Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
184 Cards in this Set
- Front
- Back
|
Signs & tx of a right ventricular infarct |
Signs: hypotension, tachycardia, clear lungs, elevated JVP, and NO pulsus paradoxus
Tx: fluid resuscitation, don't give nitro! |
|
|
Tx for CHF exacerbation
|
LMNOP: lasix, morphine, nitro, O2, position (elevate head) or positive pressure ventilation
|
|
|
Tx for stable CHF that has mortality benefit
|
ACEi, Beta-blockers, spironolactone
|
|
|
Tx for ACS (UA, NSTEMI, STEMI)
|
BEMOAN: beta-blockers, enoxaparin, morphine, O2, ASA, nitro
|
|
|
Long-term tx post-MI
|
"ASA-Beta-Stati-Pril": ASA, Beta-blocker, Statin, ACEi
|
|
|
Most common cause of death post-MI
|
Arrhythmias (VFib)
|
|
|
Post-MI complication: New systolic murmur 5-7 days after
|
Mitral regurgitation due to papillary muscle rupture
|
|
|
Post-MI complication: Cause of acute severe hypotension
|
Cardiac tamponade due to ventricular free wall rupture
|
|
|
Post-MI complication: "step-up" in O2 concentration from RA to RV
|
Ventricular septal rupture leading to left-to-right shunt
|
|
|
Post-MI complication: persistent ST elevation ~1mo later + systolic murmur
|
Ventricular wall aneurysm
|
|
|
Post-MI complication: Cannon A-waves
|
AV dissociation either due to VFib or 3rd degree heart block
|
|
|
Post-MI complication: pleuritic chest pain and fever 5-10 wks later
|
Dressler's syndrome (likely autoimmune pericarditis). Tx with NSAIDs and ASA.
|
|
|
Diagnose: chest pain worse with inspiration, better with leaning forward, friction rub, and diffuse ST elevation
|
Pericarditis
|
|
|
Diagnose: chest pain worse with palpation
|
Costochondritis
|
|
|
Diagnose: chest pain with vague hx of recent viral infection and murmur
|
Myocarditis
|
|
|
Diagnose: chest pain that occurs at rest, worse at night, few CAD risk factors, with migraine H/As, transient ST elevation during episodes
|
Prinzmetal's angina (tx with CCB or nitrates)
|
|
|
EKG rhythm: progressive prolongation of PR interval followed by a dropped beat
|
2nd degree AV block - Type I
|
|
|
EKG rhythm: Cannon-a waves on physical exam and regular P-P interval and regular R-R interval
|
3rd degree AV block
|
|
|
EKG rhythm: varrying PR interval with 3 or more morphologically distinct P waves in the same lead; seen in older person with chronic lung dx (COPD) in pending resp failure
|
MAT: multifocal atrial tachycardia
|
|
|
EKG rhythm: short PR interval followed by QRS>120 ms with a slurred initial deflection representing early ventricular activation via the bundle of Kent
|
WPW: Wolff-Parkinson-White syndrome
|
|
|
EKG rhythm: regular rhythm with a ventricular rate of 125-150 bpm and atrial rate of 250-300 bpm
|
Atrial flutter
|
|
|
EKG rhythm: prolonged QT interval leading to undulating rotation of the QRS complex around the EKG baseline in a pt with low Mg, low K, lithium overdose, or TCA overdose
|
Torsades de pointes
|
|
|
EKG rhythm: renal failure pt OR crush injury OR burn victim with peaked T-waves, widened QRS, short QT and prolonged PR
|
Hyperkalemia
|
|
|
EKG rhythm: undulating baseline, no P waves, irregular RR interval in a pt with hyperthyroidism OR old pt with SOB/dizziness/palpitations with CHF or valve disease
|
AFib
|
|
|
Murmur: systolic ejection murmur, crescendo-decrescendo, louder with squatting, softer with valsalva, +parvus et tardus
|
Aortic stenosis
|
|
|
Murmur: systolic ejection murmur louder with valsalva, softer with squatting or handgrip
|
Hypertrophic cardiomyopathy
|
|
|
Murmur: late systolic murmur with click, louder with valsalva and handgrip, softer with squatting
|
Mitral valve prolapse
|
|
|
Murmur: Holosystolic murmur radiates to axilla with left atrial enlargement
|
Mitral regurgitation
|
|
|
Murmur: Holosystolic murmur with late diastolic rumble in kids
|
VSD
|
|
|
Murmur: Continuous machine-like murmur
|
PDA
|
|
|
Murmur: wide fixed and split S2
|
ASD
|
|
|
Murmur: rumbling diastolic murmur with an opening snap, left atrial enlargement, and AFib
|
Mitral stenosis
|
|
|
Murmur: blowing diastolic murmur with widened pulse pressure
|
Aortic regurgitation
|
|

