Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
30 Cards in this Set
- Front
- Back
|
What is the earliest recognizable erythroid precursor called?
How does it differ from a mature erythrocyte? |
Pronormoblast (proerythroblast)
It has a large nucleus and blue cytoplasm. As cell matures, nucleus shrinks and is extruded and cytoplasm becomes hemoglobinized (more pink). |
|
What cells are polychromatic and why? What other feature distinguishes them from mature RBCs?
|
Reticulocytes --> both pink and blue mixed. They are enucleated but retain some cytoplasmic ribosomes which give bluish color
Retics are also slightly larger than RBCs. *use Supravital Stain to identify |
|
What does the presence of these cells in the circulation indicate?
|
(nucleated RBCs in peripheral blood) = Abnormal state
Breakin bone-marrow and blood barrier or extramedullary hematopoiesis |
|
|
Where in the body is EPO produced. How does anemia lead to increased EPO production?
|
EPO made in the kidney (mostly) and liver.
"Feedback loop" Anemia --> ↓ O2 production --> O2 sensor in renal tubule detects --> kidney produces EPO to ↑ RBC production |
|
|
What cytokines/growth factors other than EPO contribute to erythropoiesis (RBC production). Hint: there are three.
What happens to EPO levels in anemia? |
SCF (stem cell factor), IL-3, and GM-CSF
In anemia, EPO levels increase (to make more RBCs) |
|
|
What is meant by "Hemoglobin" when it is measured in the lab?
Why are the normal values different in men vs. women? |
Hb: gm of Hb / dL of whole blood
Men 15 ± 1.7, RBC count million/ul Women 13 ± 1.5 |
|
|
What is the definition of "Anemia"?
|
Low circulating RBC mass
Either due to decreased number of RBCs, or decreased Hb content. |
|
|
What is a normal HCT? How is it measured?
Clinical pearl: If a person's measured Hb is 13, how do you approximate HCT? |
HCT= VOLUME of RBCs (when blood is centrifuged, divide packed RBC by total volume of blood including plasma and buffy coat)
HCT is roughly 3 x Hb. So 39 %. |
|
|
What is the effect of the following on Hb:
1. Dehydration 2. Pregnancy 3. High altitude 4. Gender (male) 5. Increased age |
1. Dehydration- ↑ Hb ( plasma vol is low)
2. Pregnancy- ↓ Hb (plasma vol high) 3. High altitude- ↑ Hb (because EPO levels ↑) 4. Male- ↑ Hb (androgens stimulate BM to make RBC) 5. Age- slight decrease in RBC production |
|
|
Symptoms of anemia?
What specific history do you want to get that would clues to underlying diagnosis? |
SOB, Fatigue, Angina, Palpitations, headache
Blood loss (menstruation, surgery) Diet (Alcohol intake- EtOH suppress BM, cirrhosis causes splenomegaly, Vegan) Family hx (thalassemia, sickle cell, etc.) Medications ROS: pica (eating clay, chalk, dirt), neuropsych hx. |
|
|
What physical exam findings are consistent with anemia?
|
Orthostatic hypotension, Conjunctival pallor, Reflex tachy
Jaundice (suggests hemolysis), heart mumur (damaged valve), blood in stool, splenomegaly, Parasthesia/spasticity (B12 deficiency), koilonychia |
|
|
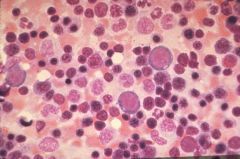
Anemia, neutropenia, and thrombocytopenia suggest what condition?
Elevated WBCs with blasts plus anemia and thrombocytopenia suggest what condition? |
Pancytopenia--> aplastic anemia or malignancy in bone marrow
Acute leukemia (failure of maturation of WBCs) |
|
|
What is a normal MCV? How is it calculated?
What are 3 causes of microcytic anemia? |
Normal mean corpuscular volume or size of RBC = 80-100. (10 x Hct)/ RBC count.
Microcytic <80 1. Fe deficiency 2. ↓ Heme synthesis (lead poisoning) 3. ↓ Globin synthesis (Thalassemia) |
|
|
What are 4 causes of macrocytic anemia?
|
Macrocytic= MCV >100
1. Megaloblastic anemia (B12 deficiency, folate deficiency) 2. Increased Retics 3. Increased Target cells (liver disease) 4. Myelodysplasia |
|
|
What is the MCV in anemia from acute blod loss pre compensation? what about after compensation?
|
Normocytic initially.
After compensation- macrocytic (because of ↑ retics) |
|
|
What does the RDW measure?
|
RBC distribution width = measures variability in size of RBC aka. anisocytosis
*can help distinguish Thalassemia from Fe-deficiency anemia |
|
|
Formula for reitculocyte count? What is a normal Retic count?
What is a more accurate expression of reticulocyte count and how do you calculate it? |
# Reticulocyte/ Total RBCs
Normal = 1% Reticulocyte index= retic count x (pt Hb/ nl Hb) *this adjusts for the degree of anemia |
|
|
Elevated reticulocyte indexes suggest what type of anemias?
