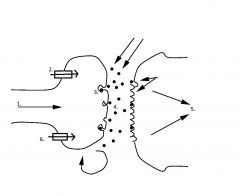
What is happening a 6?
|
Neurotransmitter is either degraded, reabsorbed or diffuses away according to the law of mass action.
|
|
|
Cholenergic receptors
|
Receptors for acetylcholine
|
|
|
Nicotinic receptor
|
Cholenergic receptor
non-specific cation channel controlled by acetylcholine. |
|
|
Muscarinic receptor
|
G- protein pathway that is controlled by acetylcholine.
|
|
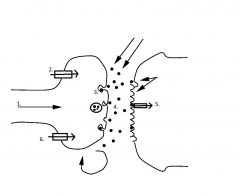
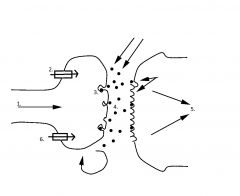
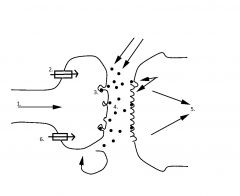
1 in the ACh receptor
|
Action potential arrives at the synaptic knob of the motor neuron
|
|
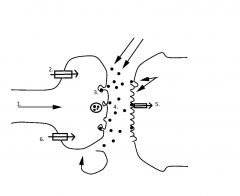
2 in the ACh neuron
|
Ca channels open and Ca flows into the cell down it's electrochemical gradient
|
|
3 in the ACh synapse
|
Acetylcholine is exocytosed into the synapse
|
|
4 in the ACh synapse
|
ACh diffuses across the synapse and binds to nicotinic cholinergic receptors on the post synaptic membrane
|
|
5 in the ACh synapse
|
Nicotinic receptors are non-specific cation channels allowing Na influx and K efflux which results in depolarization of the muscle fiber
|
|
6 in the ACh synapse
|
ACh is degraded by the enzyme acetylcholinesterase (AChE).
|
|
|
Selective Serotonin Reuptake Inhibitors (SSRI)
|
Blocks the reuptake of Serotonin. Makes serotonin have a longer half life in the synapse.
Ex: Zoloft, Paxil, Prozac. |
|
|
Nerve Gases
|
Organophosphates inactive AChE in the cholinergic synapses. Causes spastic paralysis because ACh persists in the receptor which will lead to death because it paralyzes the diaphram.
|
|
|
Tetanus
|
Causes spastic paralysis by inhibiting the action of inhibitory interneurons in the CNS by hyperpolarizing the cell.
|
|
|
Botulism
|
Inhibits the release of ACh from presynaptic motor neurons, causing flaccid paralysis.
|
|
|
Non CNS Capillaries are leaky due to what 3 things?
|
Endothelial pores
Direct diffusion Transcytosis |
|
|
CNS cappilaries are NOT leaky because of what?
|
There are no endothelial pores, instead the endothelial pores are connected through tight junctions which are stimulated to be produced by astrocytes.
|
|
|
What are astrocytes?
|
specialized gial cells which are found in the CNS that stimulate the production of tight junctions between endothelial cells.
|
|
|
How do molecules cross the blood brain barrier?
|
Hydrophobic molecules
or molecules that can mimick a solute (ie: glucose, etc.) |
|
|
ISF and plasma have nearly the same concentration of all solutes except _____
|
Protein
|
|
|
CSF and plasma do not have the same concentration for many solutes, including ____, _____, _____, ______.
|
Glucose
K+ Na+ Protein |
|
|
What is CSF?
|
Intersititial fluid that bathes the brain and spinal cord.
|
|
|
What is grey matter?
|
Found in the exterior of the brain
Cell bodies, dendrites, and synapses (mylenated axons) Integration (EPSP & IPSP) Cerebral cortex Interior of spinal cord. |
|
|
What is white matter?
|
Interior of brain
Myelinated axons Transmission exterior of spinal cord. |
|
What kind of fibers are these?
Where are they found? |
Projection Fibers
Cerebral cortex and the brain stem or spinal cord. |
|
What kind of fibers are these? and where are they found?
|
Association fibers
Different areas of the cerebral cortex. Can only relay information on one hemisphere. |
|
What kind of fibers are these and where are they found?
|
Commissural fibers
Two hemispheres, via the corpus callosum |
|
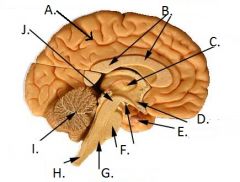
What is A called?
