Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
38 Cards in this Set
- Front
- Back
|
Schizophrenia non-genetic correlates
|
-Families with Expressed Emotion (EE) (?)
- Virus (during 2nd trimester) - Pregnancy complications - Birth complications - Stress vulnerability (inc. genetic vulnerability to developing psychosis when stressed) |
|
|
Percent of population w/ Schiz.
|
1.3%
(of that percentage 8% are sibling of patinet, 45-50% identical twin of patient, 15% paternal twin of patient, 12% child w/ ill parent, 40-45% child w/ 2 ill parents) |
|
|
Dopamine levels & Schizophrenia - explain the correlation
|
Foundation of Schiz is associated with Dopmine receptors in the temporal lobe and basal ganglia - Temporal lobe is accelerating, frontal lobe is slowing down -> the disconnect betwen the 2
|
|
|
Associated Neurotransmitters
|
- GABA : loss of GABA -> hyperactivity of dopamine
- Serotonin (5HT) - Norepinephrine (NE) (NE and 5HT modulate Dopamine system) - Glutamate: abnormal neural maturation (mostly seen in young men w/ shiz.) |
|
|
Schizophrenia biological correlations
|
Hypofrontality: frontal lobe shown to have dec. blood flow and glucose metablolism.
Temporal lobe is smaller in size : not seen in all patients -> affects information processing (hypoactivity -> memory difficult b/c cognition impaired) Bilateral hemisphere - prefrontal and frontal dysfunctions. |
|
|
Positive and Negative Symptoms
-distinguishing characteristics - types of each |
- Positive - result of overactivity, acute onset, normal social functioning during remission, favorable response to antipsychotic meds,
hallucinations, delusions, bizarre/ disorganized behav., positive formal thought disorder. - Negative - result of underactivity; gradual onset, premorbid history of emotional problems, chronic deterioration, atrophy on CT scans, harder to treat, last longer, more severe - The 5 A's on separate card |
|
|
Hallucinations:
Types of and top 3 most common |
Image (or sensation) that occurs w/o an external stimulus
- Auditory (75-90%) - Visual (49%) -Tactile (20%) - Olfactory - Gustatory Hallucinations can worsen – from commenting to conversations w/ one another. Command hallucinations that tell the person to do things. |
|
|
Delusions:
Types of |
NOT VALIDATED IN REALITY
A fixed false belief that is contrary to the persons educational and cultural background. - Persecution (81%) - Ideas of reference (49%) - things in envirn. are b/c of them -war, bad weather - Grandeur (39%) - important status "advisor to Al Gore" - Somatic (28%) -brain is rotting, pregnant w/ 9 babies - Control (broadcasting, insertion, w/drawl): their thoughts are being controlled, they think people can hear their thoughts (broadcasting), insertion – someone put them their, withdrawl – someone has removed their thoughts b/c they cant think clearly anymore. |
|
|
Difference between bizarre and non bizarre behaviors
|
- Bizarre – could not be possible, “someone stole my kidneys overnight” and have no scars to prove it.
- Non-bizarre – is possible, “FBI is following me” |
|
|
Speech Assessment
- Poverty of speech - Poverty of content of speech - POSITIVE FORMAL THOUGHT DISORDER |
POSITIVE FORMAL THOUGHT DISORDER
- Word Salad: jumble of words that is meaningless - Flight of Ideas: - Neologism: making up words - Clang Association: using words that sound the same - Echolalia: repeat everything you say |
|
|
The 5 A's of Schizophrenia
(Negative Symptoms) |
- Affective flattening: lack of facial features, look sad but are not
- Alogia - impoverished thinking and cognition - Anhedonia: lack of ability to experience pleasure - Attentional impairment - Avolition: lack of initiative of energy |
|
|
Cognitive Symptoms of Schiz.
|
Concrete thinking
Loss of Ego boundaries depersonalization: loss of identity or that part of self is unreal derealization: false perception that environment has changed |
|
|
Affective Disturbances of Schiz.
|
Restricted/ constricted
Bluted Flat Inappropriate Labile Aggressive |
|
|
Behavioral Features of Schiz.
|
- Automatism – slow, rigid movement
- Avolition – stay in one place - Catatonia –absence of movement, unusual postures – keeping arm in the air - Exhopraxia – mechanic movement - Negativism - resistance - Sterotypy – repetitive movement - Waxy Flexibility – mold the person like wax, put them in positions and they will stay there. |
|
|
Social Changes
Examples of Direct and Indirect |
Direct
–deterioration of social skills and mistrust –lossofdrive/motivationloss of drive/motivation –inability to communicate –deterioration of personal hygiene • Indirect –poor academic/vocational performance – |
|
|
MSA (Mental Status Assessment) Observations
- Cognitive Changes - Affective Changes - Behavioral Changes - Speech Changes |
- Cognitive: concrete thinking, thought processes
- Affective: blunted, negative, congruency w/ thought - Behavioral: appearance, gestures, mannerisms - Speech: tone, amount, clarity |
|
|
Suicide risk for Schiz
- % that attempt? - % that succeed? - highest risk? |
50% attempt
10-15% at some point succeed males < 30, college educated, unemployed, recent hospitalization, history of prior depressive episode |
|
|
Peak onset of Schiz for men and women.
