![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
425 Cards in this Set
- Front
- Back
|
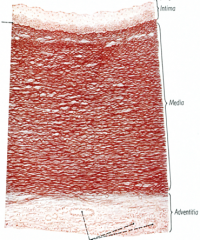
tunica intima characteristics |
endothelial cells, underlying CT inner elastic lamina (smooth muscle) longitudinal |
|
|
tunica media characteristics |
smooth muscle elastic lamina/ fiber external elastic lamina (SM): help regulate BP between intima and adventita no fibroblast, so everything is produce by SM circular |
|
|
tunica adventitia characteristics |
connective tissue blood vessels, nerves (most outer) has fibroblast longitudinal |
|
|
artery v. vein |
artery: thick wall (TM), TA thinner and circular (high pressure) vein: thin walls (TM), TA thicker and less circular |
|
|
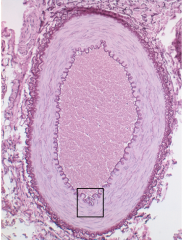
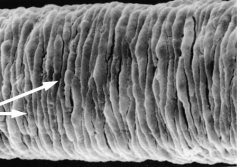
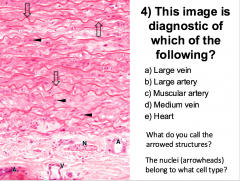
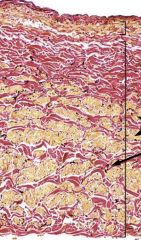
elastic arteries |
large variation in size, full with elastic lamina in media and none in TA large media size allow vessels to expand when heart contract and constrict when heart relax own nerve and blood supply =large arteries |
|
|
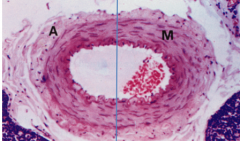
muscular arteries characteristics |
has inner elastic lamina and external elastin lamina 10-40 layers of SM reduce pulsatile flow expand during systoly SM in TM |
|
|
muscular arteries |
|

|
muscular arteries |
|
|
small arteries characteritics |
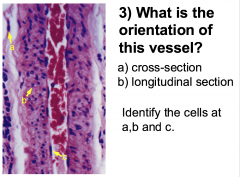
3-10 layers of SM inner elastic lamin in larger one endothelial cell runs along with the longitudinal side, and smooth muscle cells run the other way |
|
|
small arteries |
|
|
small arteries |
|
|
small arteries |
|
|
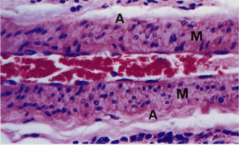
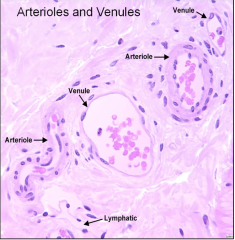
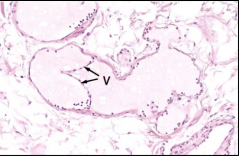
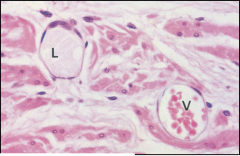
arterioles characteristics |
<3 layer of SM no elastic laminae and associated with accompanying venule look for a ring of pink (SM since its eosinophillic) |
|
|
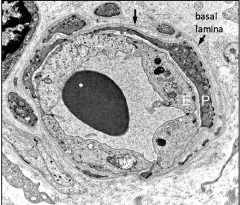
capillaries characteristics |
endothelial (only) and basal lamina no T media or adventita usually only big enough for RBC continuous, fenestrated, discontinuous exchange can occur |
|
|
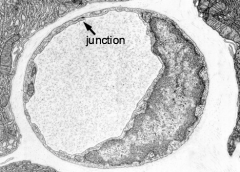
continuous capillary |
ex. nervous system, muscle CT tight junctions at the end of endothelial cell not leaky (most of capillaries) vesicles aka muscular capillaries |
|
|
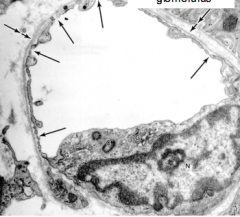
fenestrated capillaries |
ex. endocrine glands, kidney pores allow small molecule to escape |
|
|
discontinuous capillaries |
aka sinusoidal lymphodes, liver large gaps/ openings, big enough for RBC and WBC to go through |
|
|
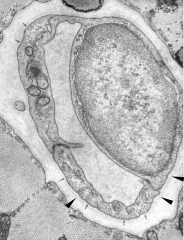
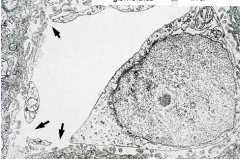
pericytes |
within basal lamina and accompany capillary regulate permeability, contractile, control endothelial proliferation (via gap junction) can't tell between endothelial and pericytes nucleus |
|
|
pericytes |
|
|
venules characteristics |
endothelial cell wall no media and adventitia leaky (lymph and interstitial fluid escape) and histamine sensitive |
|
|
aterioles has smooth muscles, so the pink ring around it |
|
|
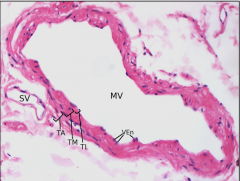
small/medium veins characteristics |
endothelial cell and sooth muscles in T. media thick adventitia have valves |
|
|
small/medium veins |
|