What is it in charge of? |
Cerebrum
conscious thought, sensation, higherprocessing, memory, skeltal muscle movement, emotions, speech interpretation and formation. |
|
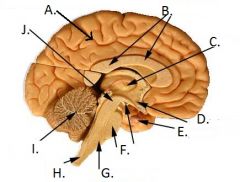
What is B called?
What is it in charge of? |
Corpus callosum
it is in charge of communication between the two hemispheres |
|
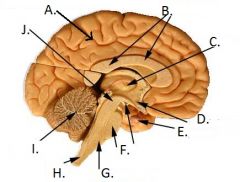
What is C called?
What is it in charge of? |
Thalamus
Sensory intergrating center |
|
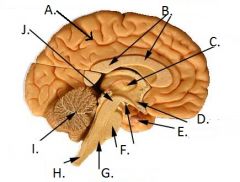
What is D called?
What is it in charge of? |
Hypothalamus
Emotions, homones, homeostasis regulation, hunger, thirst, and sexual responses |
|
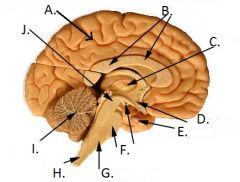
What is F called?
What is it in charge of? |
Pons
a bridge from the cerebellum to the brainstem, coordination and breathing |
|
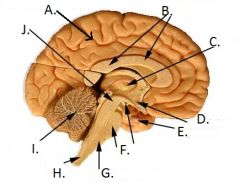
What is G called?
What is it in charge of? |
Medulla Oblongata
Sensory information, control of involuntary functions |
|
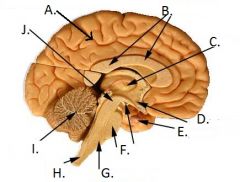
What is I called?
What is it in charge of? |
Cerebellum
Voluntary and involuntary motor activities |
|
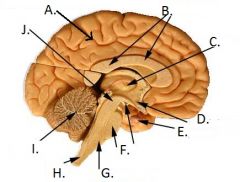
What is J called?
What is it in charge of? |
Midbrain
Visual and auditory information, eye movement |
|
|
What is proprioception?
|
Knowing where your body is in space
|
|
|
What are the ridges of the brain called?
|
Gyri
|
|
|
What are the crevices of the brain called?
|
Sulci
|
|
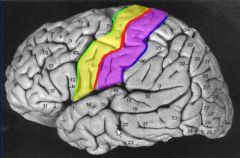
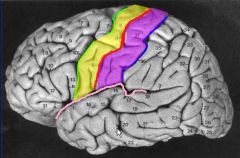
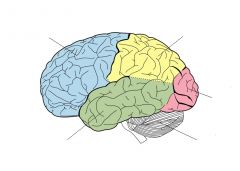
What is the red line called?
|
Central Sulcus
|
|
What is the pink line called?
|
Lateral Sulcus
|
|
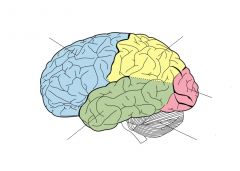
What is the blue lobe called?
|
Frontal lobe
|
|
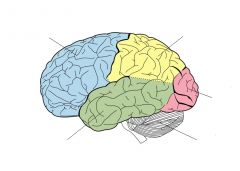
What is the yellow lobe called?
|
Parietal lobe
|
|
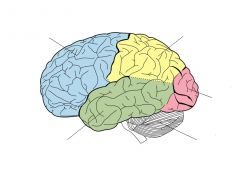
What is the pink lobe called?
|
Occipital lobe
|
|
What is the green lobe called?
|
Temporal lobe
|
|
|
What is the purple area?
What is that cortex for ? |
Post central gyrus
Somatosensory information |
|
|
What is the green lobe called?
|
Temporal lobe
|
|
|
What is the purple area called?
What is that cortex for? |
Post central gyrus
Somatosensory information |
|
|
What is the purple area called?
What is that cortex for? |
Post central gyrus
Somatosensory information |
|
|
What is the purple area called?
What is that cortex for? |
Post central gyrus
Somatosensory information |
|
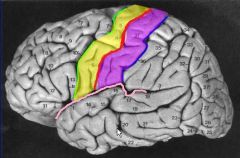
What is the purple area called?
