Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
164 Cards in this Set
- Front
- Back
|
Which class of antihypertensive is contraindicated in pts with advanced renal failure?
|
K+ sparing diuretics
if hyperkalemia - ACEI/ ARBs contraindicated |
|
|
What heart defect is assoc with Chr 22q11 deletion?
|
Truncus arteriosus
Tetrology of fallot |
|
|
What heart defect is assoc with Down Syndrome
|
Endocardial cushion defects (ASD, VSD, abnormal connection btw all 4 chambers)
|
|
|
What heart defect is assoc with Congenital rubella?
|
PDA
Pulmonary Artery Stenosis |
|
|
What heart defect is assoc with Turner's Syndrome?
|
Coarctation of aorta
|
|
|
What heart defect is assoc with Marfan's Syndrome?
|
Aortic insufficiency
|
|
|
What is the next step once a brain tumor has been identified on CT or MRI of the head?
|
(Step up pg 187)
need to realize most common source of tumor in the brain in adults is metastasis, so you need to look for the source of cancer: full body CT scan bone scan - mets may have gone to bones as well |
|
|
antidote to acetominophen?
|
n-acetylcysteine
|
|
|
antidote to lead?
|
Penicillamine
EDTA Dimercaprol Succimer |
|
|
antidote to Cyanide?
|
Thiosulfate
Hydroxycobalamin Nitrates |
|
|
antidote to Methemoglobin
|
Methylene blue
Vit C |
|
|
What are the indications for surgical parathyroidectomy?
|
- symptomatic
- serum Ca++ conc >1.0 above the upper limit of normal - Creatinine clearance reduced by 30% - bone mineral density T-score < -2.5 at any site - younger than 50 yrs of age |
|
|
What are the diagnostic features of a peritonsillar abscess?
|

- Infxn btw the tonsil & pharyngeal constrictors by Strep pyogenes, staph aureus and/or Bacteroides
- severe sore throat, fever, muffled "hot potato" voice - classic diagnostic feature is obvious abscess on the tonsil or deflection of the uvula to the opposite site - other signs and symptoms include trismus ("lockjaw") and drooling |
|

What is the tx for peritonsillar abscess?
|
- needle aspiration or I&D
- Pain meds + ABX: Augmentin 875mg PO BID x10days or Clindamycin 300mg or 450mg PO q6hrs x10days |
|
|
What is a normal range for the A-a gradient?
|
5-15mmHg
|
|
|
Deviated uvula - trouble opening mouth - muffled "hot potatoe" voice
Dx? |
Peritonsillar abscess
|
|
|
What is a helpful symptom to differentiate a common cold from the flu?
|
myalgias (muscle aches) are common in flu but not in colds
|
|
|
What are the diagnostic features of acute bacterial sinusitis that distinguish it from the common cold?
|