|
valves in small/medium veins |
|
|
varicose veins characteristics |
when valves fail, blood cannot travel as smoothly superficial veins |
|
|
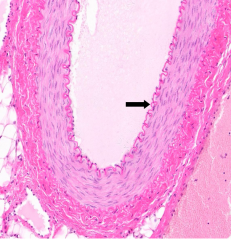
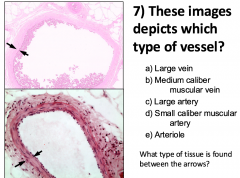
large veins characteristics |
ex. vena cava, brachiocephalic TI: endothelial TM: endothelial TA: smooth muscles (diagnostic, longitudinally) could have elastic fiber in TM or TA not continuous SM |
|
|
portal systemcharacteristics |
capillary bed separate two other vessels capillary --> vessel --> capillary --> heart |
|
|
Heart wall characteristics |
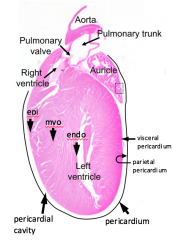
epicardium (TA)--> myocardium (TM) --> endothelium (TI) |
|
|
parietal v. visceral pericardium |
parietal: surface that faces the heart |
|
|
endocardium |
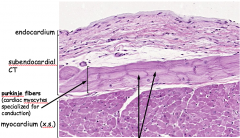
where purkinje fibers
|
|
|
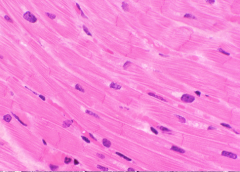
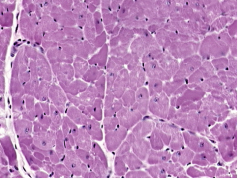
myocardium |
|
|
myocardium |
|
|
epicardium |
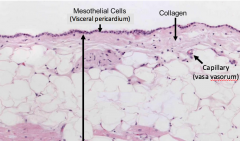
little fluid |
|
|
Atherosclerosis |
focal thickening of intima, accumulation of ECM macrophages, SMC, cholestrol, prone to induce clotting complication: myocardial infarct, angina, conductive anomalies |
|
|
what happen when cardiac muscle dies |
replace with fibrous CT |
|
|
where do purkinje cells lie in heart |
subendocardial CT |
|
|
function of cardiovascular system |
nutrion/metabolic (nutrient transport, gas exchange, waste removal, H distribution) protective (distribute immune cell, clotting) homeostasis (body temp/ brown fat, pH/ pressure regulation) |
|
|
Forces that allow blood return to heart (feet back to heart) |
skeletal muscle contraction one way valve |
|
|
microvasculature pathyways |
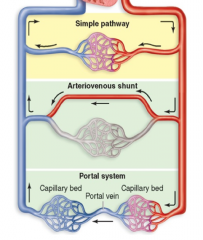
simple arteriovenous shunt (prevent loss of heat by shutting down capillaries/ thermoregulation) portal system (ex. hepatic): capillary --> vein --> capillary--> vein |
|
|
continuous capillary |
|
|
continuous capillary |
|
|
fenestrated capillary |
|
|
discontinuous capillary |
|
|
muscular arteries |
|
|
B cell a: fibroblast cell b: SM cell c: endothelial |
|
|
elastic=large arteries part of TM arrow: elastic fiber nuclei = SM |
|
|
elastic arteries |
|
|
vasa vasorum |
vessels of the vessels |
|
|
deep vein thrombosis |
big thrombi blocking the vein, may cause by lack of moving or defect in clotting blood clots in your veins can break loose, travel through your bloodstream and lodge in your lungs, blocking blood flow (Pulmonary metabolism ) |
|
|
large veins (cross sectional) |
|
|
B lumen to wall ratio is large --> vein TM>TA--> vein between the arrows: SM |
|
|
lymphatics |
|
|
lymphatics and venule |
|
|
lymphadema |
can be caused by lymphatic blockage/ damage (Ex. elephantiasis) or lymphadenectomy |
|
|
where does coronary arteris travel in |
epicardium |
|
|
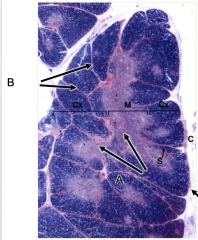
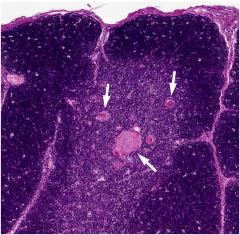
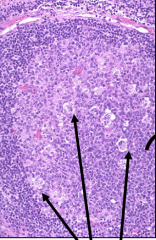
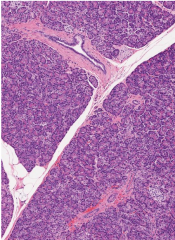
thymus A: medulla B: septa |
|
|
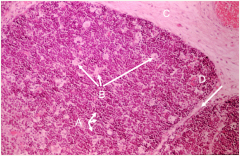
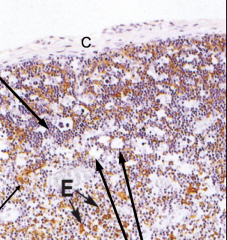
thymus cortex A: lymphocyte B: macrophages C: capsule D: septa |
|
|
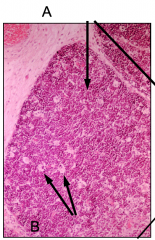
A: lymphocytes B: macrophage |
|
|
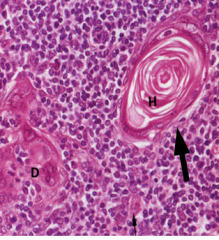
B Hassal's corpuscle |
|
|
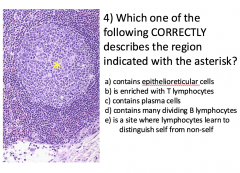
thymus E: Epithelioreticular |
|
|
Hassal's corpuscle |
|
|
Hassal's corpuscle |
|

|
Hassal's corpuscle |
|
|
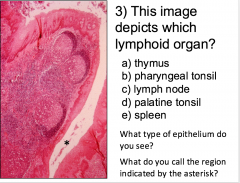
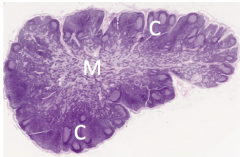
D SSNKE *= crypt |
|
|
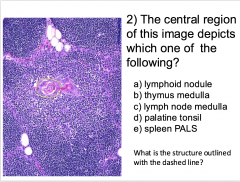
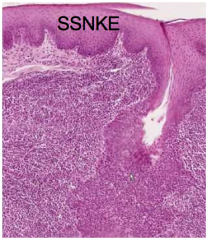
palatine tonsil |
SSNKE |
|
|
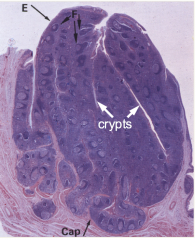
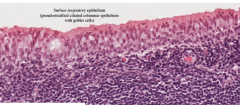
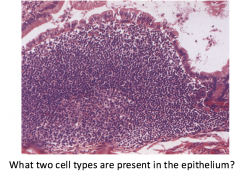
pharyngeal tonsil |
respiratory epithelium |
|
|
palatine tonsil |
|
|
palatine tonsil |
|
|
pharyngeal tonsil |
|
|
D |
|
|
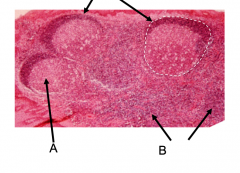
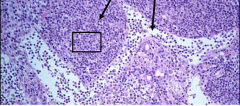
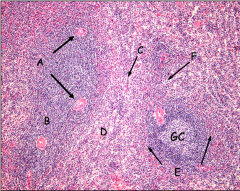
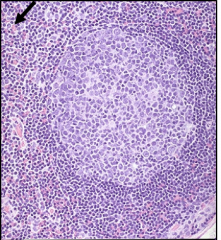
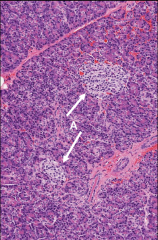
lymphoid nodules A: B cell proliferation, gerinal center B: diffuse, T-cell center |
|
|
D |
|
|
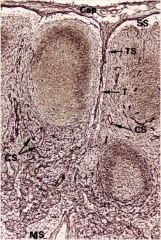
medullary sinuses and cords |
|
|
lymph node |
|
|
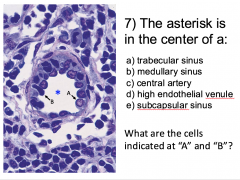
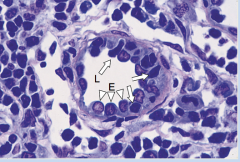
D A: endothelial B:lymphocyte |
|
|
HEV |
|
|
E |
|
|
C A: SM B: CT |
|
|
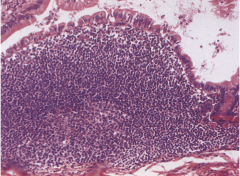
Peyer's patch |
|
|
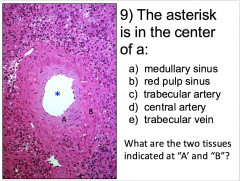
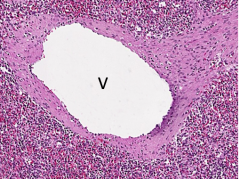
trabecular vein |
|
|
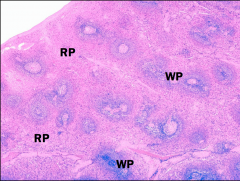
Spleen |
|
|
Spleen, red pulp cords and sinusses |
|
|
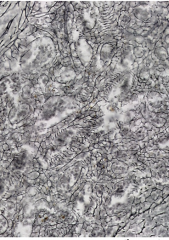
spleen red pulp cords (the reticular fibers around cords) |
|
|
PALS |
peripheral lymphatic sheath lymphocytes surround central artery in spleen |
|
|
marginal zone |
slow down the blood flow to increase interaction of foreign antigens and lymphocytes |
|
|
marginal zone (A) what is surround the white pulp |
|
|
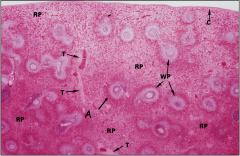
A: central arteries B: PALS C: red pulp cord D: red pulp E: marginal zone F: red pulp sinus |
|
|
Peyer's patch |
|
|
Peyer's Patch |
|
|
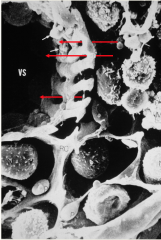
to show the discontinuous endothelial and the open circulation in spleen |
|
|
Tonsil reticular fiber showing with the medullary cord and sinus are |
|
arrow? |
lymph nodules arrow is pointing to macrophages diffuse (t cells) and germinal center (B cells) |
|
|
lymph nodules |
|
|
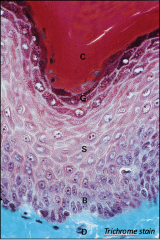
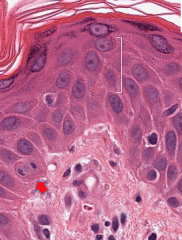
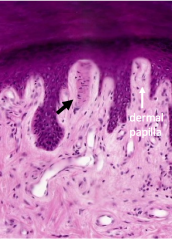
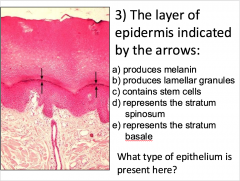
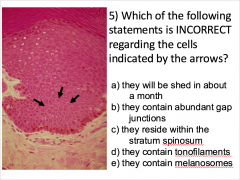
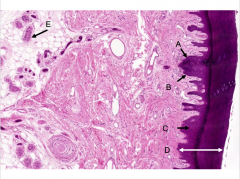
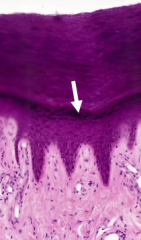
epidermis stratum basale (D) stratum spinosum (S) startum granulosum |
|
|
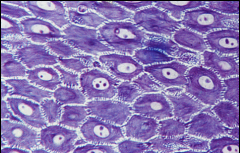
stratum spinosum |
|
|
(thin skin) stratum spinosum stratum granulosa (the top, nucleus with dark halo) stratum corneum (kertinized layers at the very top) |
|
|
stratum corneum |
|
|
stratum corneum |
|

