![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
333 Cards in this Set
- Front
- Back
|
What are the basic anatomical divisions of the nervous system? |
1. Central Nervous System 2. Peripheral Nervous System |
|
|
Neurons and Glia are what? |
These are 2 basic cell types found in the nervous system |
|
|
What is the role of glia? |
1. It acts like glue 2. Provides support for neurons |
|
|
List the 4 types of glia in CNS. What are the important features of each? |
1. Astrocytes: supplies nutrients, ensheath blood capillaries, transmit info 2. Microglia: CNS immune cells, engulfs microorganisms and debris 3. Ependymal cells: line filled spaces of the brain and spinal cord, cilia (hair like processes) circulate CSF 4. Oligodendrocytes: support nerve fibres, ensheath them with myelin |
|
|
What type of glial cell in found in PNS? What is its function? |
1. Schwann Cells 2. They support the nerve fibres and ensheath them with myelin. They are similar to oligodendrocytes. |
|
|
Name the structure that increases our nerves conduction velocity. What kind of material is it composed of? |
1. Myelin Sheath 2. Made of lipid |
|
|
What are the 4 structural components of a neuron? |
1. Dendrites: receive input and send it to cell body 2. Cell body: contains nucleus and organelles 3. Axon: carries electrical impulses 4. Axon terminal: site of neurotransmitter release |
|
|
What is the nodes of ranvier? What is their function? |
1. Gaps in the myelin sheath that increase conduction. 2. It is at these sites that voltage-gated sodium and potassium channels can open to allow these ions to move between the inside and outside of the cell. We refer to action potentials as having "saltatory conduction" which means they jump between nodes of Ranvier. |
|
|
What happens to the myelin in Multiple Sclerosis? What is the cause of this? |
Demyelination due to infection or autoimmunity |
|
|
What are the consequences of multiple sclerosis, in terms of symptoms you might notice? |
1. Weakness 2. Loss of coordination 3. Speech impairment 4. Visual impairment |
|
|
What structures in the neuron can be referred to as the "input zone" and what type of input are they receiving? |
1. Dendrites and cell bodies 2. They are receiving chemical input (neurotransmitter) |
|
|
What structure in a neuron is referred to as the 'summation zone', and what occurs here? |
1. Axon hillock 2. Decision is made whether to transmit the signal further |
|
|
What structure in a neuron is referred to as teh conduction zone, and what type of signal does conduct? |
1. Axon 2. Conducts electrical signal |
|
|
What structures in neurons are referred to as the output zone? Where might they be sending their output and what kind of output will it be? |
Axon terminal Might be sending output to another neuron - or some other cell. Output will be chemical (neurotransmitter) |
|

What type of morphological neuron this is? |
1. Multipolar 2. Multiple processes emanate from the cell body. Multiple dendrites, a single axon |
|

What type of morphological neuron is this? |
1. Bipolar 2. 2 processes emanate from the cell body. 1 functions as dendrite, other functions as axon |
|
|
1. Unipolar 2. 1 process emanates from the cell body, then branches into dendrite and axon |
|
|
What is a synapse? |
The junction where 2 neurons communicate. |
|
|
Synapses can be classified as axodendritic, axosomatic, axoaxonic. \What do these mean and what is the most common in CNS? |
1. Axodendritic: from output zone of pre-synaptic cell to the input zone of of post synaptic. This is the most common 2. Axosomatic: from the axon of the pre-synaptic cell to the cell body of the post synaptic cell 3. Axoaxonic: axon of pre-synaptic to axon of post-synaptic |
|
|
What is the afferent signal? What is another name for this? |
1. A signal that travels towards the brain 2. Also called ascending |
|
|
What is efferent? Another name? |
1. A signal that travels away from the brain. 2. Descending |
|
|
What is the name for the grouping of neuron cell bodies in the CNS? |
Nucleus |
|
|
What is the name for a grouping of axons? |
Tract |
|
|
What is the name for grouping of cell bodies in the cerebral cortex? |
Grey matter |
|
|
What is the name for the grouping of axons in the cerebral cortex? |
White matter |
|
|
What is the name for grouping of cell bodies in the PNS? |
Ganglion |
|
|
What is the name for grouping of axons in the PNS? |
Nerve |
|
|
What are the gross structures of the CNS? |
1. Brain 2. Spinal cord |
|
|
What are the gross structures of the PNS? |
1. Spinal nerves 2. Cranial nerves |
|
|
Describe the somatic nervous system. |
It deals with things we are aware of and have voluntary control over |
|
|
Give an example of and afferent and efferent signal for the somatic nervous system. |
afferent: reading a book efferent: kicking a ball |
|
|
Describe autonomic nervous system. |
It deals with things we are not aware of and do not have voluntary control over |
|
|
Give and example of efferent and afferent signal for the autonomic nervous system. |
afferent: sensing blood pressure efferent: signals to increase heart rate |
|
|
What is a motor unit made of? |
1. a motor neuron 2. the axon and all its branches 3. every muscle fibre that it innervates |
|
|
What does 'fight or flight' describe? |
The function of the sympathetic nervous system. |
|
|
What does 'rest and digest' describe? |
parasympathetic nervous system |
|
|
What are the 2 types of parasympathetic ganglia? |
1. Sympathetic chain ganglia 2. Collateral ganglia |
|
|
How many sympathetic chain ganglia are there? Where are they found? |
1. 21-23 pairs 2. Found alongside the vertebral column |
|
|
Where the spinal column start and end? |
1. Foramen Magnum ---> Inferior border of L1 |
|
|
Name the space within the vertebral column where the spinal cord sits: |
Spinal cavity |
|
|
Name the sack within the spinal cord which the spinal cord extends. |
Meningeal sack |
|
|