What information does this cortex process? |
Postcentral gyrus
Somatosensory |
|
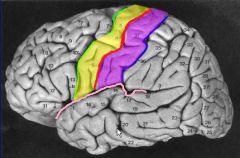
What is the yellow area called?
What information does this cortex process? |
Precentral gyrus
Motor |
|
|
What is the pink area called and what kind of signals does it receive?
|
Dorsal Root
Afferent signals (signals that go to spinal cord) |
|

What is the yellow section called and what kind of signals does it recieve?
|
Ventral root
Efferent signals (signals that go to the body) |
|
|
What is a reflex?
|
Automatic response to a sensory stimulus
|
|
|
What are two ways that reflexes were developed?
|
Conditioned: learned phobias
From birth: kee jerk or withdrawl reflexes |
|
|
What two efferent pathways can reflexes utilize?
|
Autonomic: pupilary dilation, blood pressure (baroreceptor reflex)
Motor: muscle spindle, vomiting, sneezing, withdrawl reflex |
|
|
What are the two CNS integration locations for reflexes?
|
Brain: all complex reflexes like sneezing, phobias, vomiting
Spinal Cord: muscle spindle, withdrawl reflex, erection reflex |
|
|
What two synapses are involved in pathways for reflexes?
|
Monosynaptic: muscle spindle stretch reflex (knee jerk)
Polysynaptic: all other reflexes. |
|

What kind of EEG is this ?
|
REM or awake/ alert
|
|

What kind of sleep wave is this?
|
SWS stage 4
|
|
|
In REM sleep what is the dominant autonomic pathway?
|
Sympathetic
|
|
|
Is there body movement in REM?
|
No, paralysis: arms and legs may infrequently twitch
|
|
|
In REM compare the breathing rate and heart rate as compared to being awake.
|
Elevated
|
|
|
In REM are there dreams?
|
Yes, they are common and detailed (often irrational)
|
|
|
In REM do you sleep walk, have night terrors, or bed wet?
|
No
|
|
|
Are there spontaneuous penile erections during REM?
|
yes
|
|
|
During SWS what is the dominant autonomic pathway?
|
Parasympathetic?
|
|
|
During SWS is there body movement?
|
Yes, usually change of position or posture
|
|
|
Compare your heart and breathing rate during SWS vs. being awake.
|
Decreased
|
|
|
Is there rapid eye movement during SWS?
|
no
|
|
|
Are there dreams during SWS?
|
Less common and vague (often rational)
|
|
|
Do you sleep walk, have night terrors, or bed wetting during SWS?
|
Yes
|
|
|
Are there spontaneous penile errections during SWS?
|
no
|
|
|
What are the steps for sensory reception?
|
Stimulus (pressure, temp, chemicals, light, sound)
receptor responds to the stimulus receptor acts as a biological transducer; converting the stiumulus to action potentials Action potentials fore along afferent neuron |
|
|
What are somatic senses?
|
touch/pressure
propriception temperature nociception (pain) |
|
|
Special senses
|
Vision
Hearing Taste Smell Equilibrium |
|
|
What are chemoreceptors?
|
Receptors that respond to chemicals
ie: O2, pH, etc. Ex: smell, taste, nociceptors |
|
|
What are mechanoreceptors?
|
Receptors that respond to mechanical stimulus
ie: sound, acceleration, stretch, pressure, vibration, proprioception Ex: hearing and touch |
|
|
What are thermoreceptors?
|
Receptors that respond to changes in temperature.
ie: cold or warm |
|
|
What are photoreceptors?
|
Receptors that respond to photons
ONLY found in the eye |
|

What kind of a receptor is this?
|
Simple receptor (somatic)
Ex: nociception |
|

What kind of a receptor is this?
|
Complex receptor (somatic)
Ex: touch, proprioception, vibration |
|

What kind of a receptor is this?
|
Special sense
Ex: vision, hearing, equilibrium, olfaction, gustation |
|
|
What are first order neurons?
|
Neurons that to the CNS from the periphery neurons
|
|
|
What are secondary neurons?
|
Neurons that go from the brainstem (where it entered the CNS) to the thalamus
|
|
|
What are Tertiary neurons?
|
Neurons that go to the post central gyrus.
|
|
|
Sensory nature
|
Type of sensory input
Relies on appropriate sensors CNS determines nature by which neurons are sending action potentials |
|
|
What is synesthesia?