|
melanin cap, sun is on the top |
|

|
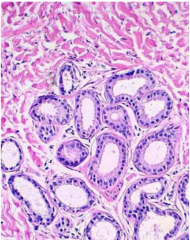
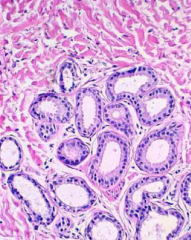
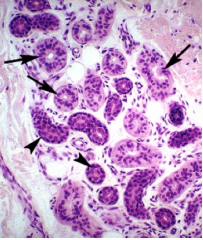
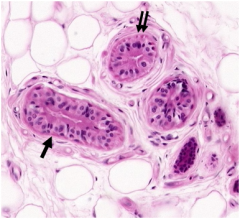
eccrine sweat gland |
|

|
eccrine sweat gland |
|
|
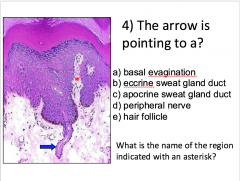
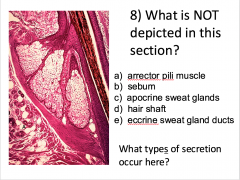
eccrine gland duct |
|

|
eccrine gland duct |
|
|
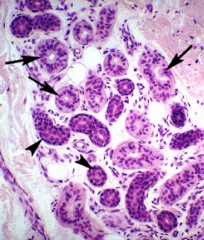
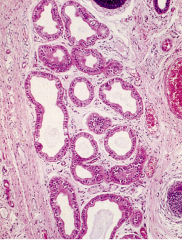
apocrine gland |
|
|
eccrine gland |
|
|
Meissner's corpuscle |
|
|
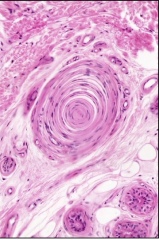
Pacinian corpuscle |
|
|
B |
|
|
B |
|
|
Stratum granulosum |
|
*? |
B *=papillary |
|
|
B |
|
|
D |
|
|
apocrine sweat gland |
|
|
C merocrine (A) and holocrine |
|
|
apocrine |
|
|
eccrine |
|
|
A |
|
|
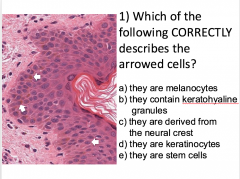
A: Merkel B: melanocyte C: Langerhan D: keratinocyte E:myoepithelial |
|
|
myoepithelial |
|
|
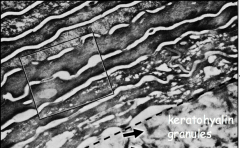
keratinohyaline granule |
|
|
D |
|
|
Thymus characteristics |
starry sky basophilic due to lymphocytes cortex and medulla clear area is the macrophages no nodules |
|
|
thymus medulla characteristics |
not as basophillic compare to cortex |
|
|
thymus stroma |
CT capsule and septa |
|
|
epitheilorecticular cells |
keratiform clusters in thymus, may be found in surround capillaries create blood thymus barrier |
|
|
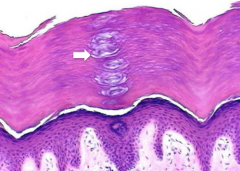
Hassall's corpuscle |
stimulating subset of T cells develop only thymic medulla eosinophillic |
|
|
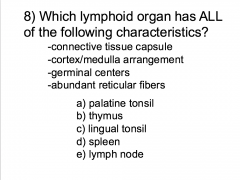
secondary lymphoid organ |
has nodules not capsulated: tonsil, peyer's patch, appendix MALT: lymph nodes, spleen |
|
|
Tonsil |
ex. lingual, palatine, pharyngeal multiple crypts, increase SA to expose all antigen |
|
|
pharyngeal tonsil |
back of the throat respiratory epithelium |
|
|
palatine tonsil |
near the nose SSNKE |
|
|
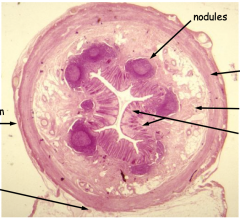
appendix |
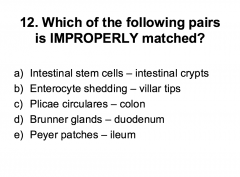
no villi, but has intestinal crypt has lymphocytes |
|
|
appendix function |
Immune surveillance (abundant m cells) Endocrine orgaearly ilife Reserve of gut flora: loss due to diarrhea, toxic etc Surgical substitute for diseased ureters, sphincter in reconstructive bladder surgeries Vestigial: former enlarged cecum |
|
|
lymph nodes |
filter lymph and expose antigen to immune cells concentrate in neck, axilla, groin |
|
|
paran cortex |
key lymphocytes |
|
|
lymph nodes medulla cords |
loose CT, highly cellular, produce Ab that gest into sinuses, plasma cells |
|
|
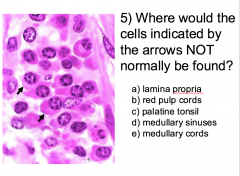
lymph nodes medullary sinus |
venous channel running between cords discontinuous endothelium traversed by reticular fibers would not find CT cells |
|
|
what cells are present in outer cortex of lymph nodes |
b cells |
|
|
what cells are present in the inner cortex of ;ymph nodes |
t cells |
|
|
what mech lymph nodes use to ensure lymphocyte and antigen mix |
sinuses are lined by a discontinuous endothelium reticular fibers transverse sinuses afferent lymphatics outnumber efferent (bottleneck effect) |
|
|
lymphocyte circulation @lymph node |
subcapsular --> trabecular --> medullary |
|
|
HEV |
high endothelial venule lymph node more cuboidal than other veins lymphocyte escape blood and go into various organ importance surveillance route |
|
|
paracortical reaction |
activation of HEV lead to enlargement of paracortex die to T cell inflex and proliferation |
|
|
cortical sinus |
subcaspsular and travecular |
|
|
lymphadenopathy |
disease of lymph nodes ex. HIV infection: virus bind to CD4 of T cellf |
|
|
unction of spleen |
Immune response, B & T cells Destroys damaged, senescent blood cells Sequesters monocytes Hematopoiesis (fetadevelopment) Storage of blood/platelets Recycling of iron |
|
|
lymph node cords/ sinus v. spleen cords/ sinuses |
spleen have blood celiboth cords and sinuses and sinuses are not traversed by reticular fiber |
|
|
white pulp v. red pulp |
masses of lymphocyte, few RBC red pulp has more RBC |
|
|
Red pulp cords |
Loose CT/ reticular fibers Cellular elements: RBC, platelets, macrophages, plasma, lymphocytes Go through the slits of stave cells to get to sinus |
|
|
Red pulp sinuses |
Sinusoid don’t have reticular fiber “stave cells” Venous channel lined by elongated discontinuous endothelial cells Spherical structure line with endothelial |
|
|
circulation in spleen |
Trabecular → central artery → branches that go to the red pulp → open circulation |
|
|
spleen trabecular artery |
efferent lymphatic, alst stop for filtration |
|
|
PAL |
lymphocytes surround central artery |
|
|
Marginal zone |
Reticular fiber slow the blood flow down so foreign antigen can interact with the lymphocyte, first part of open circulation, where antigen-immune cell interaction occur first in spleen |
|
|
Trabecular arteries v. veins ub spleen |
Arteries: endothelial cell and SM
Vein: fibroblast, collagen |
|
|
skin |
epidermix and dermis |
|
|
integument |
skin and hypodermis |
|
|
hypodermis |
subcutaneous (superficial fascia), adipocyte, contain specialized glands, hairs, sensory receptors (cutaneous adnexa) |
|
|
function of kin |
Protective: keratin synthesis, hairs, sebum Sensory: specialized nerve endings Thermoregulation: sweat glands, control of blood flow Metabolic: vitamin D synthesis, ion balance (Sweat) Immunological: longerhan’s cells, wandering lymphocytes Absorption: nicotine, steroid H, motion sickness |
|
|
Epidermis |
SSKE, keratinocytes, avascular |
|
|
thick skin |
located on palms/ soles, hairless, fingerprint grooves, SSKE |
|
|
thin skin |
located everywhere except palms/ soles, usually has hair/ hair associated glands, SSKE |