Diagnose CXR: hyperlucent lung fields with flattened diaphragms
|
COPD
|
|

Diagnose CXR: opacification, consolidation, air bronchograms
|
Pneumonia
|
|

Diagnose CXR: heart>50% AP diameter, cephalization, Kerly B lines, interstitial edema
|
CHF
|
|

Diagnose CXR: cavity containing air-fluid level
|
Abscess
|
|

Diagnose CXR: Upper lobe cavitation, consolidation, +/- hilar lymphadenopathy
|
TB
|
|
|
Common causes of transudative pleural effusion
|
CHF, nephrotic, cirrhotic
|
|
|
Diagnose: transudative pleural effusion low in pleural glucose
|
Rheumatoid arthritis
|
|
|
Diagnose: transudative pleural effusion high in lymphocytes
|
TB
|
|
|
Common causes of exudative pleural effusion
|
Cancer or parapneumonic (pleural effusion secondary to pneumonia)
|
|
|
Light's criteria
|
Exudative pleural effusion if:
1. LDH > 2/3 of upper limit of normal 2. LDF effusion/serum >0.6 3. Protein effusion/serum >0.5 |
|
|
Sx of a PE
|
Sx: pleuritic chest pain, hemoptysis, tachypnea, tachycardia
|
|
|
Signs of a PE
|
right heart strain on EKG, sinus tachycardia, decreased vascular markings on CXR, wedge infarct, ABG with low CO2 and O2
|
|
|
Causes and tx of ARDS
|
Sepsis, gastric aspiration, trauma, low perfusion, pancreatitis
Tx: mechanical ventilation with PEEP |
|
|
Tx for COPD that has mortality benefit
|
Quitting smoking and continuous O2 therapy >18 hrs per day
|
|
|
Important vaccinations for COPD pts
|
Pneumococcus with a 5yr booster and yearly influenza vaccine
|
|
|
Diagnose: 1 cm nodules in upper lung lobes with eggshell calcifications
|
Silicosis
|
|
|
Diagnose: Hilar lymphadenopathy, increase ACE, erythema nodosum
|
Sarcoidosis = syndrome involving abnormal collections of chronic inflammatory cells (granulomas) that can form as nodules in multiple organs
|
|
|
Diagnose: pt with kidney stones, constipation, low PTH, and CENTRAL lung mass
|
Squamous cell carcinoma of the lung (paraneoplastic syndrome secondary to secretion of PTH-rP = low PO4 and high Ca)
|
|
|
Diagnose: pt with shoulder pain, ptosis, constricted pupil, facial edema, wt loss, cough + hemoptysis
|
Superior Sulcus Syndrome from Small Cell Carcinoma (also a central lung cancer)
|
|
|
Diagnose: pt with ptosis that improves after 1 min of upward gaze
|
Lambert Eaton Syndrome (autoimmune Ab production against pre-synpatic Ca channels)
-Around 60% of those with LES have underlying malignancy, most commonly Small Cell lung cancer; it is therefore regarded as a paraneoplastic syndrome |
|
|
Diagnose: old smoker presenting with hemoptysis, wt loss, Na=125, moist mucus membranes, and normal JVP
|
SIADH from small cell lung cancer (produces euvolemic hyponatremia)
Tx: fluid restrict (if Na>112, add 3% saline) |
|
|
Diagnose: pt with hemoptysis and wt loss, with CXR showing PERIPHERAL cavitation and CT showing distant mets
|
Large Cell Carcinoma of lung
|
|
|
IBD that increases risk for Primary Sclerosing Cholangitis
|
Ulcerative colitis (PSC leads to higher risk of cholangiocarcinoma)
|
|
|
IBD in which fistulas, granulomas, and transmural inflammation are likely
|
Crohn's
|
|
|
Tx of IBD
|
Corticosteroids to induce remission, ASA and sulfasalazine to maintain remission. For Crohn's, give metronidazole for any ulcer or abscess. If severe disease, give azathioprine, 6MP, and methotrexate.
|
|
|
Diagnose: AST>ALT (2x) + high GGT
|
Alcoholic hepatitis
|
|
|
Diagnose: ALT>AST and in the 1000s
|
Viral hepatitis
|
|
|
Diagnose: AST and ALT in the 1000s after surgery or hemorrhage
|
Ischemic hepatitis (shock liver)
|
|
|
DDx of elevated direct bili
|
Obstructive liver dx (stone, cancer), Dubin-Johnson syndrome, Rotor syndrome
|
|
|
DDx of elevated indirect bili
|
Hemolysis, Gilbert's syndrome, Criglr-Najjar syndrome
|
|
|
Diagnose: elevated ALP and GGT
|
Bile duct obstruction. If pt has IBD, consider PSC
|
|
|
