![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
44 Cards in this Set
- Front
- Back
|
What arterial branch supply scaphoid ? |
Dorsal carpal branch of radial artery |
|
|
Why scaphoid fracture tend to get AVN ? |
Because the blood supply is from distal to proximal |
|
|
First sign of AVN is? |
Sclerosis |
|

Finding 2 Diagnosis Cut of value ? |
There is an intra-articular radial styloid fracture. Importantly, there is widening of the scapholunate distance (Terry Thomas sign) consistent with scapholunate dissociation. 3 mm |
|
|
What are the components of scapholunate ligament? Which band is the most important for stability? Associated deformity? |
3 parts Volar dorsal and middle Dorsal DISI deformity |
|
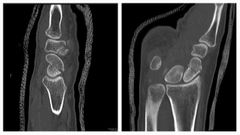
Finding Complications 2 |
Comminuted anteriorly impacted waist of scaphoid fracture producing a humpback deformity (seen on sagittal images).Scapholunate relationship is maintained. Non union DISI |
|
|
MRI signal of AVN T1 |
T1 dark |
|

Finding Diagnosis Risk factors? 2 |
Extensive arthropathic changes of the radioscaphoid joint evident by severe narrowing of its joint space and subarticular sclerotic bony change and remodelling involving the scaphoid bone. Scapholunate advanced collapse ( SLAC) Prior fractures CPPD disease affecting the scapholunate ligament |
|

Finding Diagnosis |
Frontal view:Osteoarthritis affecting the radial styloid and the scaphoid, with narrowing of the radioscaphoid joint space and associated subchondral sclerosis and cyst formation.Osteoarthritis with narowwing of the lunocapitate joint space (Snac stage III), due to proximal migration of the capitate.Ulnar translation of lunate.Lateral view:Dorsal tilt of the lunate with increased scapholunate angle.Features consistent with SNAC wrist stage III, with DISI. |
|

Finding Diagnosis Risk factor |
Widening of the SL angle with dorsiflextion of the lunate Angle > 60 ( normal 30-60) DISI ( dorsal intercalated segmental instability) Radial sided injury ( scapholunate ligament) |
|

Finding Diagnosis Risk factors |
The scapholunate angle is small < 30 VISI volar intercalated segmental instability Ulnar sided injury lunotriquetral ligament |
|
|
If you suspect scapholunate dissociation what is the best view to exaggerate it ? Chronic scapholunate dissociation result in? |

Clenched fist view SLAC deformity |
|

Finding Diagnosis Associated fractures? |

Lunate stays in its place Carpal bone around it moved
Perilunate dislocation
Scaphoid fracture 60% |
|

Finding Diagnosis What is injured |
Lunate is anteriorly dislocated Lunate dislocation Dorsal radiolunate ligament injury |
|

Finding Diagnosis Associated fracture? |
Both lunate and capitate lose radial alignment Mid carpal dislocation Lunotriquetral intra osseous ligament disruption Triquetral fracture |
|
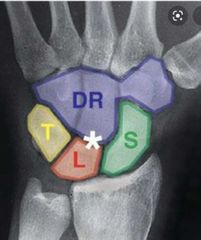
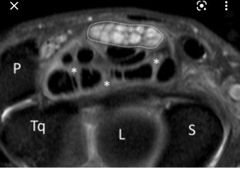
The space marked by astrix called? What it indicates? |
Space of Poirier Weakest point because it is ligament free |
|
|
What are the two synovial spaces communicate normally in the wrist ?
Clinical significance? |

Pisiform space and radiocarpal joint
Both spaces can be used in wrist arthrogram |
|
|
What are the other joint spaces that should not communicate ? 3 |
Glenohumeral joint and subacromial bursa ( full thickness tear of rotator cuff) Ankle joint and common personal tendon sheath ( tear if calcaneofibular ligament) Achilles tendon and posterior subtalar joint |
|
|
Function of TFCC? |
Triangular fibrocartilage complex TFCC Shock absorbable and stabiliser for the distal radio ulnar joint. |
|