|
|
list of layers, deepest to most upper |
basale spinosum granulosum corneum lucidum |
|
|
stratum corneum |
hin skin Has lipid in intracellular space |
|
|
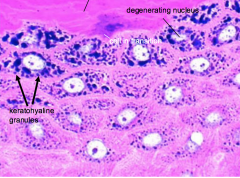
stratum granulosum |
granules are histidine rich negatively charged (appear dark) Abundant keratintonofibril Undergo special apoptosis: nucleus and organelles degenerate, but the cell membrane persist. Has granuleskeratohyaline granules and Lamellar granules: |
|
|
keratintonofibril |
skin keratin intermediate, tonofilament bound together filaggrin (fill the surface cell) |
|
|
granuleskeratohyaline granules |
not membrane bound filaggrin and loricrin |
|
|
filaggrin |
filament aggregating protein, anti friction and restrict water movement |
|
|
loricrin |
coat inside of the membrane, help to reinforce the PM |
|
|
lamellar granules |
exocytosis, fill with lipid, make the skin waterproof |
|
|
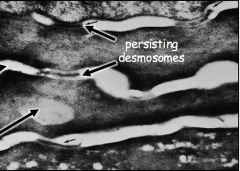
Stratum spinosum |
prickle cell layer Abundant desmosomes tonofilament |
|
|
stratum basale |
germinativum stem cells layer HPV infection of basal keratinocytes→ hyperproliferation, warts or carcinoma (basal cell or squamous cells)tonofilament |
|
|
stratum basale stem cell division |
At the top: slowly dividing cell, mitosis horizontal axis, both daughter cell in contact with BL'\ At the bottom: mitotic axis is not vertical, has melanocytes, Merkel cellsc |
|
|
cell types in skin |
melanocutes, keratinocytes, langerhan's cells, Merkel cells |
|
|
melanocyte |
clear, typically found right at the BL Neural crest derivative Synthesize tyrosinase (unique) at golgi |
|
|
Pigment donation |
keratinocytes take the melanin from melanocytes and incorporated it in their cytoplasm |
|
|
melanin |
emumelanin and phaeomelanin |
|
|
phaeomelanin |
Less effective at block UV rays, weaker antioxidant→ increase risk of melanoma/ skin cancer Can have vitamin D synthesis under low light |
|
|
Langerhan's cells |
Ag presentation no desmosome, few IF derived from bone marrow |
|
|
Merkel cells |
mechanoreceptors |
|
|
pigmentation in skin |
Dermal capillary bed Fat soluble pigments (carotene) Endogenous pigment (bilirubin, hemosiderin) Stratum corneum thickness eumelanin/pheomelanin pigments |
|
|
dermis |
CT, contains specialized glands, hairs, sensory receptor |
|
|
papillary |
upwelling that extend into epidermis |
|
|
function of papillary |
increase SA between epidermis and the underlying dermis A place for blood vessel for heat exchange with the outside word Bring sensory sensor as close to the outside world as possible |
|
|
hair |
keratinized epithelial structure |
|
|
glands |
eccrine, apocrine, sebaceous |
|
|
eccrine |
single simple, coiled tubular, only have on thick skin myoepithelial cells |
|
|
function of eccrine |
thermoregulation (sweat) salt balance ducts modify the secretion |
|
|
myoepithelial in eccrine |
forces sweat out reabsorb sodium in hypodermis and CT |
|
|
apocrine |
simple coiled tubular gland both apocrine/ eccrine secretion store product Ducts do not modify the secretionRestricted distribution Develop at puberty Pheromone production, activated by stress and sexual stimulation Go into hair follicle where CF is defected |
|
|
sebaceous gland |
Acinar Holocrine Secrete oily substance (sebum) Usually associated with hairs, may exist without (fordyce spots) Arrector pili muscle Go into hair follicle |
|
|
arrector pili muscle |
give you goosebumps |
|
|
sensory ending |
non capsulated: free nerve ending, merkel encapsulated: meissner's corpuscle, pacinian |
|
|
free nerve ending |
thermo, mechano, nociceptor, extend to stratum Gr. |
|
|
merkel nerve ending |
slow adapting mechano |
|
|
Meissner’s corpuscle |
rapid-adapting high desnity = discrimnartory (Braille) Dermal papilla (give nutrients to the skin) |
|
|
Pacinian corpuscles |
rapidly adapting mechano (vibration) hypodermis axon in the middle |
|
|
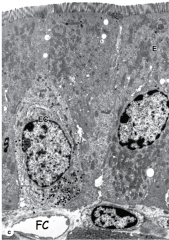
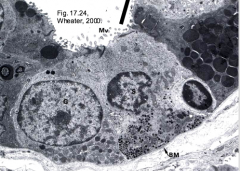
enteroendocrine cells |
|
|
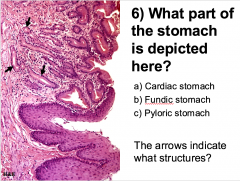
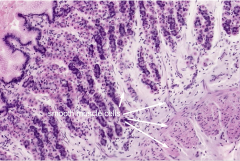
pyloric region stomach |
|
|
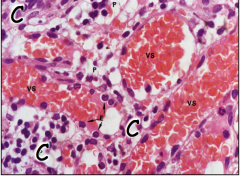
Fundic region stomach A: SM |
|
|
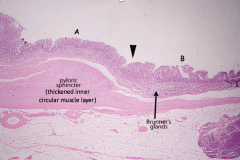
pyloric sphincter A: pyloric stomach B: duodenum |
|
arrow? |
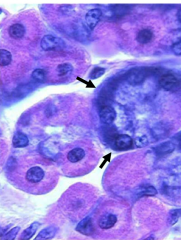
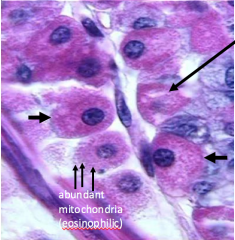
chief cells |
|
clear part? |
Parietal cells clear: IC |
|
|
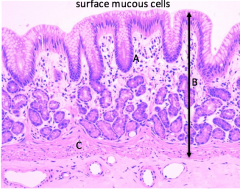
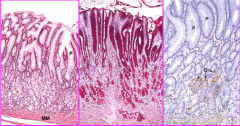
Fundic region stoamch parietal cells chief cells mucous neck cells |
|
|
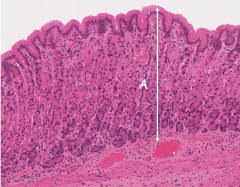
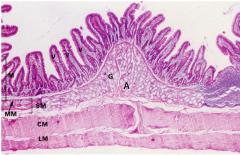
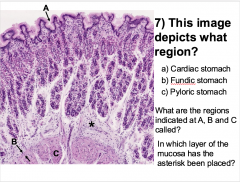
fundic region stomach A: mucosa |
|
|
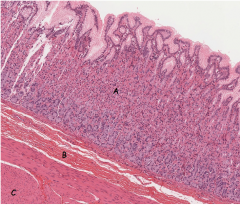
stomach, fundic region A: mucosa B: submucosa C: muscularis externa |
|
|
stomach, cardiac region A: lamina propria B: mucosa C: muscularis mucoase |
|
|
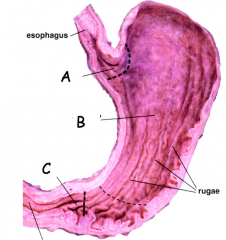
A: Cardiac B: fundus/ body C: pyloris |
|
|
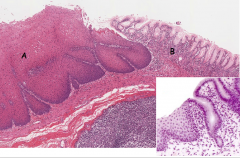
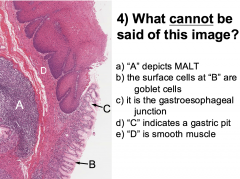
gastroesophageal junction A: esophagus B: cardiac stomach |
|
|
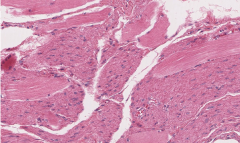
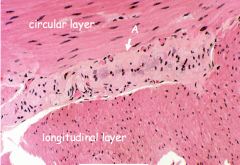
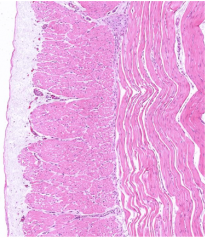
esophagus muscularis externa longitudinal section middle third |
|
|
esophagus muscularis externa lower third A: myenteric plexus (Auerbach's) |
|
|
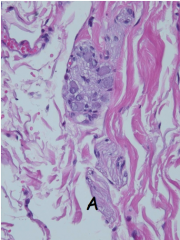
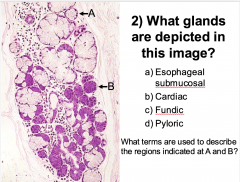
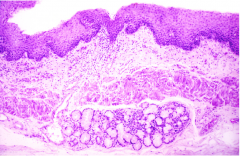
esophageal glands |
|
|
esophagus submucosal plexus (Meissner's) |
|

