![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
112 Cards in this Set
- Front
- Back
|
GERD stands for? |
- gastro-esophageal reflux disease |
|
|
What happens in GERD? |
Lower esophageal sphincter is incompetence → allow reflux (backflow) of gastric contents into esophagus → causing burning pain |
|
|
What causes GERD? |
Primary: - ↓ tonus of lower esophageal sphincter Others: - ↓ esophageal motility - pyloric stenosis - hiatal hernia Dietary Factors: - coffee - fatty food - alcohol, tobacco |
|
|
GERD patients usually come with? (symptoms) |
MAINLY: - burning pain (heart burn) - dyspepsia - waterbrash (sudden flow of saliva) Also: - coughing - hoarseness, sore throat - nausea, vomit |
|
|
How burning pain in GERD looks like? |
Retrosternal / epigastric pain: - pain radiates along esophagus (area of sternum) - burning sensation shortly after eating - worsened by lying down * may mimic cardiac chest pain |
|
|
Mnemonic for symptoms in GERD? (L A W D O H) |
L - long standing GERD A - anemia W - weight lost D - dysphagia O - odynophagia H - heme stool (melena) |
|
|
Mnemonic for symptoms in GERD? (ALARM symptoms) |
A - anemia L - loss of weight A - anorexia R - recent onset of progressive sx M - melena |
|
|
How can we do to confirm GERD? (diagnosis) |
1. Endoscopy (with biopsies) - to see if present of dysplasia TRO Barrett's esophagus 2. Barium contrast study - TRO strictures / ulceration 3. 24h pH monitor in lower esophagus - for pt. with typical sx BUT normal endoscopy - to confirm any reflux of gastric content 4. Esophageal manometry - to evaluate esophageal peristalsis - TRO dysphagia / motility disorder |
|
|
GERD can cause complications, depends on? |
- what is the nature of reflux (acidic / less)? - is it possible to clear the reflux? - volume of reflux? - how is the local mucosal protective function? |
|
|
Complications of GERD? |
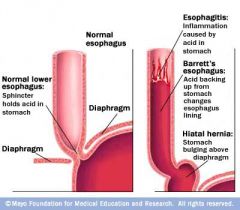
1. Erosive esophagitis - may cause occult bleeding / odynophagia 2. Peptic stricture - ? - fibrotic rings → narrowing esophageal lumen 3. Esophageal ulcer - may cause upper GI bleeding - pain similar to gastric / duodenal ulcer - heal slowly → may have scar 4. Anemia 5. Barrett's esophagus - metaplasia of str. sq. epi → columnar gastric epi. (histology) - ↑ risk of adenoma |
|
|
How to treat peptic stricture complication? |
- repeated balloon dilatation |
|
|
How to treat Barrett's esophagus complication? |
May treat with PPI - may suppress acid BUT - do NOT suppress progression of metaplasia |
|
|
Empirical treatment for GERD? (5 phases) |
Phase 1 - lifestyle - antacids (when symptomatic) Phase 2 Phase 3 - monotherapy of PPI Phase 4 - multitherapy - PPI with pro-motility agent (metoclopramide - dopamine blocker) Phase 5 - anti-reflux surgery (Nissen fundoplication) |
|
|
Examples of anti-histamine (H2)? Examples of PPI? |
Anti-histamine (H2)? - dine (raniti-, lorata-) PPI? - prazol (ome-, panto-) |
|
|
When do we need to do Nissen fundoplication in GERD? |
For severe/resistant cases: - serious esophagitis - hiatal hernia - hemorrhage - stricture / ulcer |
|
|
What is Barrett's esophagus? |
Metaplasia of: - stratified squamous epi. → columnar gastric epi. (histology) - ↑ risk of adenoma |
|
|
Can Barrett's esophagus cause cancer? |
YES - ↑ risk of adenoma - major RF of esophageal adenocarcinoma - 10% lifetime risk |
|
|
How Barrett's esophagus can occur? |
- adaptive response to GERD - WEAKLY associated with smoking |
|
|
Barrett's esophagus can be diagnosed with? |

1. Presence of GERD sx - heartburn, waterbrash 2. Positive endoscopy - red-appearing bands of metaplastic epi. - extend proximally 3. Positive biopsies |
|
|
How to initially treat Barrett's esophagus? |
