Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
38 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Ottawa Charter
|
First International Conference on Health Promotion, Ottawa, 21 November 1986
|
|
|
|
pre-requestists for health
(acc to Ottawa Charter) |
1. peace
2. shelter 3. food 4. income 5. education 6. social justice 7. equity 8. stable ecosystem |
|
|
|
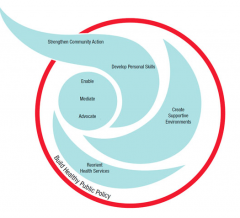
5 key aspects of Ottawa Charter (WHO, 1986)
|
1. build healthy public policy
2. reorient health services 3. create supportive environments 4. strengthen community action 5. develop personal skills and to / by enable, mediate, advocate |
|
|
|
how can you 'advocate'
|
aim to make underlying determinants as favourable as possible
|
|
|
|
how can you 'mediate'
|
consider the interest of more than one group and facilitate compromise
|
|
|
|
how can you 'enable'
|
empowering people to stride towards good health themselves, to reach their fullest potential
|
|
|
|
building healthy public policy -
examples |
no smoking areas, taxation on alcohol, plain packaging for cigarettes, sunsmart,
|
|
|
|
creating supportive environments - examples
|
parks & gardens
playground walkin/bike tracks are you OK day |
|
|
|
strengthen community action - examples
|
setting priorities, helping with implementation
|
e.g. community run activity (clean up Australia day)
|
|
|
developing personal skills - examples
|
information campaigns
|
schools, education
|
|
|
reorienting health services - examples
|
beyond the responsibility for providing clinical services, focus on provention, catering for cultural diversity & minorities
|
|
|
|
upstream intervention
|
extensive and broad in nature, population focused:
policies, education, housing, work environment, social environment, transport, pollution |
organisational development,
economic & regulatory activities, advocacy |
|
|
downstream intervention
|
targeted, explicit proposes, focused on individuals
|
screening procedures (breast screen) risk assessments (work place health checks) immunisation
|
|
|
midstream
|
social marketing, behaviour of audience
health information |
every cigarette is doing you damage, slip-slop-slap-slide, there is noting healthy about a tan
|
|
|
problems might impact
|
1. individuals
2. family/friends 3. workplace/groups 4. community 5. society |
e.g. problem gambling
|
|
|
potential harm of problem gambling (example)
|

|
|
|
|
DHS solutions for problem gambling (example)
|

|
|
|
|
health inequalities
|
measurable differences and disparities in health between groups (Kawachi et al., 2002)
|
|
|
|
health inequities
|
inequalities in health which are deemed unfair or stemming from some form of social injustice (Kawachi et al.,, 2002)
|
|
|
|
social justice
|
fair access to distribution of resources. further, equitable access must supersede individual goad, so that the least advantaged people in the community receive care and services equal to that received by those who are advantaged by resources which incl finances & knowledge (McMurray 2003)
|
example: closing the gap
|
|
|
in the early beginnings of health promotions, health was explored in two ways ...
|
a) our ability to satisfy needs
b) our ability to change or cope with environment |
|
|
|
historical overview
|

|
|
|
|
LaIonde Report (1974)
for the first time looked at/beyond |
- beyond biomedical model
- introduced 'lifestyle' - start with 'at-risk groups' |
|
|
|
Build Healthy Policy
(acc Ottawa Ch.) |
health promotion goes beyond health care and includes legislation, fiscal measures, taxation and organisation change
|
example: buckle up
|
|
|
creating supportive environments
(acc Ottawa Ch.) |
living and working condition that are safe, stimulating, satisfying and enjoyable
|
example: worksafety campagnes
|
|
|
strengthen community action
(acc Ottawa Ch.) |
setting priorities, making decision, planning strategies and implementing them so that communities control of their own destinies
|
examples: get of the grog (ind) or Men's Shed
|
|
|
developing personal skills
(acc Ottawa Ch.) |
education for health and life skills so people can experience more control over their own health and their environment
|
|
|
|
re-orientate health services
(acc Ottawa Ch.) |
we must move increasingly in the health promotion direction, beyond its responsibility for providing clinical and curative services
|
|
|
|
DHS / Dep of Health response to Ottawa Charter
|

|
Health Promotion Interventions
|
|
|
how does DHS interventions relate back to Ottawa Ch.
|

|
|
|
|
stages for planning a health promotion program
|

|
|
|
|
needs assessment
(for creating a health promo plan) |
1. consult key stakeholders
2. awareness of on/off buttons (to get people involved in program) 3. collaborative process |
|
|
|
identify objectives
(for creating a health promo plan) |
1. what are the aims/goals
2. what data will be recorded & how (not just outcomes but also processes) 3. how will the program be evaluated/measured |
|
|
|
theory-based methods/strategies
(for creating a health promo plan) |
1. what framework/model informs the approach
2. often psych or social theories drawn on (i.e. behaviour change) |
|
|
|
program development
(for creating a health promo plan) |
1. who, what, where & when
2. let previous evidence/efforts guid current practice 3. draw on needs assessment results to inform development |
|
|
|
adoption & implementation
(for creating a health promo plan) |
1. how long will it run for
2. who will run it 3. how is it sustainable |
|
|
|
evaluation plan
(for creating a health promo plan) |
1. this is key - does the program work?
2. what will tell you if it did/didn't 3. qual & quant approach (mixed method) |
|
|
|
health promotion (def)
|
the process of enabling people to increase control over and to improve their health
|
|