|
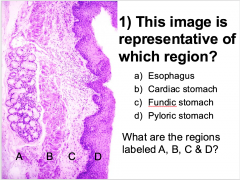
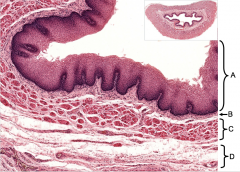
esophagus A: muscularis mucosae B: submucosa C: mucosa D: muscularis externa E: SSNKE F: adventitia/ serosa |
|
|
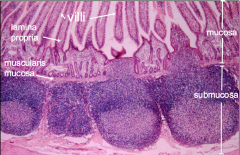
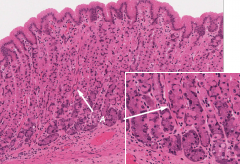
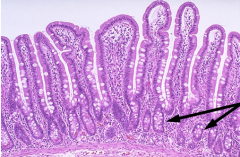
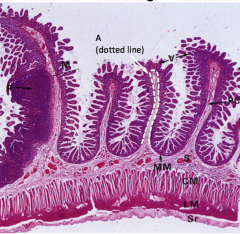
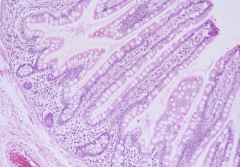
Small intestine duodenum |
|
|
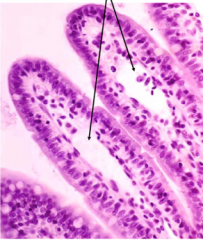
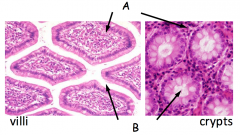
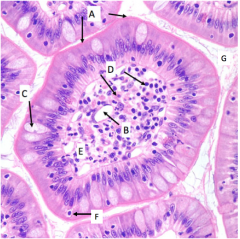
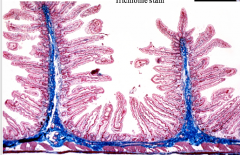
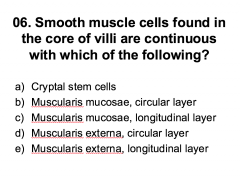
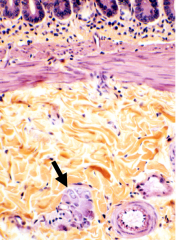
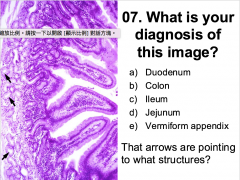
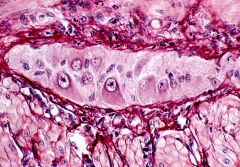
villi small intestine |
|
|
small intestine central lacteal |
|
|
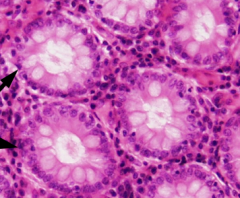
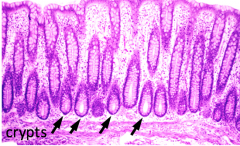
small intestine crypts |
|
|
duodenum arrow: crypts |
|
|
A: lamina propria B: intestinal lumen |
|
|
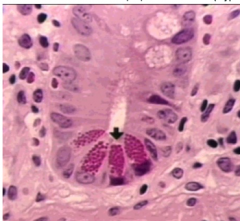
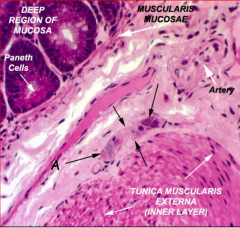
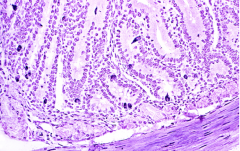
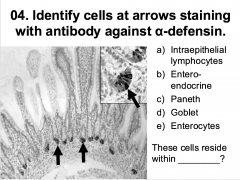
paneth cells |
|
|
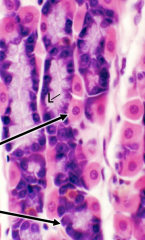
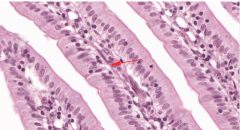
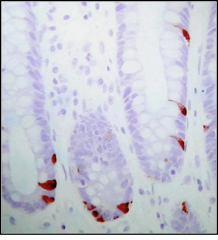
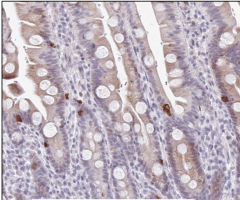
enteroendocrine cells |
|
|
enteroendocrine cells |
|

|
open type enteroendocrine cells |
|
|
close type enteroendocrine cells |
|
|
jejunum A: muscularis mucosa |
|
|
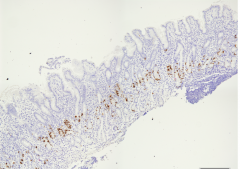
ileum Peyer's patch |
|
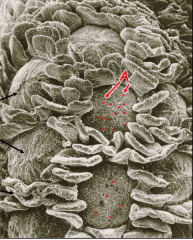
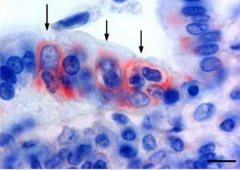
red dots? |
Peyer's patch red: M cells |
|
|
muscularis externa small intestine A: myenteric (Auerbach's) plexus |
|
|
Meissner's plexus small intestine |
|
|
Serosa small intestine |
|
|
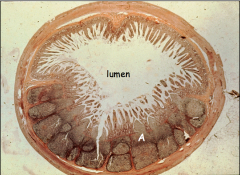
colon |
|