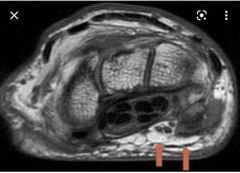
Finding Diagnosis |
MR arthrogram shows a full-thickness tear of the central portion of the TFC proper, with intact radial and ulnar attachments. Contrast is observed extending proximally into the distal radioulnar joint through this defect. The ulnar attachment of the TFC is intact, as are the distal attachments of the TFCC. There is a linear area of contrast extending through the lunotriquetral ligament indicating complete tear. There is a mild amount of oedema within the head of the ulna related to the trauma. Class 1 TFCC injury |
|
|
TFCC injury associated with ? |
Positive ulnar variance |
|
|
TFCC hold up by 3 ligaments? |
Volar and dorsal radio ulnar ligaments And Extensor capri ulnaris Ulnar collateral ligament |
|
|
In TFCC injury which side is likely to heal faster and why? |
Ulnar side as the blood supply comes from peripheral to centre Radial side will not heal properly |
|
|
Associated abnormalities with Positive ulnar variance Negative ulnar variance |
Positive TFCC injury ulnar impaction syndrome Negative AVN of lunate ( Keinbocks) |
|
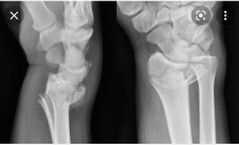
Name the fracture Associated fracture? |
Colles' fracture Ulnar styloid fracture |
|

Name fracture Associated fracture? |
Smith fracture Younger patient Ulnar styloid fracture |
|

Name the fracture |
Barton fracture Radial rim fracture Radiocarpal dislocation is hallmark Surgical correction |
|
|
How many extensor tendons for the wrist joint? What are the components of first compartment? |
6 1st Abductor pollices longus ( APL) Extensor pollices brevis ( EPB) |
|
Name structure Separate which 2 extensor compartment ? |
Lister's tubercle 2nd and third |
|
|
What is the first extensor compartment to get tenosynovitis in rheumatoid arthritis? |
6th compartment extensor carpi ulnaris |
|
|
Contents of carpal tunnel? 10 |
4 flexor digitorum profundus ( deep) 4 flexor digitorum superficialis 1 flexor pollicis longus Median nerve |
|
|
What are the structures not passing carpal tunnel? 4 |
Flexor carpi ulnaris, Flexor carpi radialis Flexor pollicis brevis Palmaris longus |
|
Finding Diagnosis US features Risk factors 4 |
Increased signal of median nerve Swollen with bowing of flexor retinaculum Carpal tunnel syndrome Thickened nerve Dialysis Pregnancy DM Hypothyroidism |
|
What anatomical structure is pointed out? |
Guyon's canal |
|
|
What are the boundaries for Guyon's canal ? What is guyon's canal syndrome? Caused by? |
Hook of hamate and pisiform Entrapment of ulnar nerve Handle bars |
|

Diagnosis |
Subsheath tear/ dislocation of extensor carpi ulnaris ( 6th compartment) |
|
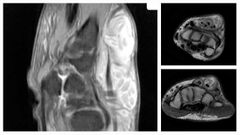
Finding Diagnosis 2 classical finding for this condition |
Marked synovial thickening is seen in the fourth and fifth extensor compartments with a large amount of fluid and multiple bodies within the tendon sheaths. The bodies are uniform in shape and show moderately high T2 and isointense T1 signal intensity. Enhancement of the thickened synovium is noted in the post-contrast images. Rice bodies , spares muscles Tuberculous tenosynovitis |
|
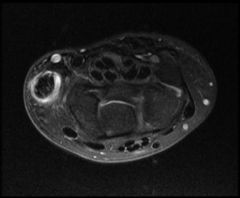
Finding Diagnosis Risk factors Indicator for good prognosis ? |
MRI reveals thickening of the first dorsal compartment tendons of the wrist (abductor pollicis longus and extensor pollicis brevis). There is increased fluid within the tendon sheath. Post-contrast, there is local enhancement. De Quervian's tenosynovitis first extensor compartment ( EPB and APL) Overuse New mom carrying baby Absent Intratendinous septum BTW EPB and APL |
|
|
Tenosynovitis of both extensor pollicis longus and brevis happened in ? |
Intersection syndrome ( first extensor compartment crosses second compartment) causing tenosynovitis |
|
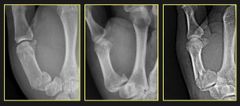
Name the fractures |

Rolando is comminuted Bennett is not |
|

Name the fracture ? Asscociated with ?2 |
Gameskeeper's thumb ( skier) Avulsion fracture of the proximal first phalanx Ulnar collateral ligament disruption Stener lesion |
|
|
What is stener lesion in gameskeeper's fracture? |
When the ulnar collateral ligament cought up by the adductor aponeurosis which delay the healing process |
|
|
Appearance of stener lesion in gameskeeper's fracture in MRI? |
Yo yo on string |
|
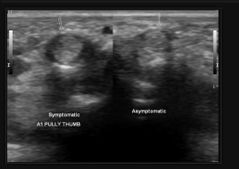
Finding Diagnosis Risk |
Thickened A1 pully Stenosing tenosynovitis ( trigger finger) Repetitive trauma and Scarring of flexor tendon |