What about normal or low retic indexes? |
Elevated= BM appropriately responding (ex: acute bleed or hemolytic anemia)
Normal/Low= impaired BM rbc production (ex: Fe, B12, folate deficiency, tumors or lymphoma replacing marrow, or aplastic anemia) |
|
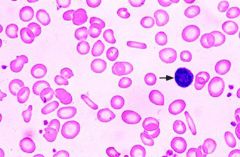
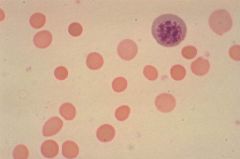
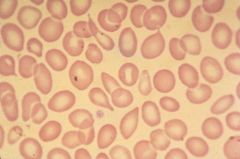
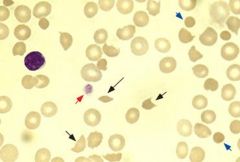
What type of anemia is shown here? How can you tell? What does the arrow point to? What is the MCV?
|
Fe deficiency Anemia-
1) Microcytic, 2) central pallor >1/3rd of cell, 3) pencil cells (elongated RBCs) Arrow= lymphocyte. MCV = microcytic |
|
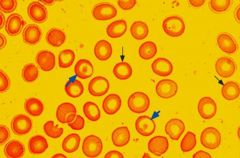
What type of anemia is shown here? What is the MCV?
|
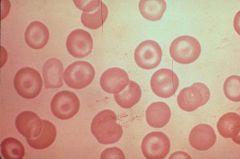
Thalassemia (problem in globin production). Target cells = large. Macrocytic.
|
|
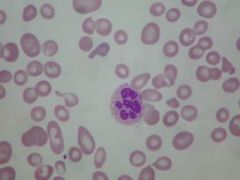
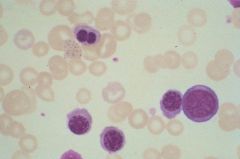
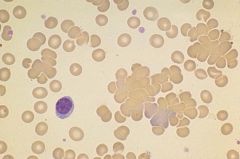
What type of anemia is shown here? What would the MCV be? What about the retic index?
|
B12 deficiency (megaloblastic anemia). Macrocytic. Note the hypersegmented polys.
Retic index is normal to low (inappropriate compensation). |
|
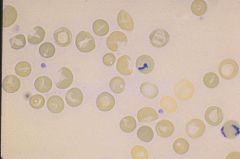
What are these cells called? What two conditions are characterized by these cells?
What RBC index would you expect to be elevated? |
Spherocytes (no central pallor, tiny RBC packed with Hb).
1. Hereditary Spherocytosis, 2. Warm autoimmune hemolytic anemia MCHC = Mean corpuscular Hb conc. is essentially Hb/HCT.Elevated in diseases that cause spherocytes |
|
This type of cell is seen in what two conditions?
|
Teardrop cells-
1. Myelofibrosis, 2. metastatic cancer of BM |
|
What are these cells called? What conditions might they be seen in?
|
Schistocytes (helmet cells), seen in some hemolytic conditions (ex: chewed up RBC or going past poorly fitted aortic valve).
|
|
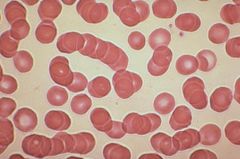
This particular pattern of RBCs is seen in what condition?
|
Rouleaux cells- Multiple Myeloma (RBCs lose normal charge that repels cells and they stack on each other)
|
|
What is seen here? What is it associated with?
|
Non-specific RBC clumping
Cold Autoantibodies --> Cold agglutinin disease |
|
This finding indicated what about the patient?
|
Howell-Jolly bodies
That they are asplenic (usually spleen removes the tiny nuclear remnant that stays behind when nucleus is extruded from RBC). |
|
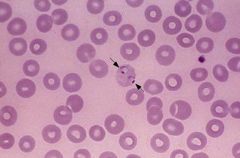
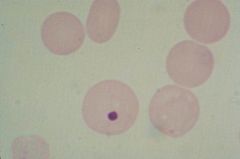
What is seen in the cell that the arrow is pointing to?
|
Sporozoites
*seen in Malaria (always consider when pt has travel history + cyclic/chronic fever and fatigue) |
|
|
What is the most common cause of anemia worldwide? If you see it, what should you immediately evaluate for?
|
Fe-deficiency anemia. Evaluate for blood loss, especially occult GI bleed.
|
|
When do you examine Bone Marrow in a patient with anemia?
What is beneficial about doing an aspirate? a biopsy? |
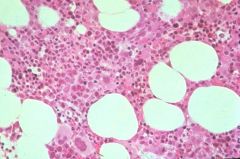
Examine BM when there is low retic count and cause of anemia is not clear from preliminary testing.
BM aspirate- gives cellular detail, BM biopsy- appreciate marrow architecture |