|
Teniae coli |
|
|
appendix |
|
|
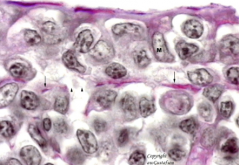
A = microvilli/glycocalyx B = central lacteal C = goblet cell D = immune cells (plasma, lymphocyte) E = lamina propria F = wandering lymphocyte G = gut lumen |
|
|
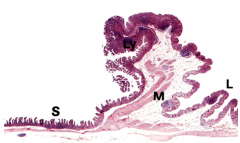
A ------- D:SSNKE C:lamina propria B:muscularisexterna A:submucosa (seromucous glands) |
|
|
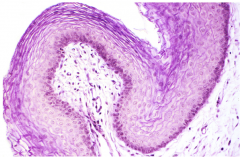
esophagus epithelial and lamina propria |
|
|
Esophagus A: epithelium B: lamina propria C: m. mucosae D: submucosa |
|
|
A ------- A: serous B: mucous |
|
|
esophagus |
|
|
C |
|
arrow? |
esophagus, middle 1/3 arrow is myenteric plexus |
|
|
esophagus, middle 1/3 |
|
|
C |
|
|
B |
|
|
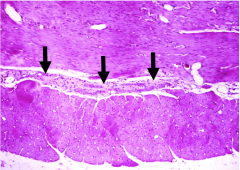
A (squamocolumnar junction) |
|
|
B A: pit B:inner muscular mucosae C: external muscular mucosae *: lamina propria |
|
|
stomach, fundus gastric gland proper |
|
|
B A is mitochondria |
|
|
enteroendocrine cells |
|
|
stomach, fundic region |
|
|
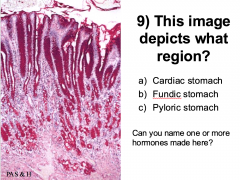
C hormone: ghrelin, gastric |
|
|
A |
|
|
stomach, pyloric |
|
|
gastroduodenal junction |
|
|
B in lamina propria |
|
|
D |
|
|
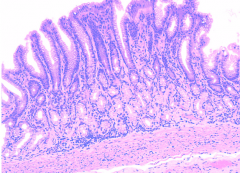
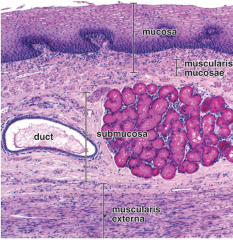
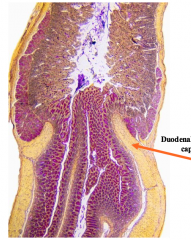
What is diagnostic of duodenum? |
Bruner's glands |
|
|
C |
|
|
How does small intestine increase curface area |
Organ (coiled) Plicae Villi Microvilli Glycocalyx |
|
|
plicae of small intestine |
|
|
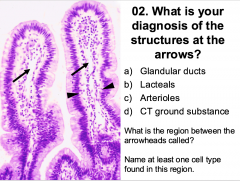
B Between the arrow: Laminapropria cell types: Macrophage,fibroblast, lymphocyte/ plasmacell, SM cells |
|
|
D |
|
|
enteroendocrine, small intestine |
|
|
C reside in crypt |
|
|
Paneth cells |
|
|
E |
|
|
B |
|
|
small intestine mucosa and submucosa arrow = enteric ganglion of submucosal neural arteriole and veinule |
|
|
A arrow is the Bruner's gland (submucosa) |
|
|
MyentericNeural Plexus (Auerbach) |
|
|
C |
|
|
ileum |
|
|
C |
|
|
M cells |
|
|
M cells |
|
|
ileocecal junction |
|
|
B Teniae coli |
|
|
D |
|
|
C |
|
|
Esophagus function |
transfer food, gluid form pharynx to stomach protection: SSE, secretion (EGF, bicarbonate, mucins, antimicrobials) |
|
|
esophagus mucosal lining |
SSNKE (langerhans cells. merkel cells, and rarely melanocyte) lamina propria: ridges, no glands musclaris mucosae: longitidunally |
|
|
esophagus submucosal |
loose CT, Meisner glands (mixed seromucous) ducts: stratified cuboidal epithelium |
|
|
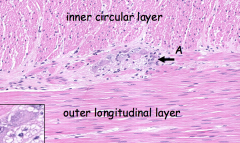
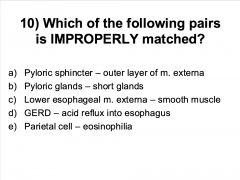
esophagus musclaris external |
inner is circular/ outer longitidunal myenteric (Auerbach's) upper 1/3=skeletal muscle middle 1/3 = skeletal/ smooth mixed lower 1/3= smooth muscle |
|
|
suqamocolumnar junction |
zigzag line end of esophagus and stomach simple columnar at the beginning of stomach |
|
|
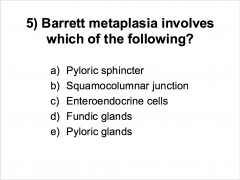
Barret esophagus |
protect lower esophagus by metaplastic change to simple columnar, become unstable, precursor to cancer |
|
|
stomach function |
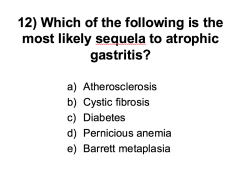
mechanical churning acid production protein hydrolysis, bacteriostatic mucous production releases intrinsic factor: absorb vitamin B12 releases hormones |
|
|
stomach secretory organ |
exocrine eneteroendocrine |
|
|
What do stomach exocrine glands secrete |
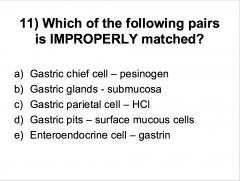
HCl, intrinsic factor, pepsinogen/ pepsin, gastric lipase, lysozyme |
|
|
what do stomach enteroendocrine secrete |
H (gastrin/ paracrin; ghrelin/ endocrine. somatostatin) |
|
|
stomach mucosa |
simple columnar (extend into ducts, gastric pits) lamina propria: mucosal glands, surrounded by loose CT M. mucosae: inner circular, outer longitudinal |
|
|
stomach submucosa |
dense CT, no glands |
|
|
stomach muscularis externa |
discontinuous outer: longitudinal muscle middle: circular inner: oblique, not well developed in central region |
|
|
rugae |
allow stomach to expand when eating |
|
|
gastric canal |
form esophagus directly to intestine (ex. water) bypass stomach |
|
|
sections of stomach |
cardiac fundus pyloris |
|
|
stomach cardiac region |
short short glands extend into lamina propria |
|
|
stomach cardiac region glands |
mucous enteroendocrine |
|
|
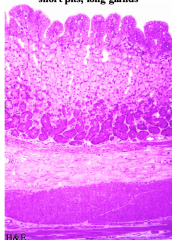
stomach fundus region |
short long (branched) thick mucosa lining glands stretched down to muscular mucosa |
|
|
Cell types in stomach fundus region |
parietal cell cheif cells SM mucous neck cell |
|
|
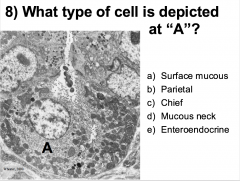
parietal cells |
aka oxyntic cell intracellular canaliculus mitochondria --> eosinophilic release intrinsic factor for vitamin B12 absorption in gut |
|
|
intracellular canaliculus |
when inactive state (between meals): tubulovesicular system wActive: after eating, fuse to the membrane and form deeper IC with huge SA for proton pump to decrease the pH in the lumen, so clear area inidicate active |
|
|
what does IC look on stain |
clear |
|
|
stomach pyloris region |
lon short spincter: open when digestion is completely done |
|
|
stomach pyloric glands |
mucous, enteroendocrine |
|
|
diagnostic feature of small intestines |
villi goblet cells mucosal glands (paneth cells) submucosal glands @ duodenum |
|
|
organization of small intestine epithelium layer |
coiled organ plicae villi microvilli and glycocalyx |
|
|
plicae |
permanent, don't stretch out core: collagen of submucosa |
|
|
small intestine villi core |
SM cells that are continuous with muscularis mucosae circular layer |
|
|
enzyme activity in microvilli/ glycocalyx in small intestine |
local activation of trypsinogen to trypsin by enterokinase/ enteropeptidase |
|
|
Crypts of small intestine (cell types and characteristics) |
extend into lamina propria goblet paneth enteroendocrine stem cells diffuse neuroendocrine cells |
|
|
paneth cells |
antimicrobial cells (innate immunity) located at the base of the crypt Pyramidal shaped contain large eospinphilic granules secrete lysozyme, alpha defensinshelp keep small intestine aseptic |
|
|
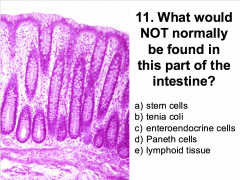
why is there no paneth cells in large intestines |
Not normally found in large intestine because large intestine is septic |
|
|
enteroendocrine cells in small intestine crypt |
secrete basally into ECM, fenestrated capillaries Open and closed |
|
|
open enteroendocrine |
regulate luminal contents Has a surface that is exposed to lumen |
|
|
closed enteroendocrine |
regulate neural and paracrine mechanism, lot of pores for product to get in |
|
|
turn over rate of small intestine stem cells |
4-6 days |
|
|
muscularis mucosae of small intestine |
longitudinal SM muscles move villi and mix lumen content lymphatic |
|
|
muscularis externa of small intestine |
inner circular and outer longitudinal layers Myenteric (Aurebach’s) plexus Meissner’s capsule Submucasal plexus |
|
|
components of small intestestine |
duodenum jejunum ileum |
|
|
duodenum |
where liver and gallbladder empty to Brunner's gland goblet |
|
|
Brunner's gland |
secrete alkaline mucus to neutralize chyme |
|
|
jejunum |
plicae no glands |
|
|
ileum |
peyer's patch enterocytes m cells can have plicae, but not a lot |
|
|
diagnostic of large intestine |
No villi Many goblet cells Crypts Teniae coli Mucosal glands: long, no paneth cells normally |
|
|
colonocytes characteristic |
larger intracellular region, smaller microvilli |
|
|
components of large intestine |
cecum vermiform appendix colon |
|
|
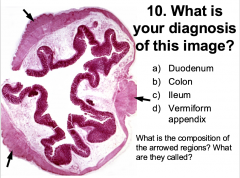
vermiform appendix |
enterocytes, goblet cells, M cells narrow lumen Lymphoid nodules: often extending from lamina propria to submucosa, perforating the muscularis mucosae No villi Crypts deep into mucosaMuscular mucosa similar to small intestines |
|
|
colon |
smooth surface no villi teniae coli serosa and adventitia cover |
|
|
sections of colon |
ascending, transverse, descending, sigmoid |
|
|
teniae coli |
SM, slow down peristalsis |
|
|
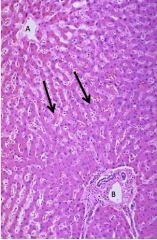
A liver |
|
|
liver |
|
|
liver |
|