Diagnose: elevated ALP, normal GGT, normal Ca
|
Paget's disease of the bone (excessive breakdown and formation of bone causing bone pain, back pain, increase hat size, hearing loss, headache).
Tx with bisphosphonates. |
|
|
Diagnose: liver disease pt with elevated antimitochondrial Abs
|
Primary Biliary Cirrhosis
|
|
|
Diagnose: liver disease pt with elevated ANA + antismooth muscle Abs
|
Autoimmune hepatitis
|
|
|
Diagnose: pt with low ceruloplasmin and high urinary Cu
|
Wilson's disease (hepatitis, psych sx due to Cu deposition in the basal ganglia, corneal deposits=Kayser-Fleischer rings)
|
|
|
Diagnose: liver disease pt with high Fe, low ferritin, low Fe binding capacity
|
Hemachromatosis (hepatitis, DM, golden skin)
|
|
|
Most common bugs causing meningitis
|
Strep pneumo
H. influenza N. meningitidis |
|
|
Tx for meningitis
|
Ceftriaxone, Vancomycin, Ampicillin (for Lysteria), and Dexamethasone
|
|
|
Pneumonia: most common bug?
|
Strep pneumo
|
|
|
Pneumonia: most common bug in healthy young people?
|
Mycoplasma
|
|
|
Pneumonia: most common bug in hospitalized pts?
|
Pseudomonas, Klebsiella, E. coli, MRSA
|
|
|
Pneumonia: most common bug in old smokers with COPD?
|
H. influenza
|
|
|
Pneumonia: most common bug in alcoholics with currant jelly sputum?
|
Klebsiella
|
|
|
Pneumonia: most common bug in old men with headache, confusion, diarrhea, and abdo pain?
|
Leigionella
|
|
|
Pneumonia: most common bug in pt who just delivered a baby cow and has vomiting and diarrhea
|
Coxiella burnetti
|
|
|
Pneumonia: most common bug in pt who just skinned a rabbit?
|
Franciella tularensis
|
|
|
Pneumonia: most common bug in pt who just had the flu?
|
MRSA
|
|
|
Positive TB test interpretation
|
Induration >15 mm is positive TB test in general pop
Induration >10 mm is positive if prisoner, healthcare worker, nursing home, DM, EtOH, chronically ill Induration >5 mm if AIDS or immunosuppressed |
|
|
Tx regimen for TB
|
RIPE: rifampin, INH (isoniazid), pyrazinamide, ethambutol
|
|
|
TB tx: s/e of Rifampin
|
body fluids turn orange/red, induces CYP450
|
|
|
TB tx: s/e of INH
|
peripheral neuropathy and sideroblastic anemia (prevent by giving vit B6), hepatitis with mild bump in LFTs
|
|
|
TB tx: s/e of Pyrazinamide
|
benign hyperuricemia
|
|
|
TB tx: s/e of ethambutol
|
optic neuritis, other color vision abnormalities
|
|
|
Acute endocarditis: most common bug?
|
Staph aureus
|
|
|
Subacute native valve endocarditis: most common valve affected and most common bug responsible?
|
mitral valve and Viridens group strep
|
|
|
IV drug use endocarditis: most common valve affected and most common bug?
|
tricuspid valve and Staph aureus
|
|
|
Endocarditis complications
|
CHF is #1 cause of death, septic emboli to lungs or brain
|
|
|
What is the next step if you find endocarditis caused by Strep bovis bacteremia?
|
Colonoscopy to look for colon cancer!
|
|
|
Criteria for diagnosing endocarditis?
|
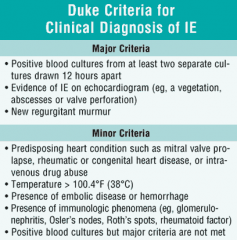
Modified Duke Criteria:
A definite diagnosis of IE can be established if the following conditions are fulfilled: 2 major criteria, 1 major + 3 minor criteria, or 5 minor criteria. |
|
|
When to suspect HIV...
|
1. young pt with new/bilateral Bell's palsy
2. young pt with unexplained thrombocytopenia & fatigue 3. young pt with unexplained wt loss >10% 4. young pt with thrush, Zoster, or Kaposi sarcoma 5. pt who "travels a lot for work" and have a lot of sex |
|
|
Acute retroviral syndrome (initial post-HIV infection sx)
|
Sx of HIV infection can occur 2-3 wks after exposure but 3 wks before seroconversion (so ELISA is still negative): fever, fatigue, lymphadenopathy, HA, pharyngitis, N/V, diarrhea, +/- aseptic meningitis
|
|
|
Most common bug in HIV pt complaining of dyspnea, dry cough, fever, and chest pain? Findings on CXR? 1st line tx?
|

