Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
59 Cards in this Set
- Front
- Back
|
What is a lymphoma?
|
A lymphomas is a proliferation of lymphocytes which typically presents with enlargement of the spleen and/or lymph nodes.
|
|
|
What organs are commonly infiltrated by lymphoma?
|
Liver, lung and bowel
|
|
|
What type of lymphoma is on the rise?
|
Incidence of Non-Hodgkin's Lymphoma has been on the rise for 60 years.
|
|
|
How is the diagnosis of lymphoma made?
|
Lymphoma Dx is based on excisional biopsy of a centrally-involved lymph node.
|
|
|
How is Hodgkin's Lymphoma staged?
|
By the degree of dissemination of the disease.
Stage 1 - Single node Stage 2 - Multiple nodes, same side of diaphragm Stage 3 - Multiple nodes, both sides of diaphragm Stage 4 - Disseminated disease with extra-lymphatic involvement |
|
|
What is the characteristic histologic finding in Hodgkin's Lymphoma?
|
The "Reed-Sternberg" Cell
|
|
|
What composes the bulk of a Hodgkin's tumor?
|
Unlike other malignancies, most cells in a Hodgkin's tumor are normal. Only a few are the binucleate "Reed-Sternberg" cells.
|
|
|
What the two broad sub-types of Hodgkin's Lymphoma?
|
1) Classical Hodgkin's
2) Nodular Lymphocyte Predominant Hodgkin's Disease (NLPHD) |
|
|
What are the four sub-types of Classical Hodgkin's Disease?
|
1) Lymphocyte Rich (rare - good prog.)
2) Nodular Sclerosis (50% - good prog.) 3) Mixed Cellularity (40% - med. prog.) 4) Lymphocyte Depletion (5% - worst prog.) |
|
|
What are B-Symptoms in Hodgkin's Disease?
|
Constitutional symptoms: fever, night sweats, unexplained weight loss of more than 10% in the past 6 months.
|
|
|
What imaging technique can differentiate an active HD tumor?
|
PET Scan
|
|
|
What is the primary goal in the treatment of Hodgkin's Disease?
|
HD is treated for CURE, so accurate staging and chemotherapy is critical.
|
|
|
What is the therapy for Hodgkin's Disease? What are the cure rates?
|
Limited Chemo + Limited Radiation. Cure rates are 70-90%
|
|
|
What is the modern chemo regimen for Hodgkin's Disease?
|
Hodgkin's: ABVD
A - Adriamycin B - Bleomycin V - Vinblastine D - DTIC |
|
|
What are the older chemo regimens for Hodgkin's Disease?
|
MOPP
|
|
|
How is prognosis and therapy determined for Non-Hodgkin's Lymphomas (NHLs)?
|
The histologic pattern seen in involved lymph nodes.
|
|
|
What are the two most important lymph features in NHL?
|
1) Overall architecture (diffuse or clustered)
2) Individual tumor cell appearance (large vs. small cells) |
|
|
From what cell lines are NHL tumors derived?
|
85% from B-Cells
15% from T-Cells |
|
|
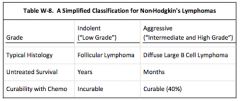
What are the two types of NHL classifications for this course?
|
"Indolent/Low Grade" and "Aggressive/Intermediate & High Grade"
|
|
|
Describe the Classification, Histology, Mean survival, and Chemo for NHL.
|
|
|
|
What is the typical clinical presentation of NHL?
|
Painless Adenopathy.
|
|
|
Which lymphomas are curable?
|
Aggressive lymphomas are often more curable than indolent ones.
|
|
|
What chemotherapy drug seems to be key in curing aggressive lymphoma?
|
Doxorubicin (Adriamycin)
|
|
|
What are the treatment options for INDOLENT NHL?
|
Stage 1-2 Indolent: radiotherapy alone (50% cure)
Stage 3-4: no therapy, or chlorambucil, CVP and/or rituximab (CD20) |
|
|
What does Rituximab recognize?
|
The CD20 antigen
|
|
|
What's CVP, and what disease is it used for?
|
CVP is a chemo regimen for Indolent Stage 3-4 NHL
* Cyclophosphamide * Vincristine * Prednisone |
|
|
What is the standard chemo for an Aggressive Non-Hodgkin's Lymphoma?
|
CHOP:
* Cyclophosphamide * Doxorubicin (Hydroxydaunorubicin) * Vincristine (Oncovin) * Prednisone |
|
|
How often can remission be induced with CHOP therapy for NHL?
|
60-80% of aggressive NHL patients will go into remission
|
|
|
What is a Plasma Cell Dyscrasia?
|
Disorders of the plasma, or B-Cells, that often generate extra antibodies. Examples are multiple myeloma and Waldenstrom's macroglobulinemia.