Rhinosinusitis symptoms lasting seven or more days and any of the following:
- purulent nasal discharge - maxillary tooth or facial pain (esp unilateral) - unilateral maxillary sinus tenderness - worsening symptoms after initial improvement Radiologic tests are of little value b/c they cannot distinguish acute viral sinusitis from acute bacterial sinusitis, but CT of the sinuses can rule out sinusitis if another etiology of the symptoms is being considered |
|
|
What is the treatment for ACUTE bacterial sinusitis?
|
- Observation and symptom relief alone in otherwise healthy pts with mild pain and temp <101F
---nasal saline irrigation ---analgesics ---topical decongestant (ie Afrin) or systemic decongestant (ie Sudafed) - Antibiotics: --- First line: Amoxicillin 1g TID x10-14days >Augmentin 875 BID x10-14days --- Second line: Cephalosporins (omnicef 300mg BID x10days) > Fluoroquinolones (Levaquin 750mg qd x5days, or moxifloxacin 400mg qd x5days) or Bactrium > Macrolides (ZIthromax 500mg qd x3days) +/- Intranasal glucocorticoids - may reduce inflammation and symptoms, but studies lacking |
|
|
What is the treatment for CHRONIC (>3mos of symptoms) bacterial sinusitis?
|
Combined therapy:
- Oral steroids (ie Prednisone 20mg BID x5days -- then qd x5days) - Oral Antibiotics for 3-6wks (Augmentin or clindamycin) - Intranasal saline irrigation - Intranasal steroids indefinitely - if underlying allergies -- antihistamines, antileukotrienes (ie Singulair) and/or allergen immunotherapy - if nasal polyps refractory to steroids -- surgical debulking - if allergic fungal sinusitis -- sinus surgery -- prolonged course of steroids |
|
|
What are the potential complications of sinusitis?
|
meningitis
abscess orbital infection osteomyelitis |
|
|
What is the classic presentation of allergic fungal rhinosinusitis? How is the diagnosis made?
|
- chronic rhinosinusitis
- in this disase the sinuses are opacified with thick "alelrgic mucin" that is colonized with fungus (not to be confused with invasive fungal disease) - the diagnosis is made at the time of surgery when the "allergic mucin" is identified |
|
|
What antibiotics would you use to treat pneumonia in a NEWBORN?
What are the most common bugs in this age group you are trying to kill? |
Ampicillin & Gentamicin
+/- Vancomycin (if MRSA is a concern) (use Erythromycin for Chlamydia) Bugs: GBS > Gram negs (E coli) Listeria Chlamydia trachomatis |
|
|
What antibiotics would you use to treat pneumonia in a 1-4mo?
What are the most common bugs in this age group you are trying to kill? |
Macrolides (azithromycin, erythromycin, clarithromycin)
+/- cefotaxime RSV, Chlamydia trachomatis, Parainfluenza, Bordatella, Strep pneumo, Staph aureus |
|
|
What antibiotics would you use to treat pneumonia in a 4mo-4yo?
What are the most common bugs in this age group you are trying to kill? |
Amoxicillin or Ampicillin (oral)
RSV or other virus, Strep pneumo, H flu, mycoplasma, staph aureus |
|
|
What antibiotics would you use to treat pneumonia in a 5-15yo?
What are the most common bugs in this age group you are trying to kill? |
1) Amoxicillin + clarithromycin (or erythromycin)
2) Azithromycin 3) Amoxicillin + doxycycline Strep pneumo > Mycoplasma, C. pneumonia, other viruses (rhino, influenza, adenovirus, coronavirus) |