|
liver (pig) |
|
|
B |
|
|
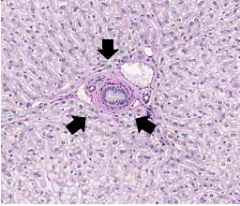
portal area blue: collagen |
|
|
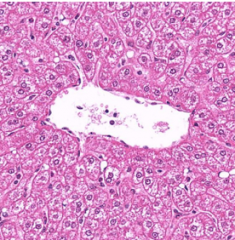
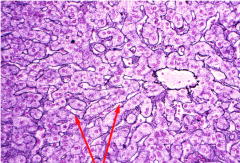
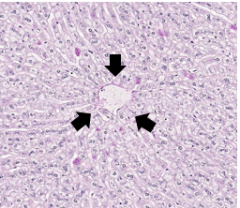
liver central vein |
|
|
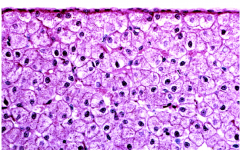
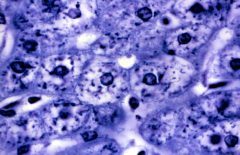
hepatocyte |
|
|
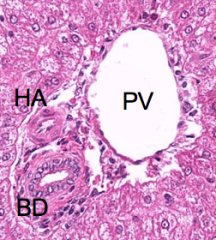
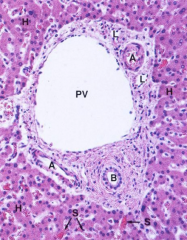
portal area liver |
|
|
liver, intralobular CT red arrow: reticular fiber |
|
|
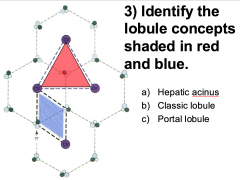
red: C blue: A |
|
|
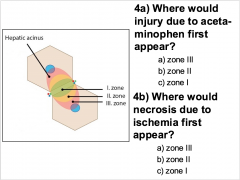
4a.) A 4b.) A |
|

|
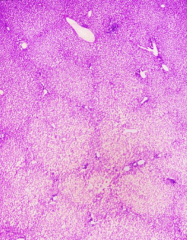
liver acinus zone III would have the most pathologic change |
|
|
hepatocyte |
|
|
C |
|
|
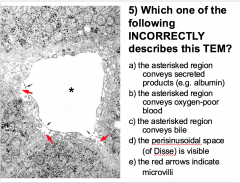
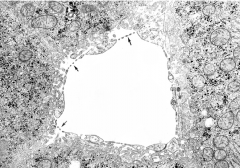
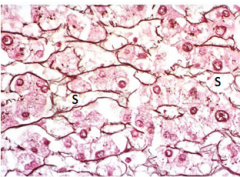
sinusoidal domain |
|
|
sinusoidal capillaries B |
|
|
B |
|
|
8a.) A 8b) C |
|
|
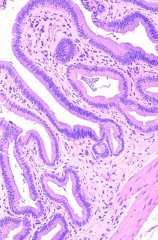
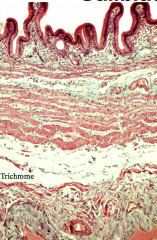
gallbladder |
|
|
gallbladder |
|
|
B |
|