Name the tapered structure at the inferior end of the spinal cord |
Conus medularis |
|
|
What is the filum terminale? |
The extension of the meninges that extends from the conus medularis of the spinal cavity and anchors the spinal cord |
|
|
How many spinal nerves do the cervical, thoracic, lumbar and sacral have? |
1. Cervical = 5 2. Thoracic = 12 3. Lumbar = 5 4. Sacral = 5 |
|
|
At what level would the spinal nerves going to the arms and thorax exit the vertebral column? |
Cervical and thoracic |
|
|
At what level nerves going to the legs, pelvis and abdomen exit the vertebral column? |
Lumbar, sacral, coccygeal levels |
|
|
Do the following carry efferent or afferent information? 1. Anterior column 2. Posterior column 3. Lateral column |
1. Efferent 2. Afferent 3. Both |
|
|
Where in the spinal cord to motor neurons reside? |
1. Ventral horns |
|
|
Where in the spinal cord do autonomic motor neurons reside? |
Lateral/ventrolateral horns |
|
|
In what structures do cell bodies of sensory neurons reside? |
Dorsal root ganglia |
|
|
In what direction does info flow in a spinal nerve - is it afferent or efferent? |
1. The nerves head out of the CNS from the ventral roots, and head in via DRG 2. Both - spinal nerves are mixed |
|
|
What structure do the spinal nerves branch into once they leave the spinal column? |
Dorsal and ventral rami |
|
|
List the bones that make up the cranium vault: |
1 Frontal bone 2 Parietal bones 2 temporal bones 1 occipital bone 1 sphenoid bone 1 ethmoid bone |
|
|
List the bones that make up the facial skeleton. How many are there? |
2 zygomatic 2 maxillary 1 mandible 2 nasal 7 internal ones Total = 14 |
|
|
What are the joints between bones of the cranium? |
Sutures: 1. Coronal (frontal - parietal) 2. Squamos (temporal - parietal) 3. Lambdoidal (occipital - parietal) |
|
|
In what group fo humans would sutures be missing? Why are these joints missing? |
1. Sutures are missing in infants. 2. There would be gaps called fontanelles. This allows the brain to grow after birth. |
|
|
Name the 3 layers of meninges: |
1. Dura mater 2. Arachnoid mater (2 layers) 3. Pia mater |
|
|
What are the dural reflections? |
1. These are formed by the inner layer of dura mater 2. Its function is to separate the major divisions of the brain. |
|
|
What is the venous sinus? |
It is the name given to the space between the layers of dura mater |
|
|
Name the dural reflections and state which parts of the brain it separates and what plane it is found in: |
1. Falx cerebri - separating cerebral hemispheres - found in median plane 2. Falx cerebelli - separating cerebellar hemispheres - found in median plane 3. Tentorium cerebelli - separating cerebrum from cerebellum - horizontal plane |
|
|
What in the arachnoid mater looks like spiderwebs? |
Blood vessels |
|
|
What is found in the subarachnoid space? |
CerebroSpinal Fluid |
|
|
What are the arachnoid villi? What is their function? |
1. Granulations of the arachnoid mater. 2. Perforate the dura, transporting ‘old’ CSF from the subarachnoid space to thevenous sinus. |
|
|
What structures of the brain does the pia mater extend into, whereas thearachnoid and dura mater do not? |
Gyri/ Sucli |
|
|
What are the ventricles, and what substance do they contain? |
Network of interconnectedspaces in the brain, containing cerebrospinal fluid (CSF) |
|
|
List the ventricles: |
1. Lateral (left) 2. Lateral (right) 6 3. 3rd ventricle 4. 4th ventricle |
|
|
Where is the CSF produced? |
In the choroid plexus - networks of capillaries that project from pia mater into lateral ventricles and roofs of 3rd and 4th ventricles |
|
|
How much of the CSF is there in adults? |
140mL |
|
|
Describe the flow of this substance, starting from the lateral ventricles and finishing withentry into the venous blood circulation: |
Flows from lateral ventricles to third ventricle, through cerebral aqueduct to fourthventricle. Then through median foramen and two lateral foramina of the 4th ventricle intosubarachnoid space. Enters venous blood circulation within venous sinuses viaarachnoid villi |
|
|
What is Hydrocephalus? |
The clinical condition caused by abnormal accumulation of CSF in the ventricles ofthe brain, causing increased intracranial pressure |
|
|
What is the root cause of Hydrocephalus? |
Blocked aqueduct |
|
|
What obvious clinical signs of this might you observe in younger patients? |
Progressive enlargement of head |
|
|
What other signs and symptoms might be reported for patients with Hydrocephalus? |
• Convulsion • Tunnel vision • Mental disability |
|
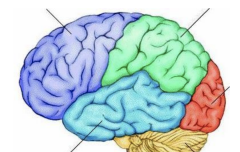
Label these: |
Purple: frontal lobe Green: parietal lobe Blue: temporal lobe Red: occipital lobe Yellow: cerebellum |
|
|
Lobes of the cerebral cortex are separated by sulci. Name the sulcus between: |
• Parietal lobe and occipital lobe: parieto-occipital sulcus • Temporal lobe and frontal/parietal lobes: lateral sulcus • Frontal lobe and parietal lobe: central sulcus |
|
|
Name the fissure between the cerebral cortex and the cerebellum: |
Transverse fissure |
|
|
For each of the lobes of the cerebral cortex below, list the major functions: |
1. Frontal = Emotions, personality, decision making & somatic motor control 2. Parietal = Sensory 3. Occipital = Vision 4. Temporal = Memory, Hearing |
|
|
Describe the frontal lobe in more detail: |
The frontal lobe can be split into the motor cortex and the pre-frontal cortex. The motor cortex is responsible for voluntary movement, and can be furtherdivided into the pre-motor cortex and the primary motor cortex. The pre-motor cortex is involved in planning movement, while the primarymotor cortex (located in the pre-central gyrus is involved in execution ofmovement. Meanwhile, the pre-frontal cortex is involved in decision-making, emotion andanticipating consequences. It is involved in “who we are” so can be affected bymental illnesses such as schizophrenia. |
|
|
The following is a summary of the major internal divisions of the brain. Name the subdivisions included within each: |