|
|
What are the indications for the pneumococcal vaccination in adults?
|
- 65 yrs or older
- serious long-term health problem such as heart disease, sickle cell disease, alcoholism, leaks of CSF, lung disease (not including asthma), diabetes or liver cirrhosis - resistance to infxn is lowered due to Hodgkin's disease, multiple myeloma, cancer treatment with Xrays or drugs; treatment with longterm steroids; bone marrow or organ transplant; kidney failure; HIV/AIDS, lymphoma/ leukemia or other cancers, nephrotic syndrome, damaged spleen or no spleen - Cigarette smokers btw the age of 19-64 |
|
|
What antibiotics can be used in the treatment of Pseudomonas pneumonia?
|
An antipseudomonal beta-lactam (piperacillin-tazobactam (zosyn) cefepime, imipenem, meropenem, aztreonam) must be added to one of the following for at least 2 weeks for adequate coverage:
- Antipseudomonal quinolone (ciprofloxacin, or levofloxacin 750mg) - Aminoglycoside (tobramycin, gentamicin, or amikacin) + azithromycin - Aminoglycoside (tobramycin, gentamicin, or amikacin) + antipseudomonal quinolone |
|
|
A surgical pt has had a NG tube in place for 2wks due to gastroparesis. He has had a persistent fever and elevated WBC ct w/o an identified source. UA, cultures, and CXRs are negative and the wound is healing well w/o signs of infection. He has no abdominal pain or symptoms to indicate intra-abdominal catastrophe. What study might reveal the source of this fever?
|
CT of head and face (to show sinusitis)
|
|
|
What are the classical findings in atypical pneumonia?
|
diffuse interstitial infiltrates
|
|
|
What organism is associated with atypical pneumonia in young adults?
|
mycoplasma pneumonia
|
|
|
What organism is associated with atypical pneumonia in the elderly and very young?
|
chlamydia pneumonia
|
|
|
What organism is most common pneumonia in children (infant to 5yrs old)
|
RSV
|
|
|
What organism is the most common cause of pneumonia in neonates?
|
Group B Strep (GBS)
|
|
|
A hospital has multiple admissions of elderly pts presenting with atypical pneumonia. All were present at the grand reopening of an old bingo establishment that has an indoor waterfall. what is the likely causal organism?
|
Legionella
|
|
|
What is the treatment for atypical pneumonia?
|
Macrolide (erythromycin, azithromycin, clarithromycin)
|
|
|
What is the typical time frame after which acute bacterial sinusitis is the cause of purulent nasal discharge?
|
more than 7 days
|
|
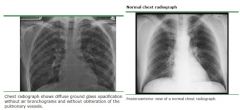
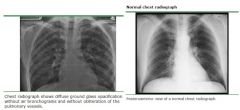
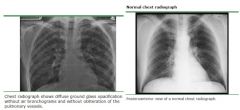
Whats the dx?
CXR shows diffuse, bilateral, interstitial infiltrates in an AIDs pt with CD4 ct < 200 What other lab value would you expect? |
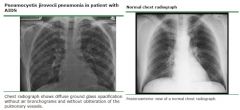
Dx: PCP pneumonia
Lab: LDH level usually >220 (and a rising LDH despite appropriate treatment portends a poor prognosis) |
|
What is the tx for for PCP?
|
21 days of antibiotics - Choices include:
TMP-SMX (Bactrim) - IV or PO Pentamidine (Nebupent) - IV Primaquine (PO) + Clindamycin (IV or PO) If moderate-severe disease (PaO2 <70mmHg, or A-a gradient >35): - hospitalize + prednisone 40mg PO BIDx5days then 40mg qd x5days then 20mg PO qd x11 days |
|