|
gallbladder mucosa bile concentration |
|
|
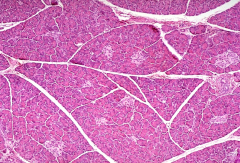
pancreas |
|
|
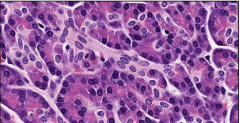
pancreas serous acinus |
|
|
D |
|
|
C |
|
|
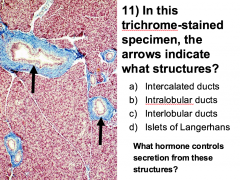
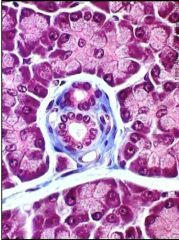
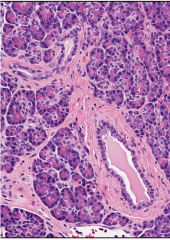
pancreas L: interlobular duct R: intralobular ducts |
|
|
C (mutation affect duct cells) |
|
|
where is CFTR located |
duct cells in pancreas |
|
|
liver function |
Metabolic (Uptake, storage, metabolism & distribution of important nutrients and vitamins; Degradation & conjugation of metabolites and potential toxic substances Iron recycling) Exocrine: Production & secretion of bile Endocrine: Synthesis & secretion into the blood of most plasma proteins |
|
|
Where are the CT in liver |
not a lot to begin with mostly around ducts and CT capsule |
|
|
liver stroma |
fibrous capsule interlobular CT intralobular CT |
|
|
liver fibrous capsule |
hold liver together Serosa: mesothelium, delicate CT (visceral peritoneum) Adventitia: hilum, attachment of gallbladder |
|
|
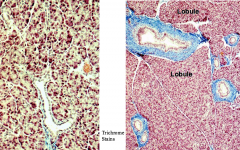
liver interlobular CT |
portal areas perilobular CT septa in some mammals |
|
|
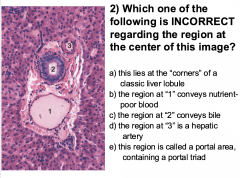
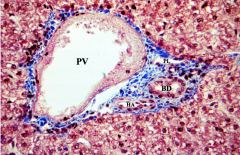
Portal areas |
portal triad portal vein, hepatic artery, bile duct |
|
|
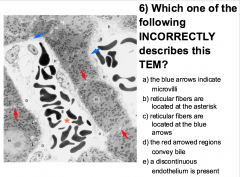
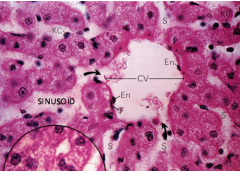
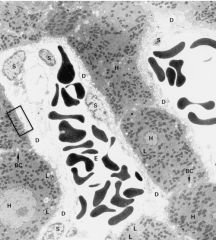
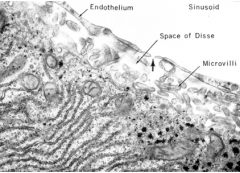
liver sinusoid |
discontinuous/fenestrated endothelium overlie perisinusoidal space (Disse) contain reticular fibers (slow blood flow) Leakiest of all capillaries |
|
|
Disse |
between endothelial and hepatocyte |
|
|
direction of blood flow in liver sinusoid capillaries |
peripheral to central |
|
|
liver cell types |
hepatocyte, Kupffer cells, fibroblast, stellate cells, stem cells |
|
|
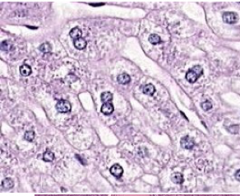
hepatocyte |
polygonal, often binucleate filled with RER and SM sinusoidal (basal): microvilli, Disse |
|
|
kupffer cells |
macrophage/ monocyte |
|
|
bile canaliculi |
secrete bile made by hepatocyte into bile duct toward portal tract sealed by occluding junction |
|
|
Ito cells |
stellate store vitamin A activated upon damage, replace with scarred tissue |
|
|
liver stem cells |
BM derived |
|
|
liver lobules |
classic, portal, liver acinus |
|
|
liver classic lobules |
endocrine, metabolic centered around central veins portal triad at the corner |
|
|
liver portal lobule |
exocrine, excretory centered around bile duct intralobular duct |
|
|
liver acinus |
microcirculatory unit, pathologic change, rapport lobule diamond shape, centered around incoming blood |
|
|
pancreas structure |
stroma and prenchyma |
|
|
parenchyma |
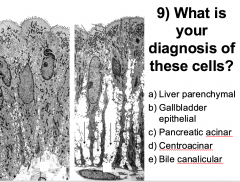
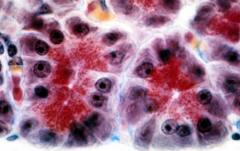
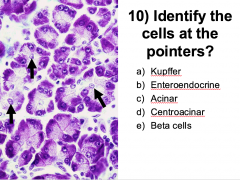
pancreas exocrine (acinar zymogenic cells) basal bsaophilia apical zymogen (secretion) centroacinar cells |
|
|
centroacinar cells |
lone, surround by white cytoplasm, no basophilia |
|
|
function of pancreas |
production and secretion of digestive enzymes (acinar cells) secretion of alkaline fluid (duct cells) |
|
|
pancreas ducts |
intralobular/ interlobular major/ accessory duodenal papillae |
|
|
pancreas exocrine |
basal basophilia (RER) euchromatic and prominent nucleus supranuclear golgi apparatus apical secretory granules (zymogen) serous |
|
|
what H control pancreatic acini |
CCK |
|
|
what H control pancreatic duct |
decretin |
|
|
pancreatic interlobular ducts |
large duct between lobules embedded within collagen to form septa simple cuboidal |
|
|
pancreatic intralobular duct |
smaller ducts in lobules eosinophilic cytoplsm elongated nuclei |
|
|
pancreatic endocrine |
islets of langerhans fenestrated capillaries produce and secretes insulin, glucagon, somatostatin |
|
|
gall bladder anatomic region |
fundus (closed end) body neck |
|
|
gall bladder mucosa |
simple columnar epithelium (no goblet cells) lamina propria no muscularis mucosa, submucosa, or mucosal glands |
|
|
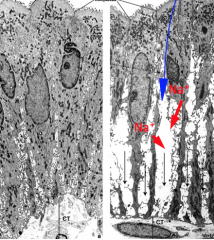
how gall bladder concentrate the bile |
when inactive, cells are closed off. when active, pump Na into basolateral spaces and generate osmotic gradient. As a result, water from solution in gallbladder when enter the basolater spaces |
|
|
diagnostic feature of gall bladder |
simple columnar epithelium (no goblet cells) false glands Rokitansky-Aschoff sinuses |
|
|
function of gall bladder |
storage and concetration of bile |
|
|
hepatopancreatic ampulla |
within major duodenal papilla, openning of common bile and pancreatic duct |
|
|
Rokitansky-Ashoff sinuses |
penetrate down to muscularis externa sacks of epithelium with fluid associated with development of gallstone |
|
|
what does CCK and secretin stimulate for gall bladder |
CCK: simulate muscularis contraction secretin: bicarbonate secretion from bile duct cells |
|
|
Gastro-esphageal reflux disease (GERD) |
Loosening of the squamocolumnar junction, that could change SS to simple columnarInflammation of esophagus, esophageal strictures, Barrett’s esophagus |
|
|
pernicious anemia |
Vitamin B12 deficiency can lead to decreased rbc development |
|
|
Helicobacter pylori infection |
Has urease on surface that convert urea to ammoniaNeutralize acid that surround bacter, dissolve mucous to allow penetrationSurface have Ag that mimic endogenous proteins in stomach. So when body makes the Ab, it becomes autoimmune and also damage stomach lining |
|
|
Celiac disease |
inflammatory response to gluten protein; glycocalyx & microvilli structure is disrupted (atrophy) leading to malabsorption |
|
|
chlelithiasis |
Formation and presence of concretions (calculi; stones) in gallbladder or bile ducts |
|
|
what is the major component of gallstone |
choelsterol |
|

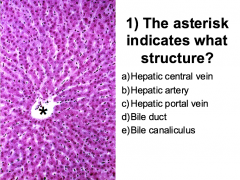
A? *? |
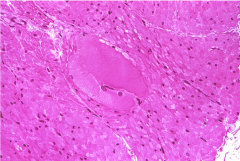
A: Central vein *: portal triad |
|
|
liver |
|
|
liver sinusoid |
|
|
liver |
|
|
liver |
|
|
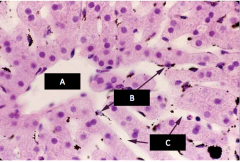
A: CV B: kupffer cell C: sinusoid |
|
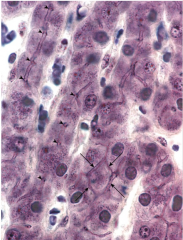
arrow? |
liver arrow: bile canaliculi |
|
what does arrow show? |
A: CV B: PV arrow show bile secretion (toward portal tract) |
|
|
liver portal area |
|
|
liver portal lobule |
|
|
liver classic lobule |
|

|
gall bladder A: Rokitansky-Aschoff sinuses |
|
|
inactive and active gall bladder epithelium |
|

|
gall bladder epithelium |
|
|
pancreas |
|
|
pancreas A: islets of langerhans |
|
|
pancreas interlobular ducts |
|
|
pancreas interlobular duct |
|
|
intralobular duct |
|
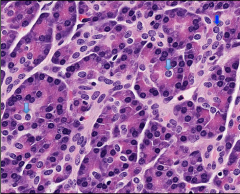
blue arrow |
centroacinar cell |