• Cerebrum = Cerebral cortex, Corpus callosum • Diencephalon = Thalamus, Hypothalamus • Brainstem = Midbrain, Pons, Medulla oblongata
|
|
|
Name the structure sometimes referred to as the ‘forebrain’: |
Thalamus |
|
|
Name the structures referred to together as the “hindbrain” |
Pons, medulla oblongata |
|
|
Describe the role of the cerebellum in integrating the motor and sensory systems |
Whenthe motor cortex initiates a movement, a copy of the instructions is sent to thecerebellum. The cerebellum then receives sensory information, which allows it tocompare the motor output/intended movement with the actual movement. It canthen adjust the motor output if necessary for coordination. |
|
|
List the basal nuclei: |
• Caudate • Putamen • Globus pallidus • Subthalamic nucleus • Substantia nigra |
|
|
Describe the role of the basal nuclei in integration motor and sensory systems: |
• Select movement • Initiate movement • Terminate movement |
|
|
What is an ion? |
An atom or molecule that carries an electrical charge due to the loss or gain of one or more electrons |
|
|
What is a cation? |
A positively charged atom or molecule |
|
|
Name three important cations in the body: |
• Na+ • K+ • Ca2+ |
|
|
What is an anion? |
A negatively charged atom or molecule |
|
|
Name three important anions in the body: |
• Cl- • HCO3- • Negatively charged proteins |
|
|
What are the two most important cations for neurotransmission? |
• Na+ • K+ |
|
|
What cellular structure creates an electrical potential within the body? How does it do this? |
The cell membrane or phospholipid bilayer. It does this by creating a barrier which prevents ions from freely flowing between the cytosol and the extracellular fluid. There is an uneven |
|
|
What is the typical value for the resting membrane potential (RMP) in living neurons? Which side is negative? |
-70mV inside the cell is more negative. |
|
|
What protein structures in neurons are the equivalent of an “electrical switch”? |
Ion channels |
|
|
How do the ion channels select between Na+ and K+? |
By size. Potassium is larger than sodium. |
|
|
At resting membrane potential, are Na+ channels open or closed? |
Mostly closed |
|
|
At resting membrane potential, are K+ channels open or closed? |
Some open |
|
|
Name the ion pump that carries out active transport in order to assist in the maintenance of RMP. What ions does it exchange? In what direction? What molecule does it use to provide energy for this? |
1. Na+/K+ ATPase or the “sodium-potassium pump”. 2. It transports 3 Na+ outside the cell in exchange for bringing 2 K+ in. 3. Uses ATP to provide energy. |
|
|
What is the most important difference between an ion pump and an ion channel? |
1. An ion pump uses energy to actively transport ions against their concentration gradient (“uphill”) 2. A channel facilitates passive diffusion of ions down their concentration gradient (“downhill”). |
|
|
Is an excitatory local potential depolarised or hyperpolarised? |
Depolarised |
|
|
What channel do we expect to have opened for an excitatory local potential? |
Na+ |
|
|
Is an inhibitory local potential depolarised or hyperpolarised? |
Hyperpolarised |
|
|
What channel do we expect to have opened for an inhibitory local potential? |
K+ |
|
|
What threshold of depolarisation must be reached to trigger an action potential? |
-59mV |
|
|
What approximate maximum depolarisation is reached with an action potential? |
+30mV |
|
|
About how long does it take for the events described above to occur? |
2ms |
|
|
Is amplitude of an action potential lost as it conducts along an axon? |
No |
|
|
What prevents an action potential from ‘going backwards’ back down an axon? |
Refractory periods, which is an intrinsic feature of the sodium channels |
|
|
Name the three phases of the activation cycle of a Na+ channel: |
• Open • Inactive open |
|
|
Name the refractory period in which it is impossible to invoke another action potential |
Absolute refractory period |
|
|
Name the refractory period in which a very large stimulus will be required to invokeanother action potential |
Relative refractory period |
|
|
About how fast is action potential conduction in large mammals? |
50-70m/s |
|
|
Name the type of conduction that occurs in large mammals that makes this increasedconduction speed possible, and name the structures involved: |
Saltatory conduction.This is where an action potential ‘jumps’ between nodes of Ranvier, which aregaps in the myelin sheath. |
|
|
Name some key structural features you would expect to find in the synaptic knob or“Bouton” of a pre-synaptic neuron: |
• Voltage-gated Ca2+ channels • Synaptic vesicles • Mitochondria |
|
|
About how big is the synaptic cleft? |
20-30nm |
|
|
What is the typical concentration of Ca2+ in ECF? |
2-2.5mM |
|
|
What is the role of Ca2+ in neurotransmission? |
Triggers release of synaptic vesicles |
|
|
What type of channels open at the synaptic knob when an action potential arrives? |
Voltage-gated Ca2+ channels |
|
|
After neurotransmitter is released from synaptic vesicles, it diffuses across the synapticcleft and binds to receptors on the post-synaptic neuron. This causes channels to open. Describe what type of signal will be produced if each of the following channels opens: |
• Na+ excitatory • K+ inhibitory • Cl- inhibitory |
|
|
What do we call the local potential of a post-synaptic neuron if there is netdepolarisation? |
Excitatory post-synaptic potential (EPSP) |
|
|
What do we call the local potential of a post-synaptic neuron if there is nethyperpolarisation? |
Inhibitory post-synaptic potential (IPSP) |
|
|
Neurotransmitter is released into the synaptic cleft in excess. Explain what this means inyour own words: |
More is released than is needed for the receptors in thepostsynaptic cell |
|
|
There are three ways that excess neurotransmitter can be removed from the synapticcleft. What are these? |