What is the differential diagnosis (short list) for ground-glass opacities (diffuse hazy infiltrate) of the lung on CXR?
|
- interstitial pneumonia
- PCP pneumonia - Pulmonary edema - Pulmonary Hemorrhage - Hypersensitivity pneumonitis |
|
|
mcc of pneumonia in immunocompromised
|
PCP
|
|
|
common causative agent for pneumonia in alcoholics
|
klebsiella
|
|
|
can cause an interstitial pneumonia in bird handlers
|
chlamydia ptisacci
|
|
|
often the cause of pneumonia in a pt with h/o exposure to bats or bird droppings
|
histoplasma
|
|
|
often the cause of pneumonia in a pt who has recently visited south carolina, new mexico, or west texas
|
cocciodiodes
|
|
|
pneumonia assoc with "currant jelly" sputum
|
klebsiella
|
|
|
infectious agent causing Q fever
|
Coxiella burnetti
|
|
|
pneumonia acquired from air conditioners
|
Legionella
|
|
|
Mcc of pneumonia in children 1yo or younger
|
RSV
|
|
|
mcc of pneumonia in the neonate (Birth-28days)
|
GBS & E. coli
|
|
|
mcc of pneumonia in children and young adults (including college students, military recruits, and prison inmates)
|
mycoplasma pneumonia
|
|
|
common cause of pneumonia in pts with other heatlh problems
|
Klebsiella
|
|
|
Mcc of viral pneumonia
|
RSV & influenza
|
|
|
Causes a woolsorter's disease (a life-threatening pneumonia)
|
Bacillus anthracis
|
|
|
Common bacterial cause of COPD exacerbation
|
H. influenza
|
|
|
Common pneumonia in venilator pts and those with cystic fibrosis (CF)
|
Pseudomonas
|
|
|
Pontiac fever (similar to the flu)
|
Legionella
|
|
|
Which bug causes pneumonia and gram stain shows:
Gram + cocci in clusters |
staph aureus
|
|
|
Which bug causes pneumonia and gram stain shows:
Gram + cocci in pairs |
streptococcus pneumonia
|
|
|
Which bug causes pneumonia and gram stain shows:
gram neg rods in 80yr olds |
E coli
|
|
|
Which bug causes pneumonia and gram stain shows:
gram + cocci in neonate |
GBS
|
|
|
Which bug causes pneumonia and gram stain shows:
Gram neg rods in neonate |
E. coli
|
|
|
How is the dx of active TB made?
|
TB organisms seen in any of the following is sufficient to make the dx:
- sputum acid-fast stain - if seen in any of the 3 samples ideally obtained qd over 3 days in early AM - Sputum culture for TB (takes 1-8 wks depending on the media used) - Bronchoscopy with bronchoaveolar lavage (BAL) or biopsy |
|