Pneumocystis jiroveci
CXR shows bilateral diffuse symmetric interstitial infiltrates Tx: tmp-smx |
|
|
Diagnose: HIV+ pt with multiple ring-enhancing lesions on CT or MRI
|
CNS Toxoplasmosis
Tx: empiric pyramethamine sulfadiazine + folic acid for 6 wks; if no improvement, consider biopsy for CNS lymphoma |
|
|
Diagnose: HIV+ pt with one ring-enhancing lesion on CT or MRI
|
CNS lymphoma, associated with EBV infection of B-cells
Tx: HAART |
|
|
Diagnose: HIV+ pt with seizure with de ja vu aura and 500 RBCs in CSF
|
HSV encephalitis (predisposed for temporal lobe)
Tx: Give Acyclovir as soon as suspected |
|
|
Diagnose: HIV+ pt with signs/sx of meningitis
|
Cryptococcal meningitis
Diagnosis: positive India ink stain Tx: Amphotericin B (antifungal) |
|
|
Diagnose: HIV+ pt with hemisensory loss, visual impairment, and +Babinski
|
PML: Progressive Multifocal Leukoencephalopathy (widespread demyelinative lesions due to infection of oligodendrocytes by a polyomavirus)
Diagnosis: brain biopsy is gold standard Tx: experimental only (antiretrovirals) |
|
|
Diagnose: HIV+ pt with memory problems and gait disturbance
|
AIDS-Dementia complex
|
|
|
Definition of febrile neutropenia
|
FEVER: single oral temp equal to or greater than 38.3C or 101F AND a febrile state of >38C for at least 1h
NEUTROPENIA: absolute neutrophilic count of <0.5, or a count of <1 with a predicted decline to <0.5 in the next 24 to 48 hours |
|
|
Common cause of febrile neutropenia
|
Mucositis secondary to chemo that causes bacteremia (usually from the gut)
|
|
|
Work-up for febrile neutropenia
|
Tx: blood cx, then 3rd or 4th gen cephalosporin (ie. ceftazadime or cefipime); add Vanco if line infx suspected or if septic shock develops; add Amphotericin B if no improvement and no source found in 5 d
|
|
|
Diagnose: pt with target rash, fever, CN7 palsy, meningitis, and AV block
|
Lyme Disease
Tx: Doxycycline po; heart or CNS disease needs IV Ceftriaxone |
|
|
Diagnose: pt with rash at the wrists and ankles (palms and soles), fever, and headache
|
Rickettsia
Tx: Doxycycline po |
|
|
Diagnose: pt with a tick bite, no rash, myalgia, fever, HA, decreased platelets and WBCs, and increased ALT
|
Ehrlichiosis (tick-borne bacterial infection; bacteria live within WBCs of host)
Tx: Doxycycline po |
|
|
Diagnose: immunosuppressed pt with cavitary lung disease, purulent sputum, weight loss, and fever; Gram+ aerobic branching, partially acid-fast
|
Nocardia (bacteria normally found in soil; disease is one of the "great imitators" bc produces nonspecific sx)
Tx: tmp/smx |
|
|
Diagnose: pt with neck or face infection with draining yellow material (+sulfur granules); Gram+ anaerobic branching
|
Actinomyces
Tx: high dose PCN for 6-12 wks |
|
|
Nephro: causes of hypervolemic hypoNa
|
CHF, nephrotic, cirrhotic causes
|
|
|
Nephro: causes of hypovolemic hypoNa
|
diuretics or vomiting
|
|
|
Nephro: causes of euvolemic hypoNa
|
SIADH (check CXR if smoker!), Addison's, hypothyroidism
|
|
|
If pt has hyponatremia, why should you not rapidly correct their serum Na?
|
HypoNa: Correcting the serum Na faster than 12-24 mEq/day can cause Central Pontine Myelinolysis (severe damage of myelin sheath of neurons in the pons, causing paralysis, dysphagia, dysarthria, etc)
|
|
|
If pt has hypernatremia, why should you not rapidly correct their serum Na?
|
HyperNa: Correcting serum Na faster than 12-24 mEq/day may cause cerebral edema.
|
|
|
Diagnose electrolyte abnormality: pt with peri-oral numbness, +Chvostek or Trousseau sign, and prolonged QT interval