• Degradation by enzymes • Reuptake into the synaptic knob • Reuptake by glia |
|
|
What structures in the synaptic knob ensure that there is sufficient energy to meet thesignificant energy demands associated with neurotransmitter reuptake? |
Mitochondria |
|
|
What neurotransmitters are affected by methamphetamine, and what is the specificeffect? |
Noradrenaline, dopamine and serotonin. It blocks reuptake of theseneurotransmitters. |
|
|
For each of the following drugs, name the drug target it acts on: |
• Nicotine: nicotinic receptors (brain) • Heroin: opioid receptors • THC: cannabinoid receptors |
|
|
Name two excitatory neurotransmitters: |
• Acetylcholine • Glutamate |
|
|
Name the most common excitatory neurotransmitter in the CNS: |
Glutamate |
|
|
Name the most common inhibitory neurotransmitter in the brain: |
GABA (gamma aminobutyric acid) |
|
|
What type of receptor/s does acetylcholine act on, and in what locations? |
Ligand-gatedNa+ channels in NMJ and brain |
|
|
What type of receptor/s does glutamate act on? |
Ligand-gated Na+ and Ca2+ channels |
|
|
Which ion channel has a metabotropic receptor, and what does this mean? |
K+ channel.A metabotropic receptor is one that acts through a secondary messenger. |
|
|
What ions contribute to IPSP, and in what directions would they flow to achieve this? |
K+flowing out of cell. Cl- flowing into cell |
|
|
What ions contribute to EPSP, and in what directions would they flow to achieve this? |
Ca2+ and Na2+ flowing into cell |
|
|
Approximately how many synapses are there per neuron? |
50,000 |
|
|
Approximately how many neurons do humans have? |
86,000,000,000 |
|
|
What is network divergence? |
When the flow of information through a neural networkextends in different directions from a common point. This is achieved by the branching ofaxons. |
|
|
What is are the functions of divergence in neural networks? |
• Signal amplification • Few control points, allowing coordination |
|
|
What is network convergence? |
When the flow of information in a neural network tends tocome together towards a common point. |
|
|
What is the function of convergence in neural networks? |
• It builds redundancy in, allowing a back-up path for signals to travel |
|
|
Explain briefly why potassium chloride (KCl) is lethal |
It increases the extracellularconcentration of potassium. This destroys the gradient for potassium to leave the cell,which normally allows cells to repolarise following an action potential. If muscle cells areunable to repolarise they cannot contract again. Because heart is muscle, this leads tocardiac arrest. |
|
|
What are the functions of the following types of muscle? |
1. Cardiac: Pumping of blood through the blood vascular system 2. Smooth: Control the movement of fluids in the body 3. Skeletal: Movement, posture, heat, communication |
|
|
Which is the correct order of the following components of skeletal muscle, from smallestto largest? |
1. Myofilament 2. Sarcomere 3. Myofibril 4. Myocyte 5. Muscle |
|
|
What is the name given to the plasma membrane of a muscle cell? |
Sarcolemma |
|
|
What is the name given to the cytoplasm of a muscle cell? |
Sarcoplasm |
|
|
Where in a muscle cell is calcium stored? |
Sarcoplasmic reticulum |
|
|
What is a T-tubule? |
An invagination of the sarcolemma |
|
|
What is the basic contractile unit of a muscle cell? |
A sarcomere |
|
|
How many myofibrils does a single muscle cell contain? |
>1000 |
|
|
How many sarcomeres will be found within a single myofibril? |
About 15,000 |
|
|
What proteins are found in a thin myofilament? |
• F actin strands • G actin molecules • Troponin • Tropomyosin |
|
|
Name the components of a thick myofilament: |
• Myosin • Myosin heads |
|
|
What is a triad? |
A t-tubule sandwiched between two areas of SR |
|
|
What duration of muscle contraction could be supported by the ATP stores typicallypresent in muscle? |
2-4 seconds |
|
|
What additional molecule in muscle can provide energy for resynthesis of ATP? What duration of contraction can be supported by typical stores of this molecule? |
Creatinephosphate. 20 seconds. |
|
|
What does ‘anaerobic’ mean, and what are the anaerobic energy sources for skeletalmuscle? |
Not requiring oxygen. ATP stores, and regeneration of ATP using CP andglucose, are sources for skeletal muscle |
|
|
What metabolic process can convert nutrients to usable energy anaerobically in themuscle, and what by-product is a consequence of this process? |
Glycolysis, followed byconversion of pyruvate to lactate. Lactate is a by-product of this process. |
|
|
What happens to the by-product from (4)? |
It is released into the bloodstream where it isreconverted to glucose via an oxygen-consuming process. |
|
|
Why is energy required for muscle contraction? |
To allow cross-bridgeuncoupling/reenergising of myosin head |
|
|
Why does rigor mortis occur in deceased bodies shortly after death? |
There is no ATP toallow cross-bridges to be released and muscle relaxation to occur. |
|
|
What is a twitch? |
The smallest possible contraction in a muscle, generated by a singleaction potential from a single motor unit. |
|
|
What is a treppe? |
A series of spaced twitches, with increased tension generated in eachsuccessive twitch |
|
|
Why do repeated stimuli cause treppe? |
• Higher Ca2+ in sarcoplasm • Actin-myosin interactions become more sensitive to Ca2+7 • Heat – higher temperatures can produce more tension |
|
|
What is a tetanus? |
A series of closely spaced twitches |
|
|
Compare complete and incomplete tetanus |
In incomplete tetanus the fluctuations from individual twitches are still visible, while in complete tetanus summation is such thatindividual twitches are no longer seen. |
|
|
What is the main mechanism for contraction summation in tetanus? |
The sustained higherlevel of Ca2+ in the SR |
|
|
Most of the time, do most skeletal muscle fibres show twitch, treppe or tetanus? |
Tetanus |
|
|
Define fatigue |