- bilateral pulmonary infiltrates on imaging consistent with pulmonary edema
- acute onset of respiratory distress - no evidence of cardiac origin - PaO2/ FiO2 <200mmHg Dx? |
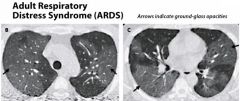
Acute Respiratory Distress Syndrome (ARDS)
|
|

What treatments are available when managing a pt with Acute Respiratory Distress Syndrome (ARDS)?
|
(1) treat underlying disease & provide supportive care in the ICU
(2) mechanical ventilation with low tidal volumes (to minimize injury) and adequate PEEP (to recruit collapsed alveoli) - Conservative fluid management to reduce pulmonary edema - Goal CVP 4-6 H2) (Furosemide and albumin may also be helpful to prevent pulmonary edema) - Prone positioning improves oxygenation but does not improve survival - Minimize oxygen consumption by preventing fever (anti-pyretics), minimizing anxiety and pain (sedative and analgesics) and limiting respiratory muscle use (paralytics) particularly in cases of asynchrony of the ventilator and pt's efforts - transfuse blood only if Hgb drops below 7 g/dL as transfusion may increase risk of death in ARDS pts |
|
|
A friend tells you that he was hospitalized for fungal pneumonia after a trip to the deserts of New Mexico. What medication did he most likely receive in the hospital to treat his pneumonia?
|
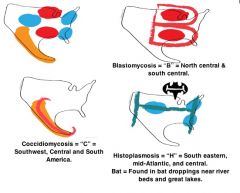
Amophotericin B (for coccidiomycosis)
|
|
|
What is the treatment for histoplasmosis & bastomycis?
|
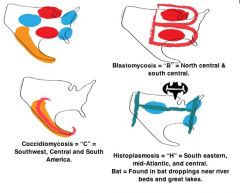
Itraconazole
|
|
|
In what situations is an induration of 5mm during a PPD screening considered a positive test?
|
HIV
close contacts with TB CXR signs of TB |
|
|
In what situations is an induration of 10mm during a PPD screening considered a positive test?
|
Homeless
immigrants from endemic areas IV drug users chronically ill health workers recently incarcerated |
|
|
In what situations is an induration of 15mm during a PPD screening considered a positive test?
|
Low risk populations
|
|
|
Why is pyridoxine (vit B6) given to pts on RIPE therapy?
|
to prevent or attenuate the peripheral neuropathy caused by isonizid
|
|
|
How might someone that received the BCG vaccine have a negative PPD test?
|
they could have had the BCG vaccine before 1 yr of age or if 10 yrs have passed since they received the vaccination
|
|
|
You notice someone's PPD test converts from negative to positive, could this be a result of the BCG vaccine?
|
yes, if the vaccine was given LESS THAN 1 MONTH ago
(takes 1 month after you get the BCG vaccine for a positive PPD test, and will have a positive test up to about 10 yrs post-vaccination) |
|
|
What is the PaO2:FiO2 ratio in ARDS?
|
normal = 300-500 mmHg
ARDS = <200mmHg during mechanical ventilation gas exchange deficit: <300 |
|
|
Which method of O2 delivery can be used to give the patient the most O2 without putting them on a ventilator?
|
non-rebreather mask can give up to 95% FiO2
|
|
|
In a pt with pulmonary edema, how can pulmonary wedge pressure (PCWP) distinguish ARDS from cardiogenic shock?
|
if PCWP <12 = noncardiogenic pulmonary edema (usually ARDS)
If PWCP >18 = cardiogenic edema (heart failure) (note: Swan-Ganz catheters are not proven to improve outcomes in ARDS) |
|
|
What are the diagnostic characteristics of Acute Respiratory Distress Syndrome (ARDS)?
|
- acute onset respiratory distress
- no evidence of cardiac origin - PaO2/FiO2 <200mmHg - bilateral pulmonary infiltrates on imaging consistent with pulmonary edema |
|
|
What is the differential diagnosis of ground-glass infiltrates on CXR?
|
Interstitial pneumonia
PCP pneumonia Pulmonary edema or ARDS Pulmonary Hemorrhage Hypersensitivity Pneumonitis |
|
|
What is a normal A-a gradient? What causes a high A-a gradient?
|
normal = 5-15 mmHg
High A-a gradient: PE, pulmonary edema or ARDS, Right to Left shunt |
|
|
What is the empiric treatment for pneumonia in a 2mo old? In a 2yr old?
|
2 month old: macrolide (erythromycin, clarithromycin, azithromycin)
2 yr old: amoxicillin or ampicillin |
|
|
How is asthma managed using different symptom based categories?
(draw the dreaded chart!!) |