|
Hypocalcemia
|
|
|
Diagnose electrolyte abnormality: "Bones, stones, groans, and psychiatric overtones", shortened QT interval
|
Hypercalcemia
|
|
|
Diagnose electrolyte abnormality: muscle weakness, ileus, ST depression, U waves
|
Hypokalemia
|
|
|
Diagnose electrolyte abnormality: peaked T waves, prolonged PR and QRS, sine waves
|
Hyperkalemia
Tx: Ca-gluconate, then insulin +glucose, kayexalate, salbutamol, and NaHCO3; Dialysis is last resort |
|
|
Diagnose: muddy brown casts in a pt taking Amphotericin or Aminoglycosides or Cisplatin
|
Acute tubular necrosis (ATN)
Tx: fluids, avoid nephrotoxins, dialysis if indicated |
|
|
Diagnose: protein, blood, & eosinophils in the urine, fever and rash, pt took tmp-smx 2 wks ago
|
Acute interstitial nephritis (AIN)
|
|
|
Diagnose: crush victim with very high serum CK, +blood on urine dipstick, but no gross hematuria
|
Rhabdomyolysis, causing hyperkalemia
|
|
|
Indicators for emergent dialysis
|
AEIOU:
A-acidosis E-electrolyte imbalance (esp high K>6.5) I-intoxication (esp antifreeze and Li) O-overload of volume (sxs of CHF or pulmonary edema) U-uremia (pericarditis, altered mental status) *Dialysis not urgently indicated for rising Cr or oliguria alone!! |
|
|
#1 cause of CKD
|
Diabetes mellitus
|
|
|
#2 cause of CKD
|
HTN
|
|
|
#1 cause of death in a CKD pt
|
Cardiovascular disease
|
|
|
Cx of CKD
|
HTN, fluid retention = CHF
normochromic normocytic anemia (loss of EPO) hyperK hyperPO4 (can cause precipitation of Ca into tissues = renal osteodystrophy and calciphylaxis (skin necrosis)) hypoCa Uremia (confusion, pericarditis, pruritus, increased bleeding secondary to uremic-induced platelet dysfunction) |
|
|
Diagnose: elderly pt with painless hematuria
|
bladder cancer until proven otherwise
|
|
|
Diagnose: pt with hematuria and progressive hearing loss & deafness
|
Alport Syndrome ( genetic disorder characterized by glomerulonephritis, endstage kidney disease, and hearing loss); mutation in collagen IV
|
|
|
Diagnose: pt with hematuria 1-2 wks after sore throat or skin infection
|
Post-strep glomerulonephritis
|
|
|
Diagnose: child with viral URI, abdominal pain, arthralgia, and purpura; can cause renal failure
|
Henoch-Schonlein Purpura
|
|
|
Diagnose: child who ate a hamburger and now has diarrhea, renal failure, petechiae, and MAHA (microangiopathic hemolytic anemia)
|
Hemolytic uremic syndrome (HUS) = Most cases are preceded by an episode of infectious, sometimes bloody, diarrhea caused by E. coli O157:H7 or Shigella, which is acquired as a foodborne illness or from a contaminated water supply.
Tx: supportive; don't tx with ABx bc causes release of more toxins Mnemonic: DART - diarrhea, anemia, renal failure, thrombocytopenia |
|
|
Diagnose: cardiac pt with renal failure, MAHA, thrombocytopenia, fever, and altered mental status; pt treated with ticlopidine (plt aggregation inhibitor)
|
Thrombotic thrombocytopenic purpura (TTP)
Tx: plasmapheresis; don't give plts Distinguished from DIC bc PT and PTT are normal ins HUS/TTP Mnemonic pentad of TTP: FARTN = fever, anemia, renal failure, thrombocytopenia, neuro signs |
|
|
Diagnose: + c-ANCA, kidney/lung/sinus involvement
|
Wegener's Granulomatosis
Dx: most accurate test is biopsy Tx: steroids or cyclophosphamide |
|
|
Diagnose: + p-ANCA, renal failure, asthma, and eosinophilia
|
Churg-Strauss Disease (medium and small vessel autoimmune vasculitis, leading to necrosis. It involves mainly the blood vessels of the lungs (it begins as a severe type of asthma), gastrointestinal system, and peripheral nerves, but also affects the heart, skin, and kidneys)