|
CNS misunderstandings of nature, senses get mixed up
Ex: hallucinogenic drugs |
|
|
Sensory location
|
Somatic senses: location on body
Special senses: Location in the visual field, timing between two inputs (smell and sound) |
|
|
Sensory intensity
|
How frequent the action potentials are firing
|
|
|
Sensory Duration
|
How long action potential firing lasts
|
|
|
Olfaction
|
Sense of smell
Primitive sense Least important sense |
|
|
What are the three types of olfactory cells?
|
Olfactory receptor cells
Basal cells Supporting cells |
|
|
Gustation 5 modalities:
|
Sweet
Salty Sour Bitter Umami |
|
|
Where are taste buds found?
|
Tongue, palate, parynx, and epiglottis
|
|
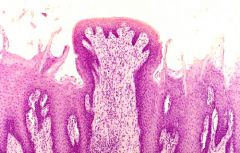
What kind of papillae is this?
|
Fungiform
|
|
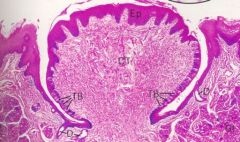
What kind of Papillae is this?
|
Vallate
|
|
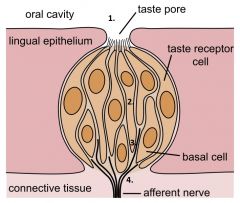
Describe 1 of signal transduction in the taste bud
|
Ligand molecule binds to a receptor on the surface of the cell or enters the cell.
|
|
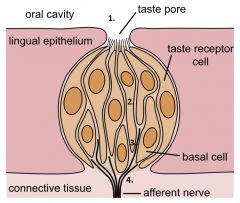
Describe 2 of the signal transduction in taste buds
|
Signal transduction pathway is activated
|
|
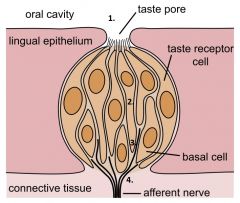
Describe 3 in the signal transduction in taste buds
|
Ca++ enters the cytosol from either the endoplasmic reticulum or from the extracellular fluid
|
|
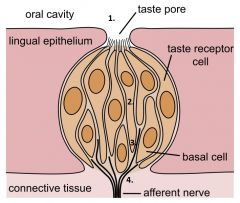
Describe 4 in the signal transduction of taste buds
|
Neurotransmitter is released via exocytosis onto a primary (1st order) sensory neuron
|
|
|
Describe salty signal transduction
|
Na+ in the saliva
Na+ influx into hte receptor cells via Na+ leak channels Cell depolarizes Ca++ channels open Cell depolarizes more Exocytosis of neurotransmitter |
|
|
Describe sour signal transduction in relation to K+ leak channels
|
H+ in the saliva
H+ binds to K+ leak channels K+ channels close Reduced K+ efflux Cell depolarizes Ca++ channels open Cell depolarizes more Exocytosis of neurotransmitter |
|
|
Describe sour signal transduction in relation to H+ leak channels
|
H+ in the saliva
H+ influx into receptor cells via H+ leak channels Cell depolarizes Ca++ channels open Cell depolarizes more Exocytosis of neurotrasmitter |
|
|
Describe sour signal transduction in relation to cation (Ca++ and Na+) leak channels
|
H+ bings to cation leak channels
Cation channels open Increased cation influx Cell depolarizes Ca++ channels open Cell depolarizes more Exocytosis of neurotransmitter |
|
|
Describe sweet signal transduction
|
Simple Carbohydrate in the saliva
Simple carbohydrates bind to a receptor that is linked to the g-protein gustducin Adenylate cyclase is activated cAMP closes K+ leak channels Reduced K+ efflux Cell depolarizes Ca++ channels open Cell depolarizes more Exocytosis of neurotramsmitter |
|
|
Describe bitter signal transduction in relation to K+ channels
|
Bitter ligand (possibly toxic) in the saliva
Ligand binds to K+ leak channels K+ channels close Reduced K+ efflux Cell depolarizes Ca++ channels open Cell depolarizes more Exocytosis of neurotransmitter |
|
|
Describe bitter signal transduction in relation to G-protein transducin
|
Bitter ligan (poss. toxic) in the saliva
Ligand binds to a receptor that is linked to the g-protein transducin Phospholipase C is activated IP3 opens Ca++ channels in the ER Cell Depolarizes Exocytosis of neurotransmitter |
|
|
Describe umami signal transduction
|
Glutamate
activates G-protein Ca++ channels open Cell depolarizes Exocytosis of neurotransmitter |