|
|
|
How is COPD managed based on stage of the disease?
|

|
|
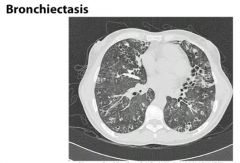
What are the possible etiologies for bronchiectasis?
|
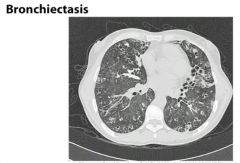
Unknown etiology in 50% of pts
Cystic fibrosis Immunodeficiency Dyskinetic cilia: Kartagener’s syndrome (dextrocardia, sinusitis, bronchiectasis), Aut Dom polycystic kidney dz Pulmonary infections (TB, fungal, or lung abscess) Obstruction (ie foreign body aspiration, tumor, lymph nodes) Other etiologies: Young’s syndrome, foreign body aspiration, rheumatoid arthritis, Sjogren’s Syndrome, allergic bronchopulmonary aspergillosis, cigarette smoking |
|
|
What does an asthma pt who has asthma attacks about 4x/week need for her medication regimen?
|
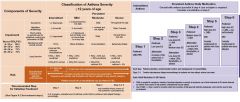
Dx: mild persistent asthma
Tx: Albuterol + low dose steroid +/- Singulair (Montelukast) +/- Cromolyn |
|
|
What is the most effective tx for COPD?
|
Stop smoking!
|
|
|
At what pt do pts with COPD qualify for home O2?
|
Pulse oximetry < 88%
|
|
|
What treatment is proven to ↓ M&M in COPD pt?
|
Supplemental Oxygen
|
|
|
What are the requirements to diagnose chronic bronchitis?
|
Productive cough >3mos over 2 yrs
|
|
|
The mc form of emphysema has what kind of distribution?
|
Centrilobar
|
|
|
What is the hallmark sign of COPD?
|
↓ FEV1: FVC ratio
|
|
|
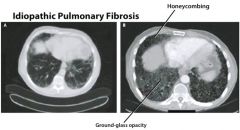
How is interstitial fibrosis diagnosed?
|
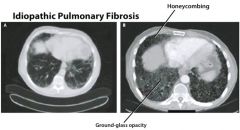
CXR possible findings → normal in 10%, reticular pattern, nodular pattern, or honeycomb lung (poor prognosis)
High resolution CT scan – greater diagnostic accuracy than plain films Serum markers including SP-A, SP-B, MCP-1, KL-6 Pulmonary function testing (PFTs) reveal restrictive lung disease with ↓ TLC, FRC, and RV Lung biopsy is required to make the definitive diagnosis & determine the stage of disease |
|
|
Which lung cancers are more common in smokers, and where are they found?
|
Small cell & squamous cell → Found centrally
|
|
|
A 60yo smoker presents with the c/o paresthesias and pain in the left upper extremity. On exam he has left eyelid drooping and miosis, which he says are new. What is the name of the syndrome? What is the disease?
|
Dx: Pancoast Syndrome, due to lung tumor
|
|
|
How might a pt w/ superior vena cava syndrome present? Tx?
|
S/S: head swelling/ plethora, headache, vision changes, AMS
Tx: Steroids & endovascular stent |
|
|
HYQ: What is the initial tx for small cell lung cancer?
|
Chemotherapy
|
|
|
What is the classic symptom of laryngeal cancer?
|
Hoarseness that worsens over time
|
|
|
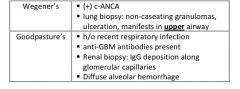
Wegener’s granulomatosis & Goodpasture’s syndrome can have similar presentations with hemoptysis, dyspnea & hematuria. What are some key differences to help distinguish the two?
|
|
|
|
What findings make a solitary pulmonary nodule more likely to be malignant?
|
Smoker
> 45yrs New/progressive lesion No calcifications Irregular calcifications > 2cm Irregular margins |
|
|
HYQ: What is the next step in the work-up of a pt with a solitary pulmonary nodule?
|
Compare to previous xray
|
|
|
Which type of lung cancer is a/w the following syndrome?
Elevated ACTH → glucocorticoid excess → Cushing’s Syndrome |
Small Cell
|
|
|
Which type of lung cancer is a/w the following syndrome?
Elevated PTH related peptide → hypercalcemia |
Squamous Cell
|
|
|
Which type of lung cancer is a/w the following syndrome?
Elevated ADH → SIADH → hyponatremia |
Small Cell
|
|
|
Which type of lung cancer is a/w the following syndrome?
Antibodies to presynaptic Ca2+ Channels → Lambert-Eaton Syndrome |
Small cell
|
|
|
HYQ: What is the initial tx of a localized non-small cell lung ca?
|
Surgical resection
|
|
|
What are the classic radiological findings in idiopathic pulmonary fibrosis?
|
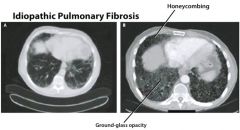
Reticular / honeycomb pattern on CXR
|
|
|
What is the tx for idiopathic pulmonary fibrosis?
|
Steroids, azathioprine or cyclophosphamide, Nacetylcysteine
|
|
|
Which type of pneumonoconiosis matches the following?
Progressive fibrosis |
Silicosis &
Coal Workers disease |
|
|
Which type of pneumonoconiosis matches the following?
↑ risk of TB |
Silicosis
|
|
|
Which type of pneumonoconiosis matches the following?
a/w working with electronics → ↑ cancer risk |
Berylliosis
|
|
|
Which type of pneumonoconiosis matches the following?
Malignant mesothelioma & bronchogenic carcinoma |
Abestosis
|
|
|
Pt with chronic sinusitis + hemoptysis + hematuria → tx?
|