A state of exhaustion (loss of strength or endurance) produced by strenuous muscle activity |
|
|
What is the cause of physiological fatigue? |
ATP depletion, secondary to depletion ofglucose, glycogen & O2. Build up of metabolic by-products: e.g. Pi and lactic acid |
|
|
What is the cause of psychological fatigue? |
Feedback from working muscles to the brain |
|
|
What type of muscle has intercalated discs, and what is their function? |
Function is to join cardiomyocytes together so they can act as a functionalsyncytium. |
|
|
What 2 types of cell junctions are present in intercalated discs |
Desmosomes – mechanical coupling Gap junctions – electrical coupling |
|
|
Describe the spread of depolarisation in the heart, and name the structures that allowthis to be achieved |
Signal originates at the SA (sinoatrial) node, where ‘pacemaker cells’ are intrinsicallyactive without external input. Depolarisation then spreads to the AV (atrioventricular) node and down the Bundle ofHis in the interventricular septum, then to Purkinje fibres (specialised excitablecardiac muscle fibres) to further depolarise the ventricles. |
|
|
Name four components of the ‘mini nervous system’ present in the heart: |
• SA node • AV node • Bundle of His (AV bundle) • Purkinje fibres |
|
|
How are the components in (4) coupled together? |
How are the components in (4) coupled together? |
|
|
What structures in smooth muscle link actin filaments? |
Dense bodies |
|
|
Does smooth muscle have sarcomeres? |
No |
|
|
In what type of smooth muscle units would we find gap junctions to allow spread ofexcitation? |
Single-unit smooth muscle |
|
|
What is the type of smooth muscle units would we find an absence of gap junctions?What advantage does this confer? |
Multi-unit – allowed fine control of individual cells |
|
|
Name three places where the type of smooth muscle unit in (8) is found: |
Digestive tract Urinary tract Reproductive tract |
|
|
Name three places where the type of smooth muscle in (9) is found: |
Pili muscles (skin) Eye muscles Blood vessels |
|
|
If diameter of a blood vessel is doubled, how many times greater will blood flow be? |
16x |
|
|
Describe the mechanism for excitation-contraction coupling in smooth muscle, andcontrast it with that of skeletal muscle. |
Action potential or hormones can provide the rise in cytoplasmic Ca2+. Ca2+ binds to calmodulin The complex of Ca2+ and calmodulin together activates the enzyme MLCK (myosin light chain kinase), which activates MLC (myosin light chain) via phosphorylation.
In smooth muscle, calcium interacts with the myosin myofilament to allow excitationcontraction coupling via an enzyme, while in skeletal muscle the calciuminteracts with the actin myofilament. |
|
|
List the special senses: |
Vision Hearing Taste Smell Vestibular (balance) |
|
|
List the somatic and visceral sensations: |
Touch Pain Warm/cold Body position |
|
|
What are the three methods of information input into the CNS? Give an example foreach |
1. Direct (e.g. temperature sensing in hypothalamus) 2. Endocrine (e.g. control of food intake) 3. Nervous |
|
|
What is a receptor? |
The sensory ending of an afferent neuron, or a specialisedreceptor cell. |
|
|
What four types of information describe a sensory stimulus? |
• Modality – type of receptor activted • Intensity – of AP firing • Duration – of AP firing • Location – of activate receptor |
|
|
Where in the muscle are the length receptors used for proprioception found? |
Muscle spindle |
|
|
Where in the muscle are the tension receptors used for proprioception found? |
Golgitendon organ |
|
|
What effect will increasing a stimulus at a receptor have on the frequency of actionpotentials sent? |
Increase the frequency of action potentials |
|
|
Does stimulus at a receptor always result in an action potential being sent along theafferent neuron’s axon? Why/why not? |
No – below a certain threshold a signal will notbe sent. |
|
|
Will response to a stimulus stay the same over time? Why/why not? |
No – adaptationoccurs, meaning decreased receptor potential over time with continuous stimulation.Receptors are most sensitive to change. |
|
|
What receptors adapt rapidly? |
Touch receptors |
|
|
What receptor adapt slowly? |
Stretch receptors |
|
|
What is receptive field? What test can be used to estimate the size of receptive fieldon an area of a patient’s body? |
Region of a space where a stimulus can lead toactivity in a particular afferent neuron. Two-point discrimination test. |
|
|
Compare the size of receptive field for fast/acute pain and slow/chronic pain: |
Fast/acute pain has small receptive field. Slow/chronic = larger receptive field. |
|
|
Describe the axons that nociceptors for fast/acute pain send signals through. What isthe name for these fibres? |
Largeish, myelinated axons. ‘A fibres’ |
|
|
Describe the axons that nociceptors for slow/chronic pain send signals through. Whatis the name for these fibres? At what speed do signals conduct? |
Small, unmyelinatedaxons. B fibres. Slow! ~1m/ |
|
|
Which type of pain is associated with somatic pain? |
Fast/acute pain |
|
|
Which type of pain is associated with visceral pain? |
Slow/chronic pain |
|
|
What is a reflex? |
A predictable, reproducible, automatic response to a particularsensory stimulus |
|
|
What is the stretch reflex triggered by? |
Stretch! Detected by stretch receptor inmuscle spindle. |
|
|
In the withdrawal reflex, what happens first - withdrawal, or perception of the stimulusby the brain? |
Withdrawal – the reflex occurs faster than the signal can make it to thebrain |
|
|
In the withdrawal reflex, what happens ipsilaterally? |
Interneurons and afferentneurons excite flexors, inhibit extensors. |
|
|
In the withdrawal reflex, what happens contralaterally? |
Interneurons and afferentneurons excite extensors, inhibit flexors. Stabilise. |
|
|
Which extrapyramidal pathway excites flexors and inhibits extensors? |
Rubrospinaltract |
|
|
Name the basal nuclei |
Lentiform nucleus Caudate nucleus Amygdaloid nucleus |