|
|
|
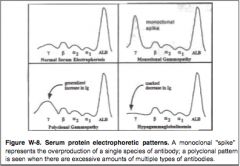
Describe the following Serum Protein Electrophoresis (SPEP) curves:
1) Normal Pattern 2) Polyclonal Gammopathy 3) Monoclonal Gammopathy 4) Hypogammaglobulinemia |
|
|
|
What are the four major Plasma Cell Dyscrasias?
|
1) Multiple Myeloma
2) Waldenstrom's Macroglobulinemia 3) Primary Amyloidosis 4) Monoclonal Gammopathy of Undetermined Significance (MGUS) |
|
|
What are the four clinical manifestations of the plasma cell disorders?
|
1) the tumor
2) Paraproteins made by the tumor 3) Decreased normal Ig proteins 4) Other factors produced by the tumor |
|
|
What is Mutiple Myeloma?
|
A malignant disorder characterized by the monoclonal proliferation of plasma, or "myeloma," cells.
|
|
|
How does MM typically present?
|
MM commonly presents as "bone pain," esp. in the vertebrae, ribs and long bones. Anemia, thrombocytopenia and neutropenia are common.
|
|
|
What are focal collections of myeloma cells called? How might they present?
|
Plasmacytomas, which might present as subcutaneous nodules.
|
|
|
Why are lytic lesions common in MM?
|
MM tumor cells produce TNF-Beta, which activates osteoclasts and increases bone resorption.
|
|
|
What is the most common lab abnormality in MM?
|
A hypo-proliferative anemia, along with "rouleax" RBCs.
|
|
|
What is a "rouleaux" finding?
|
RBCs stacking on the peripheral smear. Increased serum IgG binds to RBCs, decreasing the normal ionic repulsion between them.
|
|
|
What is the key diagnostic tool in MM?
|
Serum Protein Electrophoresis (SPEP). A prominent MONOCLONAL M-Spike will show.
|
|
|
What classic urine finding is associated with MM?
|
Bence Jones Proteinuria. About 10% of MM will produce the Ig Light Chain proteins, which are small enough to be excreted in the urine.
|
|
|
What are the marrow findings with MM? Is marrow biopsy a required test with MM?
|
MM requires marrow biopsy. Typical findings include 10-30% malignant plasma cells. Easier to detect on biopsy than aspirate.
|
|
|
What are the 4 diagnostic characteristics of MM?
|
1) >10% abnormal plasma marrow cells
2) Serum or urine monoclonal gammopathy 3) Lytic bony lesions 4) Plasmacytomas Not all features are required to make the diagnosis. |
|
|
What are the common clinical complications of MM?
|
1) Renal Failure
2) Pathologic Fractures 3) Paraprotein assoc. with hyperviscosity |
|
|
What are the issues commonly associated with high levels of paraprotein in MM?
|
1) Hyperviscosity leading to vascular stasis
2) Interference with platelet function leading to mucosal bleeding 3) Suppression of normal plasma cell growth and decreased normal Ig |
|
|
Is there a curative therapy for MM?
|
No, only palliative therapies and stem cell transplant.
|
|
|
What is a suggested palliative chemotherapy for MM?
|
1) Thalidomide & Dexamethasone
2) Lenalidomide & Dexamethasone 3) Lenalidomide & Bortezomib (relapse) |
|
|
How might local MM plasmacytomas be managed?
|
Local radiation therapy may be used to control painful tumors.
|
|
|
What can be done about bone resorption in MM?
|
Bisphosphonates reduce bone resorption in MM, and may even be toxic to tumor cells.
|
|
|
What is Waldenstrom's Macroglobulinema?
|
A hyperviscous plasma disease similar to MM.
|
|
|
What proteins are produced in WM? Is this clinically important?
|
IgM proteins. Because they are so large, complications of hyperviscosity are more common on WM.
|
|
|
What are the symptoms of hyperviscosity syndrome?
|
1) Headache
2) Confusion 3) Visual disturbances 4) Difficulty hearing 5) Coma |
|
|
What is the "Classic Triad of Hyperviscosity?"
|
1) Bleeding (epistaxis, ecchymosis)
2) Visual changes (blurred) 3) Neurologic changes (HA, dizziness) |
|
|
What are the laboratory findings in WM?
|
Marked increase in IgM in Serum Plasma Electrophoresis. Pancytopenia is possible with extensive marrow replacement
|
|
|
How is WM treated?
|
There is no cure for WM. Drugs include:
* Chlorambucil * Fludarabine * Rituximab |
|
|
What is the median survival time for WM?
|
Approx. 5 years
|
|
|
How is hyperviscosity managed acutely?
|
Plasmapheresis
|
|
|
What are the clinical features of Amyloidosis?
|
Fatigue, weakness, weight loss, dyspnea, purpura and EDEMA.
|
|
|
How is Amyloidosis diagnosed?
|
Isolation of amyloid protein with apple-green birefringence in tissue samples. Bone marrow biopsy is also performed
|
|
|
What does Congo Red staining in the marrow indicate?
|
Amyloidosis
|