Treat GERD: - acid suppression (antacids / antihistamine / PPI) - anti-reflux surgery BUT these do NOT stop progression of Barrett's esophagus |
|
|
Other methods to treat Barrett's esophagus? |
1. Endoscopic radiofrequency (laser) ablation - to resect mucosal layer 2. Esophagectomy - in high grade dysplasia 3. Cryotherapy / argon plasma coagulation 4. Photodynamic therapy |
|
|
If diagnosis confirmed to be Barrett's esophagus, what is needed to prevent cancer? |
Barrett's esophagus is PRECURSOR of adenocarcinoma 1. Regular endoscopic surveillance - if without dysplasia (every 2-3 years) - if with low grade dysplasia (every 6 months) 2. Esophagectomy - if with high grade dysplasia |
|
|
2 main types of esophageal cancer? |
- squamous cell carcinoma - adenocarcinoma |
|
|
Squamous cell carcinoma VS Adenocarcinoma? |
Squamous cell carcinoma - Where? - proximal 1/3 (upper / mid thoracic esophagus) - RF? - alcohol, smoking, hot foods, nitrosamine, HPV, achalasia Adenocarcinoma - Where? - lower 1/3 of esophagus - RF? - GERD, Barrett's esophagus |
|
|
What can be seen in patients with esophageal cancer? |
- progressive, painless dysphagia * initially to solid food * then to other types of food - anorexia / loss of weight - odynophagia / hoarseness * tumor may compress recurrent laryngeal n. - esophageal-tracheal fistula * aspiration pneumonia - dyspnea * if metastasis to lungs - chest pain, radiates to back - Horner's syndrome (MAPLE) * tumor may compress sympathetic n. |
|
|
How can we diagnose esophageal cancer? |
1. Upper GI endoscopy - with biopsies 2. Barium swallow - to evaluate any stricture 3. Thoracic / abdominal XR, CT - for staging 4. Esophageal US - if CT -ve for metastasis - to see depth / invasion of tumor |
|
|
Staging for esophageal cancer? |
I-II - confined to esophagus III - positive nodes / locally invasive IV - distant metastasis |
|
|
We can treat esophageal cancer with palliative treatment - how? |
1. Metallic stents / laser tx - to improve swallowing 2. Palliative radiotherapy - to shrink the tumor 3. Nutritional support 4. Analgesia |
|
|
What is the prognosis of esophageal cancer? |
Poor - except if only confined to esophagus |
|
|
How to cure & improve prognosis of esophageal cancer? |
1. Esophagectomy - for stage I & II tumors 2. Neoadjuvant chemoradiotherapy - platins, 5-FU - to improve prognosis |
|
|
What is chronic gastritis? |
- inflammation of gastric mucosa |
|
|
What causes chronic gastritis? |
- infection (Helicobacter pylori) - drugs (NSAIDs) - alcohol - stress - autoimmune disorders |
|
|
How to diagnose chronic gastritis generally? |
- endoscopy |
|
|
Symptoms that can be seen in patients with chronic gastritis? |
Usually ASYMPTOMATIC But, may have: - dyspepsia - GI bleeding (hematemesis / melena) - epigastric pain - nausea / vomiting |
|
|
Gastritis can also be caused by systemic disorders - examples? |
- TB - amyloidosis - Crohn's diseases |
|
|
How to treat gastritis caused by systemic disorders? |
- treat causative causes * direct to causative agent |
|
|
Gastritis can be caused by radiation. What are possible complications of radiation gastritis? |
- pyloric stenosis - perforation |
|
|
Chronic gastritis can be divided into 3 histological patterns - which are? |
1. Hypertrophic - Menetrier's disease 2. Atrophic - gastritis due to ↓ vitamin B12 - autoimmune chronic gastritis 3. Non-atrophic |
|
|
What is Menetrier's disease? |
- rare disease - typical in middle / old age - protein-losing enteropathy (due to exudation from mucosa) |
|
|
What happens in Menetrier's disease? |
- replacement of parietal & chief cells by mucous-secreting cells → dis-pattern of gastric mucosa (eventually with ulcer) → fluid & protein loss into stomach |