Dx: best test is lung bx Tx: cyclophosphamide |
|
|
Diagnose: + p-ANCA, NO lung involvement, 30% pts are Hep B+
|
Polyarteritis Nodosa (PAN) = affects small/med arteries of every organ except the lungs!
Tx: cyclophosphamide |
|
|
Types of kidney stones and most common
|
Most common: calcium oxalate
Others: cysteine, struvite (Mg/Al/PO4), and uric acid stones |
|
|
Diagnose: pt receiving chemo tx for leukemia who develops flank pain radiating to groin + hematuria
|
Uric acid stone (secondary to increased production of uric acid from purine breakdown during periods of active cell proliferation, especially following chemo treatment in pts with leukemia)
|
|
|
What are the 4 histological subtypes of nephrotic syndrome?
|
1. MCD = minimal change disease
2. FSGS = focal segmental glomerulosclerosis 3. MN = membranous nephropathy 4. MPGN = membranoproliferative glomerulonephritis |
|
|
Most common cause of nephrotic syndrome in kids
|
Minimal change disease (fusion of podocyte foot processes on electron microscopy)
Tx: steroids |
|
|
Most common cause of nephrotic syndrome in adults
|
Focal Segmental Glomerulosclerosis (FSGS)
= The individual components of the name refer to the appearance of the kidney tissue on biopsy: focal—only some of the glomeruli are involved (as opposed to diffuse), segmental—only part of each glomerulus is involved (as opposed to global), glomerulosclerosis—refers to scarring of the glomerulus |
|
|
Second most common cause of nephrotic syndrome in adults
|
Membranous glomerulonephritis (MGN)
= slowly progressive disease of the kidney affecting mostly patients between ages of 30 and 50 years, usually Caucasian; 85% idiopathic (aka unknown cause) |
|
|
Which secondary cause of nephrotic syndrome is associated with chronic hepatitis and low complement?
|
Membranoproliferative glomerulonephritis (MPGN)
|
|
|
Which secondary cause of nephrotic syndrome is associated with heroin use and HIV?
|
Focal Segmental Glomerulosclerosis (FSGS)
|
|
|
What should you suspect if a nephrotic syndrome suddenly develops flank pain?
|
Suspect renal vein thrombosis secondary to hypercoagulable blood b/c loss of anticoagulants in urine (antithrombin III, protein C & S)
|
|
|
Diagnose: 30 yo F with thrombocytopenia, recurrent epistaxis, menorrhagia, and petechiae. Decreased plts only.
|
ITP
Tx: prednisone 1st line, then splenectomy |
|
|
Diagnose: 20 yo F with recurrent epistaxis, menorrhagia, petechiae, NORMAL plts, increased bleeding time and PTT
|
VWD
Tx: dDAVP for bleeding or pre-op; replace Factor 8 (which contains vWF) if bleeding continues |
|
|
Diagnose: 20 yo M with recurrent bruising, hematuria, hemarthroses, and increased PTT
|
Hemophilia
Tx: if mild, use dDAVP, otherwise replace factors |
|
|
Diagnose: pt develops arterial clot 1 wk post-op. Her plts are 50% less than pre-op.
|
Heparin-induced thrombocytopenia (HIT)
Tx: stop heparin, reverse warfarin with Vit K |
|
|
DDx of unprovoked thrombus
|
-CANCER
-OCPs or HRT -nephrotic syndrome -lupus anticoagulant -protein c/s deficiency -+Factor 5 Leiden gene -Antithrombin III deficiency |
|
|
What are examples of "great imitator" diseases? (diseases which can be confused with others and which feature nonspecific sx)
|
-cancer
-fibromyalgia -MS -systemic lupus erythematosus -sarcoidosis -Infectious diseases: Lyme disease, Syphilis, & Nocardiosis -Celiac -Addison's -PE |
|