|
|
At rest, what are the basal nuclei doing? |
Inhibiting the motor cortex |
|
|
How is this overcome upon deciding to move? |
Cortex inhibits inhibitor |
|
|
Which division of the NS allows excitatory or inhibitory signals? |
Autonomic |
|
|
Where do sympathetic pre-ganglionic neurons emerge from the spinal cord? |
Thoracolumbar regions |
|
|
Where do parasympathetic pre-ganglionic neurons emerge from the spinal cord? |
Craniosacral |
|
|
What is a cholinergic neuron? |
Has acetylcholine as NT |
|
|
What is an adrenergic neuron? |
5. What is an adrenergic neuron? |
|
|
Are parasympathetic neurons cholinergic or adrenergic? |
Cholinergic |
|
|
Are sympathetic neurons cholinergic or adrenergic? |
can be both |
|
|
What type of receptor is ionotropic? What is the effect? |
Nicotinic cholinergic.Excitatory. |
|
|
Name three types of receptors that are metabotropic? What is their effect? |
Muscarinic cholinergic Alpha-adrenergic Beta-adrenergic |
|
|
Are preganglionic neurons excitatory or inhibitory? What are they exciting orinhibiting? |
Excitatory. Excite neurons. |
|
|
Are postganglionic neurons excitatory or inhibitory? What are they exciting orinhibiting? |
Either. Exciting or inhibiting effectors. |
|
|
What organs have dual autonomic innervation? |
Iris and lens Heart Bronchi GI tract Bladder Genitals |
|
|
What organs are exclusively subject to sympathetic innervation? |
Sweat glands Blood vessels Hairs Adrenal medulla |
|
|
Where is adrenaline released from? How is this area innervated by the autonomicnervous system? |
Adrenal medulla. Directly from first neuron in spinal cord (i.e. not viapostganglionic neuron) |
|
|
In which areas of the brain are autonomic control centres located? |
Frontal lobe Limbic system Hypothalamus |
|
|
What reflexes are under autonomic control? |
Baroreceptor reflex Light reflex |
|
|
Is any aspect of autonomic activity voluntary? |
Arguably - via self-regulation of emotionalresponses |
|
|
Describe what happens in the light reflex when it is light? Describe the sequence of event, the structures involved, and their locations. |
Signal travels via parasympathetic fibres of oculomotor nerve III, synapse in ciliary ganglion,travels to pupillary constrictor with cholinergic stimulation |
|
|
Describe what happens in the light reflex when it is dark? Describe the sequence ofevent, the structures involved, and their locations. |
Signal travels to spinal cord, adrenergic stimulation of pupillary dilator occurs |
|
|
Describe what happens in the baroreceptor reflex when high blood pressure is detected |
Stretch receptors in arterial wall in carotid sense increased blood pressure.Glossopharangeal nerve synapse in medulla with interneurons which signal to vagus nerve tochange heartrate. Increase parasympathetic stimulation– slow heartrate. Decreasesympathetic stimulation to blood vessels, causing vasodilation. |
|
|
What is the function of the endocrine system? |
Regulates the internal environment by secreting hormones that travel through the bloodstream to target areas. |
|
|
What are the components of the endocrine system? |
Endocrine cells (glands) Hormones Blood vessels Target cells |
|
|
What are hormones? |
chemical messengers produced in one location and transported to a second location (target cells) where they exert their effects |
|
|
What proportion of hormones are peptides? |
75% |
|
|
Name two chemical classes of water-soluble hormones: |
Peptide hormones Catecholamines |
|
|
Name two chemical classes of lipid-soluble hormones |
Steroids Thyroid hormones |
|
|
Which class of hormones is made and stored until required? |
Water-soluble |
|
|
Describe the sequence of events following receptor activation for water-soluble hormones,from receptor activation to cellular response: |
1. Hormone binds to receptor 2. This activates associated G-protein, it binds toguanosine triphosphate (GTP) 3. Which activates adenylyl cyclase 4. Which convertsATP to cyclic Adenosine Monophosphate (cAMP) 5. Which activates protein kinases– set of enzymes that activate other enzymes 6. Which activates the specific enzyme 7. Which converts specific substrate to product |
|
|
Describe the effect adrenaline has when binding to receptors on liver cells |
Triggers therelease of messenger molecules that activate enzymes and result in the release of glucoseinto the bloodstream |
|
|
Describe the sequence of events following receptor activation for lipid-soluble hormones |
1.Lipid-soluble hormone dissociates from carrier protein 2.Hormone diffuses across cellmembrane 3.Hormone binds to INTRACELLULAR receptor 4.Hormone-receptor complexacts as a specific transcription factor 5.New mRNA is generated 6.New protein isgenerated by translation of mRNA 7.New protein mediates cell’s specific response(SLOW PROCESS) |
|
|
Where are the receptors for lipid-soluble hormones located? |
Intracellularly |
|
|
Are water-soluble or lipid-soluble hormones faster-acting? How fast is each? Why? |
Watersolubleis faster. Milliseconds to minutes. Lipid-soluble slower. Hours-days. Because lipidsolublerelies on alteration of gene transcription which takes longer - whereas watersolubleis altering enzyme activity, which can happen more rapidly. |
|
|
What determines a cell’s sensitivity to a particular hormone? |
Number of receptorsexpressed on cell surface |
|
|
Compare and contrast nervous and hormonal control systems? |
Neuronal: Targetingachieved by specific ‘wiring’. Fastest transmission speed, to minimize response delays -When conditions are changing rapidly, response delay can lead to tissue damage, and toinstability of control. Good for brief responses. Hormonal: Targeting by expression ofspecific receptors on target cells. Relatively slow, but long lasting action. Good forwidespread and sustained responses. |
|
|
Describe the location of the pancreas |
In abdomen. Head and neck are in C-shaped curveof duodenum, and body extends behind stomach. |
|
|