Dx: Wegener’s Granulomatosis
Tx: steroids & cyclophosphamide |
|
|
Pt with anti-glomerular basement membrane Abs → tx?
|
Dx: Goodpasture’s Syndrome
Tx: Plamapheresis, steroids, possibly immunosuppressants |
|
|
A smoker has rapid onset JVD, facial swelling, and altered mental status → tx?
|
Dx: Superior vena cava syndrome
Tx: steroids, endovascular stent |
|
|
A pt chronically has an FEV1 of 40%. What meds are used in the daily management?
|

Dx: COPD
TX: inhaled steroids, long acting bronchodilatory, PRN short acting bronchodilator, risk factor reduction, Flu & pneumococcal vaccine |
|
|
What studies are helpful in dx of pulmonary embolism (PE)?
|

|
|
|
Vasodilators used in Pulmonary Hypertension:
|
Prostanoids – epoprostenol, treprostinil, iloprost
Endothelin receptor antagonists – bosentan, ambrisentan Cyclic GMP phosphodiesterase inhibitors: sildenafil (Viagra) CCB – nifedipine (Procardia) |
|
|
What imaging studies are most helpful in diagnosing a PE?
|
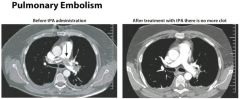
Spiral CT with IV contrast
V/Q Perfusion Scan Pulmonary Angiography |
|
|
What is a classic sign of PE on CXR?
|
Hamptom’s Hump
|
|
|
What is the next step in the management of a pt that you suspect has pulmonary HTN b/c of his symptoms of JVD< loud S2, dyspnea, and fatigue?
|
Echocardiogram
|
|
|
What is the primary drug category used to tx pulmonary HTN?
|
Vasodilators: Prostanoids, endothelin receptor antagonists, GMP phophodiesterase inhibitors, Dihydropyridine CCBs
|
|
|
A lung cancer pt is re-admitted to the hospital for dyspnea. He is found to have re-accumulation of his pleural effusion. What do you expect the pleural-to-serum protein & LDH ratios from the thoracentesis to be? What do you expect the pleural fluid protein content to be?
|
Exudate (malignancy) → high protein, high LDH
Pleur: Ser protein > 0.5 Pleur: Ser LDH > 0.6 Pleural fluid protein > 3g/dL |
|
|
• A trauma pt involved in MVC has a R-sided fluid collection evident on CXR. An emergent chest tube is places and thick pink fluid evacuates. What is the pink fluid? What structure is likely damaged in this pt?
|

What is it: Chylohemothorax (pink = mixture of blood & lymph, chyle in lymphatic fluid = white)
Thoracic duct is damaged |
|
|
What study can help you determine whether pleural effusion is loculated or free-flowing in the thorax?
|
Upright CXR, Lateral decubitus CXR
If you see that fluid mass moves → free flowing |
|
|
What are the CXR findings of a pneumothorax?
|

|
|
|
What are the components of rapid sequence intubation?
|

|
|
|
What anatomic locations are options for immediate needle decompression of a tension pneumothorax (PTX)?
|
Midclavicular line – 2nd or 3rd ICS
Midaxillary line – 4th or 5th ICS |
|
|
How is a small pneumothorax treated?
|
Supplemental O2 & observation
|
|
|
What are important symptoms in tension pneumothorax?
|
Dyspnea, tachycardia, unilateral ↓ in breath sounds
↑ resonance to percussion, tracheal deviation |
|
|
How do you treat a large hemothorax, chylothorax, pneumothorax (>15%) or pleural effusion?
|
Place a chest tube
|
|
|
An obese middle-aged man comes to your clinic with the complaint of fatigue. He reports that he falls asleep in the middle of conversations with his wife and children. What condition does he likely have, and what options are available to help him?
|
Dx: obstructive sleep apnea
Tx: weight loss, CPAP, Jaw positioning devices, surgery of upper airway |
|
|
A pt is intubated & a color change end tidal CO2 indicates that CO2 is indeed coming out with expirations. However, only the right lung sounds are audible. What is the problem?
|
Intubation of right mainstem bronchus
|
|
|
A tall, thin, young male develops an abrupt onset of SOB and R-sided chest pain. What CXR findings would indicate a pneumothorax int his pt?
|
Lung retraction
Mediastinal shift from the affected side |
|
|
What are the classic signs & symptoms of Croup?
|

|
|
|
What is the treatment for croup? What are the indications for hospitalization?
|

|
|
|
What are the characteristic features of epiglottits?
|

|
|
|
What is the treatment for epiglottitis?
|

|
|
|
What is the classic presentation of RSV bronchiolitis?
|
Starts with 1-3 days of mild URI symptoms: rhinorrhea, mild cough, and mild fever +/- otitits media
Cough with prlonged expiration, expiratory wheezing, crackles, and hyperresonance on percussion Possible respiratory distress with nasal flaring, tachypnea, retractions, grunting Possible apnea in infants (indication for mech ventilation) Complete resolution usually takes one month |
|
|
What is the treatment for RSV bronchiolitis?
|

|
|
|
How is the lecithin/sphingomyelin (L:S) ratio used in determining fetal lung maturity?
|