Diagnose: pt with knee pain, DIP involvement, no swelling or warmth at joints, worse at the end of the day, crepitus
|
OA
|
|

Diagnose: pt with arthritis at PIP and wrists bilaterally, worse in the AM, low grade fever
|
RA
|
|

Diagnose: pt with arthritis at DIP joints, rash with silvery scale on elbows and knees, pitting nails, and swollen fingers
|
Psoriatic arthritis
|
|
|
Diagnose: symmetric bilateral arthritis, malar rash, oral ulcers, proteinuria, thrombocytopenia. Arthritis is not erosive or have lasting sequelae.
|
SLE
|
|
|
Diagnose: Pt with acute swollen painful joint and aspirated fluid with needle-shaped, negatively birefringent crystals
|
Gout (monosodium urate crystals)
|
|
|
Acute and chronic tx of gout
|
Acute tx: indomethacin & colchicine (steroids if CKD)
Chronic tx: Allopurinol if overproduction of crystals, Probenecid if undersecretion of crystals |
|
|
Diagnose: pt with acute swollen painful joint and aspirated fluid with rhomboid-shaped, positively birefringent crystals
|
Pseudogout (calcium pyrophosphate)
Tx: NSAIDs, colchicine, corticosteroids |
|
|
Which Abs are most sensitive for SLE?
|
Anti-dsDNA and Anti-Smith
|
|
|
Abs positive in Sjogren's syndrome
|
Anti-Ro and Anti-La
|
|
|
Ab positive in CREST syndrome
|
Anti-Centromere
|
|
|
Abs positive in Systemic Sclerosis
|
Anti-Scl-70 and Anti-topoisomerase
|
|
|
What is CREST syndrome?
|
Limited cutaneous form of systemic scleroderma:
C - calcinosis R - Raynaud's E - esophageal dysmotility S - sclerodactyly T - telengiectasia |
|

Name this skin sign of systemic disease (may indicate internal malignancy): explosive onset of multiple seborrheic keratoses
|
Sign of Leser-Trelat
|
|

Diagnose: pt has this skin finding and also has difficulty combing hair and getting up from a chair
|
Dermatomyositis features:
-heliotrope rash -Gottron's papules -periungal erythema -proximal muscle weakness |
|

Pruritic rash that begins on extremities, lasts 7-10 d, unknown cause
|
Erythema multiforme
|
|

What is the Ddx of this skin findings (brown to black, poorly defined, velvety hyperpigmentation of the skin)
|
Acanthosis nigricans:
-occurs in individuals younger than age 40, may be genetically inherited, associated with obesity or endocrinopathies, such as: - hypothyroidism or hyperthyroidism, -acromegaly, -polycystic ovary disease, -insulin-resistant diabetes, -Cushing's disease |
|