The pancreas is both an exocrine and endocrine gland. What is meant by this? |
Endocrineglands secrete their products into the blood. Exocrine glands secrete their products intoducts opening onto an epithelium. |
|
|
What part of the pancreas is endocrine? What proportion of the mass of the pancreas doesthis account for? |
Pancreatic islets. 2% of mass |
|
|
What cells in the pancreas secrete insulin? |
Beta cells |
|
|
What cells in the pancreas secrete glucagon? |
Alpha cells |
|
|
Into what structure are the exocrine secretions of the pancreas released? |
The duodenum, via the pancreatic duct |
|
|
Describe the body’s hormonal response to raised blood glucose, noting which chemicalsare released, from where, to where, what cells are effected and the result |
Beta cells ofpancreatic islet release insulin into blood. Liver takes up glucose and stores it as glycogen,and body cells take up more glucose. Blood glucose returns to set point, reducing thestimulus for further insulin release. |
|
|
Describe the body’s hormonal response to lowered blood glucose, noting which chemicals are released, from where, to where, what cells are effected and the result |
Alphacells of pancreatic islet release glucagon. This causes liver to break down glycogen,releasing glucose into blood. Blood glucose level rises to set point, reducing the stimulusfor further glucagon released. |
|
|
List the target cells for insulin and the respective cellular effects |
• Muscle: increased glucose uptake • Adipose tissue: increased glucose uptake |
|
|
What chemical type of hormone is insulin? |
Protein hormone |
|
|
Is insulin is response to changes in blood glucose an example of positive or negativehomeostatic feedback? |
negative |
|
|
What are the target cells for glucagon, and what effects does it exert there? |
Liver cells. Increases glycogenolysis, gluconeogenesis and ketone synthesis |
|
|
Increasing concentrations of two things inhibit the further release of glucagon. What arethose things? |
• Blood glucose • Blood ketones |
|
|
What other hormones affect blood glucose levels? |
• Growth hormone • Adrenaline • Cortisol |
|
|
What happens in insulin resistance due to long term high blood sugar? |
Malfunctioning ofthe insulin receptor sites can occur, meaning that although insulin is present, binding andthe subsequent signalling cannot properly occur |
|
|
What is the long term impact of insulin resistance on the pancreas? |
Impaired beta cell function |
|
|
Which scientists first extracted insulin, and from where? |
Banting & Best, from a dog |
|
|
What proportion of patients with Diabetes Mellitus have Type I? |
~10% |
|
|
What are the symptoms of Diabetes Mellitus Type I? |
• Hyperglycaemia • Glycosuria • Polyuria • Polydipsia • Polyphagia |
|
|
When is Diabetes Mellitus Type I typically diagnosed? |
In childhood |
|
|
What is the typical treatment for patients with Diabetes Mellitus Type I? |
Insulin injections |
|
|
What is Diabetes Mellitus Type II? |
Form of diabetes where cells are resistant to insulin’s signal to store fuel |
|
|
What is the typical treatment for patients with Diabetes Mellitus Type II? |
Lifestyle changes, drugs promoting insulin release such as incretins, insulin injections (more advanced diabetes) |
|
|
What is the adenohypophysis? |
Anterior lobe of pituitary gland |
|
|
What is the neurohypophysis? |
Posterior lobe of pituitary gland |
|
|
How is the hypothalamus connected to the posterior lobe of the pituitary? |
By neurons |
|
|
What determines the rate of hormone secretion from the posterior pituitary? |
Frequency of action potentials 5 |
|
|
Where are posterior pituitary hormones manufactured? |
Hypothalamus - in cell body of neuron |
|
|
Where are posterior pituitary hormones stored until needed? |
End of axon in posterior pituitary |
|
|
What is the effect of ADH? |
Increases reabsorption of water in the kidney tubules |
|
|
What are two effects brought about by oxytocin? |
Stimulate contraction during childbirth Stimulates milk release in breastfeeding |
|
|
What is the effect of ADH in the tubular cells of the kidneys? |
Expression of aquaporins results in increased water reabsorption, decreasing loss of water in the urine |
|
|
How are electrical synapses linked? |
1. they are linked by gap junctions 2. VERY FAST synapses |
|
|
How are chemical synapses linked? |
1. linked by chemical transmitter 2. slower than electrical but still fast |
|
|
How does suckling trigger release of oxytocin and milk ejection? |
Nervous input in breastcauses long feedback loops via spinal cord to hypothalamus -> release of oxytocin fromposterior pituitary -> milk ejection |
|
|
How is the hypothalamus connected to the posterior pituitary? |
By neurons |
|
|
How is the hypothalamus connected to the anterior pituitary? |
By blood vessels |
|
|
What two broad types of chemicals does the hypothalamus use to communicate with theanterior pituitary? |
Releasing hormones and inhibiting hormones |
|
|
Where are anterior pituitary hormones produced? |
In the endocrine cells of the anteriorpituitary |
|
|
What class of hormones are anterior pituitary hormones? |
Water soluble – peptidehormones |
|
|
How are anterior pituitary hormones released? |
A releasing hormone binds to receptor oncell membrane and the hormone is exocytosed |
|
|
Where do these chemicals get released in order to travel to the anterior pituitary? How do they travel there? |
Median eminence. Travel via bloodstream (portal veins) |
|
|
Name the hormone which inhibits prolactin secretion |
Dopamine |
|
|
What cells produce this hormone? |
Dopamine neurons |
|
|
Where is this hormone referenced released? |
At the median eminence |
|
|
What stimulates the release of this hormone? |
Presence of prolactin in the bloodstream(i.e. negative feedback) |
|
|
Name two major actions of prolactin |
• Stimulation of breast development • Stimulation of milk synthesis |
|
|
Name a hormone that stimulates the release of prolactin |