|
|
|
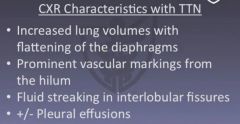
What CXR characteristics distinguish neonatal respiratory distress syndrome from transient tachypnea of the newborn?
|
RDS – low lung volumes, diffuse ground glass appearance with air bronchograms
TTN – ↑ lung volumes with flattening of the diaphragms, prominent vascular markings from the hilum (sunburst pattern) fluid streaking in interlobular fissures, +/- pleural effusions |
|
|
What is the treatment for neonatal respiratory distress syndrome?
|
Surfactant administration (from porcine or bovine source)
Continuous positive airway pressure (CPAP) or intubation and mechanical ventilation CPAP is preferred in larger babies (>1500g) or if active, breathing spontaneously, and not in resp failure Mechanical ventilation if respiratory failure |
|
|
How is cystic fibrosis diagnosed?
|
Sweat chloride test: sweat chloride conc > 60mEq/L on 2 or more occasions
Performed by a lab familiar with the test Considered the gold standard for dx of CF Genetic testing for CFTR gene mutations: identifies about 90% of cases Nasal transepithelial chloride secretion: measures abnormalities in ion transport across the nasal epithelium |
|
|
What are the general strategies for managing the GI component of cystic fibrosis?
|
Pancreatic enzyme replacement during meals
Fat soluble vitamin replacement |
|
|
What is the most common cause of Croup?
|
Parainfluenza virus
|
|
|
Croup can be diagnosed by remembering the “4 S’s” :
|
Seal-bark cough
Stridor Subglottic narrowing Steeple sign on xray |
|
|
What radiologic sign do you look for with epiglottis?
|
Thumb print sign
|
|
|
What organism is responsible for epiglottitis?
|
Haemophilus Influenza type B
|
|
|
What is extremely important to remember before examining a child suspected of having epiglottits?
|
Make sure you are in a setting in which you are capable of intubating rapidly
|
|
|
What is a typical presentation of bronchiolitis?
|
< 2yrs old
tachypneic, rhinorrhea, nasal congestion, fever, costal retractions, grunting, +/- nasal flaring |
|
|
When is maternal administration of corticosteroids indicated in the case of preterm delivery?
|
Give before the initiation of labor
Always give if < 34wks gestation Lecithin: sphingomyeline ratio < 2.0 Phosphatidylglycerol is absent |
|
|
What tests are available to confirm the dx of cystic fibrosis?
|
Sweat chloride test > 60 mEq
Genetic testing for CFTR gene Nasal transepithelial chloride secretion test |
|
|
HYQ: What substances should be avoided in pts with obstructive sleep apnea?
|
Sedatives at bedtime – Benzos, alcohol, antihistamines
|
|
|
HYW: Shortly after birth a child has stridor, wheezing, and SOB despite medical therapies. What is likely to be causing this pt’s symptoms?
|
Vascular ring
|
|
|
What are the general strategies for treating the pulmonary component of cystic fibrosis?
|
β-2 agonists, DNAse 1, hypertonic saline, chest physiotherapy, liberal PRN antibiotics
|
|
|
What is the treatment for epiglottitis?
|
Minimize anxiety, IV antibiotics, intubation
|
|
|
What is the treatment for Croup?
|
O2, steroids, racemic epinephrine
|
|
|
What is the treatment for RSV bronchiolitis?
|
O2, albuterol or racemic epinephrine
|
|
|
HYQ: Trauma pt in respiratory distress → CXR shows pleural effusion → what is the next step in the management of this pt?
|
Dx: assume hemothorax
Tx: place a chest tube |
|
|
What might cause a transudative pleural effusion?
|
CHF, cirrhosis, nephrotic syndrome
|
|
|
What size pneumothorax requires chest tube placement?
|
Pneumothorax > 15%
|
|
|
What medication is used prior to intubation in head injury pts?
|
Lidocaine
|
|
|
What is classic (but rare) EKG finding in pulmonary embolism?
|
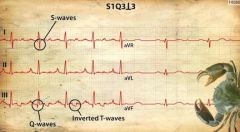
S1Q3T3 (wide S in lead I, Large Q & inverted T in lead III)
|
|
|
What is the typical CXR appearance of newborn respiratory distress syndrome?
|
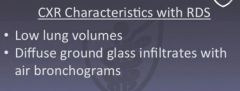
Low lung volumes
Diffuse ground glass appearance Air bronchograms |
|
|
What is the typical CXR appearance of newborn with transient tachypnea?
|
see above
|