Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
12 Cards in this Set
- Front
- Back
|
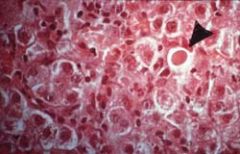
3. Liver: viral hepatitis with apoptosis The arrow points to an anucleate, deeply eosinophilic staining cell that is retracted away from the other cells. The last phase of destruction of this cell will be fragmentation into apoptotic bodies containing bound packets of organelles which will be phagocytosed and destroyed in the lysosomes of macrophages and neighboring cells. Note that there is no inflammatory infiltrate around the cell.
|
|

|
10. Brain: old artherosclerotic stroke with cystic cavity (liquefactive necrosis) Note the cystic cavities in the brain. Recall that infarction in the brain is not coagulative but liquefactive necrosis owing to the lack of good structure in the brain and the abundance of lysosomes in neuroglial cells.
|
|

|
12. Wrist: abscess due to Staphylococcus aureus (liquefactive necrosis) Note the raised, erythematous area on the wrist with a central area of draining from a sinus tract. Recall that S. aureus is a gram positive coccus that has coagulase. Coagulase converts fibrinogen into fibrin, which keeps the infection localized. This is an example of liquefactive necrosis.
|
|

|
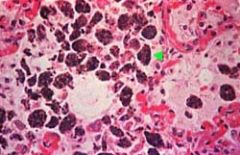
14. Lymph node: localized granuloma (caseous necrosis) in a patient with tuberculosis
Note the very well circumscribed eosinophilic staining granuloma. In the middle of the granuloma, the pink staining material is acellular. This represents caseous necrosis. Note the multinucleated giant cells at 2 and 7 o'clock. The following slide is a high power view of the granuloma. |
|
|
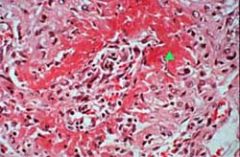
18. Arteriole: fibrinoid necrosis
Note the pink staining material in the wall of this arteriole (see arrow) that has been totally destroyed. This is an example of small vessel vasculitis, the majority of which are due to type III immunocomplex disease. Immunocomplexes deposit in the vessel and activate the alternative complement system, which releases C5a, a chemotactic agent that attracts neutrophils. The neutrophils destroy the vessel. The pink staining material represents protein from the plasma in the vessel lumen. Fibrinoid necrosis is the necrosis of immune disease and is seen in the vegetations associated with acute rheumatic fever and inflammation associated with many collagen vascular diseases. |
|
|
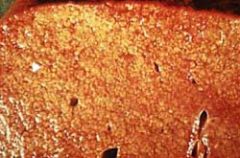
20. Liver: cirrhotic liver with fatty change
Note the diffuse nodularity of the liver and the yellowish discoloration representing fatty change. This patient was most likely an alcoholic, since alcohol is the most common cause of fatty change and cirrhosis of the liver. Refer to the class notes for the pathophysiology of fatty change. |
|
|
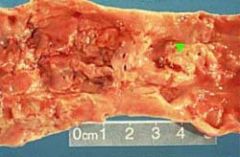
22. Aorta: aorta with complicated atheromatous plaques
Note the red clots, fissured endothelial surface, and raised plaque-like structures from the surface of the aorta (see arrow). This is an example of advanced atherosclerosis. This patient had an increase in low-density lipoprotein (LDL), the lipoprotein fraction that carries the majority of cholesterol. In the cardiovascular lectures, you will be introduced to the reaction to injury theory of atherosclerosis that is ultimately responsible for the changes noted in this slide. The fibrofatty plaques that normally occur with the reaction to injury on the aorta and muscular arteries are commonly calcified. Calcification of damaged tissue is called dystrophic calcification. Calcification significantly impairs the elasticity of the aorta, hence it cannot expand with blood during systole nor can it contract and help send the blood distally. |
|

|
35. Aortic valve: bicuspid aortic valve with dystrophic calcification leading to aortic stenosis
Note that the aortic valve has two rather than three cusps. This is a congenital bicuspid aortic valve. Since two cusps are doing the job of three cusps, they are damaged over time and develop dystrophic calcification (see arrow), which narrows the orifice of the valve leading to stenosis. Aortic stenosis results in problems with opening of the valve and the ejection of blood during systole. Left ventricular hypertrophy with concentric pathologic hypertrophy is a response to the valve stenosis. |
|
|
31. Lungs: chronic pulmonary congestion with hemosiderin laden alveolar macrophages
Note the rusty colored material in the alveolar macrophages. This patient had chronic pulmonary edema from left heart failure. The increased hydrostatic pressure in the pulmonary capillaries causes them to rupture, hence releasing RBCs into the alveoli. Alveolar macrophages phagocytose the RBCs and hemosiderin accumulates in the cytoplasm. In the setting of heart failure, these cells are called heart failure cells, which are frequently expectorated and produce a rusty colored sputum. |
|
|
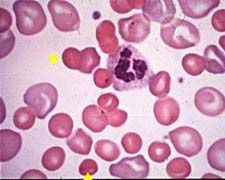
37. Peripheral blood smear: spherocytes
Note the dense RBCs without a central area of pallor (see arrow). Since normal RBCs are biconcave discs with a thin central region containing less hemoglobin than the thicker edges of the RBC, an RBC that is a sphere is completely filled with hemoglobin, hence the absence of a central area of pallor. Spherocytes have less RBC membrane than a normal RBC due to a defect in spectrin in the cell membrane. There are many causes of spherocytes in the peripheral blood besides congenital spherocytosis, such as autoimmune hemolytic anemia, ABO hemolytic disease of the newborn, to name a few. The blue staining RBCs in the peripheral blood represent young RBCs with residual RNA (reticulocytes). |
|
|
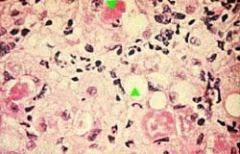
38. Liver biopsy: Mallory bodies in alcoholic hepatitis
Note the spaces in the liver biopsy representing fatty change (see arrow) and the pink staining material in the hepatocytes (see arrow) representing Mallory bodies. Mallory bodies represent damaged keratin intermediate filaments that have been "ubiquinated" by ubiquitin, hence marked for destruction. An acetaldehyde-protein complex is responsible for the damage. Mallory bodies are most commonly seen in the setting of an alcoholic with fever, neutrophilic leukocytosis, and painful hepatomegaly, the latter representing alcoholic hepatitis. |
|
|
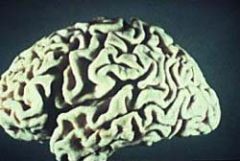
39. Brain: atrophy
Note the loss of brain mass, which causes separation of the gyri and sulci. This is most commonly caused by atherosclerosis of the internal carotid artery. Chronic tissue hypoxia causes the neurons in layers 3, 5, and 6 of the cerebral cortex to undergo apoptosis. Drop out of these neurons causes a loss in brain mass, which is evident in this slide. Other causes include degeneration of the neurons in Alzheimer's disease or destruction of neurons by infection. |