![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
36 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
GFR? |
The glomerular filtration rate (GFR) is the rate at which |
|
|
|
rel to body size? |
It is proportionate to body size |
|
|
|
ref range
|
and the reference range is usually expressed after correction for body surface area as 120 ± 25 mL/min/1.73m2
|
120 ± 25 mL/min/1.73m2
|
|
|
Direct meas |
The GFR may be measured directly by |
|
|
|
when dir? |
However, this is not performed |
|
|
|
Clinical prc |
Instead, GFR is usually |
|
|
|
widely used comp |
The most widely used |
|
|
|
Signif |
Although creatinine is |
|
|
|
creatinine and GFR |
Accordingly, provided muscle mass remains constant, changes in serum |
|
|
|
measurement |
Several methods have been |
|
|
|
widely used eq |
but the most |
|
|
|
Signi of eGFR |
Although the eGFR has several limitations (Box 17.2), its |
|
|
|
Assessment |
A potentially more accurate assessment of GFR can |
|
|
|
17.1 How to estimate glomerular filtration |
01. Measuring GFR 02. Estimating with equations |
|
|
|
Measuring GFR |
• Direct measurement |
|
|
|
Direct Meas |
using labelled EDTA or inulin |
|
|
|
Creatinine clearance (CrCl |
Minor tubular secretion of creatinine causes CrCl to |
|
|
|
drugs aff crCl |
(e.g. trimethoprim, cimetidine |
|
|
|
CrCl mL/min = |

|
|
|
|
mg/dl to umol/L |
To convert |
|
|
|
02. Estimating with Equations |
• Cockcroft and Gault equation • The Modification of Diet in Renal Disease (MDRD) study |
|
|
|
• Cockcroft and Gault equation |
Reasonably accurate at normal to moderately impaired |
Advantages |
|
|
Equation |
|
|
|
|
• The Modification of Diet in Renal Disease (MDRD) study |
Performs better than Cockcroft and Gault at low GFR |
Benefits |
|
|
Equation |

|
*A correction factor, either a value recommended by the laboratory/assay |
|
|
Limitations of eq |
• No equations perform well in unusual circumstances, such as |
|
|
|
Limitations |
01. Extremes of wt 02. Confidence Intervals 03. Changes Signicance 04. Value in AKI 05. Racial Groups 06. Special Population 07. Elderly 08. Normal func underestimation |
|
|
|
01. Extremes of wt |
• It is only an estimate, least reliable at extremes of body |
|
|
|
02. Confidence Intervals |
• Confidence intervals are wide (90% of patients will have |
|
|
|
03. Changes Signicance |
• Values are consistent in individuals, so changes mean more |
|
|
|
04. Value in AKI |
• Creatinine level must be stable over days; eGFR is not valid |
|
|
|
08. Normal func underestimation |
• It tends to underestimate normal or near-normal function, so |
|
|
|
07. Elderly |
• In the elderly, who constitute the majority of those with low |
|
|
|
05. Racial Groups |
• The equation was originally validated in US patients and |
|
|
|
06. Special Population |
• eGFR is not valid in under-18s or during pregnancy |
|
|
|
Serum cr rel to GFR |
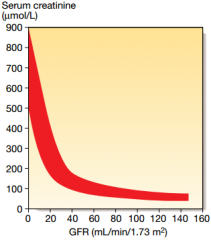
|
Fig. 17.2 Serum creatinine and the glomerular filtration rate |