|
men 15-25 yo
women 25-35 |
|
|
Dual diagnosis often associated with Schizophrenia
|
- ETOH abuse/ dependence (40-50%)
- 15-25% marijuana abuse - 5-10% cocaine abuse - 80-90% nicotine dependence people w/ dual diagnosis have more pronounced psychotic episodes, less compliant w/ treatment. Smoking can dec. effects of meds. |
|
|
Phases of Illness
|
1) Prodromal - precedes Active phase by one month to one year. Gradual development of symptoms w/ derterioration of social skills. Avg. time of phase is 6 months, unusual habits or speech may develop
2) Residual Affective flattening and role impairment, more negative symptoms over time. |
|
|
Characteristic Symptoms of Schizophrenia
|
-delusions
-hallucinations -disorganized speech -grossly disorganized or catatonic -behavior -negative symptoms (5 A's) *Must have 2 or more present in 1 month period. *40% will have one accute episode, but then controlled by medication, 40% have frequent episodes, 20% servere, need to be institutionalized |
|
|
Types of Schizophrenia
|
1) Paranoid Type
2) Catatonic Type 3) Disorganized Type 4) Undifferentiated 5) Residual Type |
|
|
Criteria for being diagnosed w/ Schizophrenia
|
1) Characteristic symptoms - 2 ore more present in 1 month period.
2) Dysfunction in major life area - work, school, self care. 3) Duration - 2 or signs then have the prodromal signs (gradual development of symptoms w/ derterioration of social skills. 6 mon. of continuous signs, 1 month of symptoms *If you are able to function normally w/ symptoms you should TECHNICALLY not be diagnosed w/ mental illness. |
|
|
Paranoid Type Schiz.
- Characteristic symptoms - Not prominent symptoms |
Preoccupation with one or more DELUSIONS or frequent AUDITORY hallucinations
*None of the below are prominent -disorganized speech - disorganized or catatonic behavior - flat or inappropriate affect Onset is later 35-40yo., treatment is more successful. Most common type of schiz. |
|
|
Catatonic Type Schiz.
|
2 of the following are present:
- motor inflexibility - excessive motor activity - extreme negativism or mutism - preculiarities of voluntary mvmt - inappropriate or bizarre postures - echolalia or echopraxia |
|
|
Disorganized Type Schiz.
|
ALL are prominent
- disorganized speech - disorganized behavior - flat or inappropriate affect Catatonic criteria are not met Early onset (teens), most impaired, poor outcomes, common to have family hx. of psych illness. |
|
|
Undifferentiated Type Schiz.
|
Characteristic symptoms are met, but cannot be classified into paranoid, disorganized, or catatonic types.
|
|
|
Residual Type Schiz.
|
Presence of 2 or more characteristic symptoms & negative symptoms BUT
Absence of positive symptoms - delusions, hallucinations, disorganized speech, and grossly disorganized or catatonic behavior |
|
|
Schizophreniform Disorder
|
Characteristic symptoms present, but episode (includ prodromal, active, and residual) lasts at least 1 month but less then 6 mon.
|
|
|
Schizoaffective Disorder:
subtypes: Criteria: |
Major depressive, manic, or mixed episode concurrent w/ characteristic symptoms of schiz.
Subtypes: Bipolar (more common in young adults) or depressive type (more common in older adults) Criteria: at least 2 weeks of delusions or hallucinations in the absence of prominent mood symptoms Information on prevalence is lacking, more common in women then men. |
|
|
Delusional Disorder:
Age of oneset, prevalence. Subtypes |
Non bizarre delusions for at least one month. Function not impaired. Can be chronic or have no recurrence.
Age of onset: middle to late adult. Accounts for 1-2% of inpatient admits. Subtypes: Erotomanic (believes one is in love w/ them), Grandiose, Jealous, Persecutory, Somatic |
|
|
Treatment focus for phases of Schiz.
-Acute - Sub-acute - Maintenance |
-Acute: Crisis intervention, SAFETY, Symptom stabilization
-Sub Acute: Stress assessment, daily activities, supports, resources - Maintenance: Understanding and acceptance of illness, Skills (self care, social, vocational), Realistic expectations, Adaptation to deficits |
|
|
Nursing Interventions
-Anxiety - Mistrust |
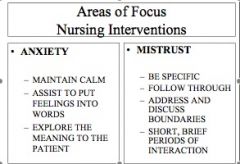
They will test their boundaries. They are trying to establish if they can trust you. Will be seeing if you follow through w/ what you say.
Short brief periods of interaction – that is all they can tolerate. Need be very aware of what you are doing nonverbally, the patients are watching you – they may perceive as threatening or you are laughing at them. |
|
|
Nursing interventions for LOOSE ASSOCIATIONS
|
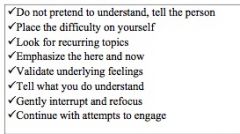
If you don’t understand, “I am having difficulty understanding….” Put the focus on your lack not theirs.
Do point out what you understand to enhance the positive. |
|
|
Nursing Interventions for HALLUCINATIONS
|
Hallucinations – “hearing voices”
• What are they saying? (commanding or demanding – need to know for safety) • Are you frightened by them? • Don’t reinforce what is not real – “I understand what you believe, but I am not seeing/ hearing that.” • If not sure how to bring back to reality say something as simple as “I like your shoes” their shoes are real, interrupts and brings back to reality. • Some will be told to interact w/ their voices – to tell them to STOP! And leave them alone. Be careful where they are instructed to do so. • Auditory hallucinations can be helped by simply wearing ear plugs, it tell the brain they cant hear – shuts off the voices. |
|
|
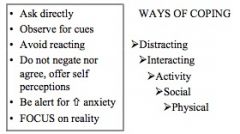
Nursing Interventions DELUSIONS
|

Delusions Interventions
|
|
|
Nurisng Intervention Social Withdrawl
|

Social Withdrawl
|
|
|
Therapy
- Individual focus - Group benefits |
- Indiv.: skills training, cognitive rehabilitation, cognitive content
-Group: Increases: motivation, medication compliance, social competence, self-concept Decreases: withdrawl, anxiety |