Prolactin releasinghormone/factor |
|
|
What physical stimulus in breastfeeding triggers the release of relevant hormones? |
Stimulation of nipple mechanoreceptors by the suckling of the infant |
|
|
What posterior pituitary hormone is released in breastfeeding, what is the effect, and bywhat mechanism? |
Hormone: Oxytocin • Effect: Milk ejection • Mechanism: Contraction of myoepithelial cells |
|
|
What is the result of neural input in suckling on hypothalamus release of PIH and PRH(aka PRF)? |
PIH decreases, PRH/PRF increases |
|
|
What does this change cause at the anterior pituitary? |
Increased prolactin secretion |
|
|
What is the effect of increased plasma prolactin on target tissues in breastfeeding? |
Stimulates milk synthesis in the gland cells |
|
|
What hormone stimulates the release of growth hormone (GH)? |
GHRH |
|
|
What hormone inhibits the release of GH? |
Somatostatin |
|
|
What protein released from the liver produces growth effects and also feeds back on thehypothalamus to alter the release of the hormones in (22) and (23)? |
IGF-1 |
|
|
What type of hormone is GH? |
Peptide hormone |
|
|
What layer of the adrenal cortex secretes aldosterone? |
Glomerulosa |
|
|
What layer of the adrenal cortex secretes cortisol? |
Fasiculata |
|
|
What layer of the adrenal cortex secretes androgens? |
Reticularis |
|
|
What type of chemical is cortisol? |
Glucocorticoid |
|
|
Describe the mechanism of action for cortisol? |
1. Cortisol in blood bound tocarrier protein. 3. Binds to receptor in cytoplasm. 4.Hormone-receptor complex migrates to nucleus. 5. Binds to DNA. 6. Transcription ofspecific genes is activated. |
|
|
What is the effect of cortisol in muscle tissue? |
Stimulates breakdown of muscle protein |
|
|
What is the effect of cortisol in liver tissue? |
Increased expression of enzymes involved ingluconeogenesis. Liver makes and releases more glucose into bloodstream. |
|
|
What is the effect of cortisol on fat mobilisation? |
Increases |
|
|
List 3 effects of cortisol in addition to the metabolic effects discussed |
• Helps cope with stress • Suppresses immune system • Helps maintain normal BP |
|
|
What hormone of the hypothalamus starts the chain of events that triggers cortisolsecretion? |
Corticotropin releasing hormone |
|
|
What two stimuli cause the release of the hormone in (10)? |
• Normal daily variation (day-night rhythm, changes in blood glucose) • Abnormal stress |
|
|
What anterior pituitary hormone is released in response to arrival of the hormone in (10)? |
Adrenocorticotropic hormone |
|
|
How long do the effects of cortisol take to develop after cortisol binds to a receptor on thecell membrane of a target cell? |
Minutes to days |
|
|
Describe the function of cortisol in the body |
Influence changes that occur in response tostress, including blood glucose, macronutrient metabolism, immune responses, antiinflammatory actions, blood pressure, heart and blood vessel tone and contraction,and CNS activation |
|
|
Describe the daily pattern of cortisol release |
Pulses during day in response to normalevents or stresses. Increases during sleep and reaches highest peak upon waking.Therefore affected by sleep disturbances. |
|
|
Describe signs and symptoms that may be exhibited with low cortisol |
• Brain fog, cloudy-headedness, mild depression • Low thyroid function • Fatigue (morning, mid afternoon) • Sleep disruption • Low BP • Lowered immune function • Inflammation |
|
|
What clinical condition can be caused by low cortisol or aldosterone? |
Addison’s disease |
|
|
What are the symptoms of the disease in addison's disease? |
• Hyperpigmentation of the skin • Low blood glucose • Low BP • Unexplained weight loss • Fatigue • Low blood sodium • High blood potassium |
|
|
What clinical condition can be caused by high cortisol? |
Cushing’s syndrome |
|
|
What signs and symptoms would you expect to see with the condition in Cushing Disease? |
• Weight gain • High blood glucose • High BP |
|
|
What hormones are released from the adrenal medulla in the stress response? |
Epinephrine (adrenaline) |
|
|
Name the cell type in the adrenal medulla that releases adrenaline (epinephrine) into thebloodstream |
Chromaffin cell |
|
|
What is the function of the endocrine release of epinephrine in the stress response? |
Supplements the actions of direct sympathetic innervation of tissues |
|
|
What are the metabolic effects of epinephrine in skeletal muscle and liver? |
Breakdown ofglycogen to glucose |
|
|
What are the metabolic effects of epinephrine on fat mobilisation? |
Increases breakdownof stored fat to fatty acids |
|
|
What type of receptor does epinephrine bind to on target cells? |
GPCR (G proteincoupled receptor) |
|
|
Compare and contrast the responses of the adrenal cortex and the adrenal medulla instress |
Adrenal medulla releases stored epinephrine. Response is quick (why? Becauseit’s stored, and water-soluble). It acts via membrane receptors and secondarymessengers to make fuel available to body. Adrenal cortex secretes cortisol, which mustbe synthesised when needed. This response is slower. The receptors are intracellularand binding of cortisol activates gene transcription. Also makes fuel available. |
|
|
Describe the location of the thyroid gland |
just below the larynx, on the anterior and lateralsurfaces of the trachea |
|
|
Name the hormones produced and secreted in the thyroid gland |
thyroid hormone,calcitonin |
|
|
Describe the microscopic structure of thyroid gland tissue |
Thyroid gland composed ofsmall spherical sacs or follicles. Each follicle is surrounded by follicular cells. |
|
|
What do follicular cells secrete, and to where? |
Thyroglobulin, into the follicle |
|
|
What do parafollicular cells secrete, and to where? |
Calcitonin, into blood vessels |
|
|
What chemical element binds to the substance referenced in thyroglobulin, and what is the result? |
Iodine. The iodised TGB moves into the follicular cells, and thyroid hormones arereleased |