Diagnose: 50 yo male presenting with blisters which become ulcerated in areas of the skin exposed to sunlight, especially on the face, ears and dorsum of the hands; his labwork shows iron overload
|
Porphyria cutanea tarda:
-a genetic photosensitive skin disease with onset in adult life with substances called uroporphyrins in the urine due to a deficiency of uroporphyrinogen decarboxylase (UROD), an enzyme required for the synthesis of heme -The hallmarks of porphyria cutanea tarda (PCT) are blisters which become ulcerated in areas of the skin exposed to sunlight -Iron overload is frequently present in porphyria cutanea tarda and may be associated with varying degrees of damage of the liver |
|
|
What is the precursor lesion of squamous cell carcinoma?
|
Actinic keratosis
|
|
|
What are the 4 subtypes of melanoma?
|
1. Superficial spreading (most common, best prognosis)
2. Nodular (poor prognosis) 3. Acral-lentiginous (palms, soles, mucous membranes, more prevalent in darker skin individuals) 4. Lentigo maligna (head & neck, good prognosis) |
|
|
What is the #1 prognostic indicator for melanoma?
|
Breslow's depth: tumor thickness remains the most powerful prognostic indicator hence why it's critical to get a full-thickness biopsy
|
|
|
Most common pituitary adenoma?
|
Prolactinoma
-consider if pt presents with amenorrhea or hypothyroidism |
|
|
Treatment of prolactinoma
|
1. Bromocriptine = dopamine agonist that decreases synthesis and secretion of prolactin; long track record and safety, dosed daily
2. Cabergoline = long-acting dopamine agonist, better safety and efficacy profile; convenience of twice-weekly administration |
|
|
What are the causes of hypopituitarism? (mnemonic: 8 "I"s)
|
❏ Mnemonic: eight “I”s
• Invasive: generally primary tumours • Infarction: e.g. Sheehan’s syndrome • Infiltrative disease e.g. sarcoidosis, hemochromatosis, histiocytosis • Iatrogenic: following surgery or radiation • Infectious: e.g. syphilis, TB • Injury: severe head trauma • Immunologic: autoimmune destruction • Idiopathic: familial forms, congenital midline defects |
|
|
In hypopituitarism, what is the sequence of hormone loss?
|
A compressive adenoma in the pituitary will impair hormone production in this order (i.e. GH-secreting cells are most sensitive to compression)
Mnemonic: “Go Look For The Adenoma Please” 1. GH 2. LH 3. FSH 4. TSH 5. ACTH 6. Prolactin |
|
|
Diagnose: pt presents with polyuria, polydipsia, hyperNa, and dilute urine
|
Diabetes Insipidus (lack of ADH)
|
|
|
How do you distinguish between central and nephrogenic Diabetes Insipidus.
|
Do a water deprivation test:
Central DI = urine osmolality still decreased after water deprivation test, but increases with administration of dDAVP Nephrogenic DI = urine osmolality still decreased after water deprivation test and administration of dDAVP (1st line tx: HCTZ and amiloride to reduce flow to the ADH-sensitive distal nephron) |
|
|
What are the 5 types of thyroid cancer?
|
1. Papillary = most common, characterized by psammona bodies on histology (round collection of Ca), spreads via lymphatic system, good prognosis
2. Follicular = hematogenous spread, more aggressive, must do total thyroidectomy 3. Medullary = associated with MENII (look for pheochromocytoma and hyperparathyroidism=hyperCa), amyloid on histology, secrets calcitonin 4. Hurthle cell 5. Anaplastic/undifferentiated = giant cells on histology, poor prognosis |
|
|
7 "P"s of papillary thyroid carcinoma
|
PAPILLARY CANCER:
Popular (most common) Psammoma bodies Palpable lymph nodes (bc lymphatic spread) Positive Iodine131 uptake Positive prognosis Postoperative Iodine131 scan to dx/tx metastases Pulmonary metastases |
|
|
3 "F"s of follicular thyroid carcinoma
|
FOLLICULAR CANCER:
Far-away metastasis (spreads hematogenously) Female (3 to 1 ratio) Favorable prognosis |
|
|
4 "M"s of medullary thyroid carcinoma
|
MEDULLARY CANCER:
MEN II aMyloid (histology) Median lymph node dissection Modified neck dissection if lateral nodes are positive |
|
|
Diagnose: female pt presenting with osteoporosis, central obesity, diabetes, and hirsutism
|
Suspect Cushing's syndrome
Best screening test: 1 mg overnight dexa suppression test or 24h urine cortisol If dexa test abnormal, next best test is 8 mg overnight dexa suppression If suppression <50% of control = pituitary adenoma (Cushing's Disease) If no suppression = either adrenal neoplasia OR ectopic ACTH (measure plasma ACTH, chest CT if smoker, abdo CT) |
|
|
Diagnose: pt presenting with weakness, weight loss, hypotension, hyperpigmentation, hyperK, and hypoNa
|
Suspect adrenal insufficiency = main cause is Addison's Disease (autoimmune adrenal destruction)
Tx: long-term replacement of aldosterone (ie. with fluodrocortisone) and cortisol (ie. with hydrocortisone or prednisone), androgen replacement tx in women |
|
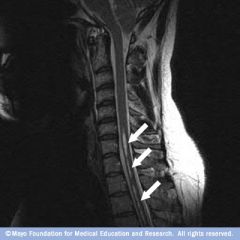
Diagnose: pt involved in MVA with whip-lash presents with loss of pain and temperature sensation on neck and arms and intact sensation
|
Suspect post-traumatic syringomyelia = CSF from the central spinal canal dissects into the surrounding white matter, forming a cystic cavity or syrinx
|
|
|
Diagnose: pt with chronic high cholesterol presents with acute onset of flaccid paralysis below the waist, loss of pain/temp with preserved vibration of position sense
|

Suspect anterior spinal artery occlusion (aka Beck's Syndrome)
-affects the spinothalamic tract (pain/temp) and corticospinaltract (motor), but not the dorsal columns (proprioception) |