|
|
How to diagnose Menetrier's disease? |
- Barium swallow - endoscopy * shows coarse & enlarged gastric folds |
|
|
How can we treat Menetrier's disease? |
- anti-secretory drugs - partial gastrectomy |
|
|
What happens in atrophic gastritis? |
- chronic inflammation that damage parietal cells (end-stage chronic gastritis) - 4x risk of gastric cancer |
|
|
What causes atrophic gastritis? |
1. H. pylori infections 2. Autoantibodies (autoimmune) * both may damage parietal cells |
|
|
Effect of atrophic gastritis to patients? (damage of parietal cells) |
1. ↓ acid / pepsin secretion - hypochlorhydria 2. lost of intrinsic factor - ↓ vitamin B12 → pernicious anemia (megaloblastic anemia) ** ↑ risk of gastric cancer (4x higher!) |
|
|
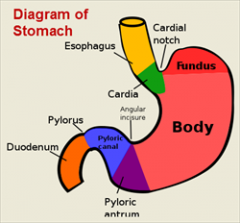
For atrophic gastritis is caused by autoimmunity, which part of stomach is affected? |
Body of stomach - antrum is spared |
|
|
How to rule out autoimmune chronic gastritis? |
- check presence of circulating antibodies (Ab) in blood |
|
|
How to rule out atrophic gastritis NOT due to autoimmune? |
NOT autoimmune etiology when: - negative anti-parietal cells (antibodies) - negative anti-intrinsic factor (antibodies) - ↓ vitamin B12 - ↑ methylmalonic acid (MMA) - macrocytic anemia (MCV > 100) |
|
|
Most common cause of chronic gastritis? |
H. pylori infection (80%) |
|
|
How to diagnose H. pylori infection? |
- antibodies to H. pylori (serology) - urea breath test - fecal antigen (Ag) test - biopsy |
|
|
How to treat chronic gastritis with H. pylori infection? |
1. Acid suppressant - PPI (most commonly - prazole) - H2 blockers 2. ATB - amoxicillin - clarithromycin - metronidazole ** usually combine PPi + 2 ATB (amoxicillin / metronidazole + clarithromycin)
|
|
|
Which medications can be used to suppress gastric acidity? |
1. PPI 2. H2 blockers 3. Antacids 4. Prostaglandins |
|
|
How PPI works in suppressing gastric acidity? |
- inhibit H+,K+‑ATPase (enzyme for secretion of H+) - promote ulcer healing - can also eradicate H. pylori |
|
|
Why PPI is used nowadays compared to H2 blockers? |
- greater rapidity of action & efficacy |
|
|
Side effects of long term use of PPI? |
Although NOT WELL described / studied - it may cause: - ↓Fe - ↓Ca (osteoporosis) - ↓ vitamin B12 - infections (pneumonia, Traveler's diarrhea, peritonitis, nephritis) |
|
|
How H2 blockers help to suppress gastric acidity? |
-competitively inhibit histamine at H2 receptor → suppress gastrin-stimulated acid secretion → proportionately ↓ gastric juice volume - also ↓ histamine-mediated pepsin secretion |
|
|
Side effects of H2 blockers? |
Cimetidine: - minor antiandrogen effects * less commonly, erectile dysfunction - changes of mental status - diarrhea - rash, drug fever - myalgias - thrombocytopenia - sinus bradycardia - hypotension after rapid IV administration All H2 blockers: - interact with P‑450 →delay metabolism of other drugs * phenytoin * warfarin * diazepam * lidocaine |
|
|
Define peptic ulcer disease? |
Ulcers = erosion of GI mucosa - may penetrate muscularis mucosa Ulcers, present in: - lower esophagus OR - stomach OR - duodenum |
|
|
What increase & decrease prevalence of peptic ulcer disease? |
Increase prevalence - use of NSAIDsDecrease prevalence - widespread use of medications to eradicate H. pylori |
|
|
What are causes of peptic ulcer disease? |
1. H. pylori infection 2. NSAIDs 3. Smoking - impair ulcer healing 4. Zollinger-Ellison syndrome - hypersecretion of gastrin |
|
|
H. pylori infections usually occur in which patients? |
- older patients > 50 y.o. - more in male? |
|
|
How H. pylori causes peptic ulcer? |
1. Produce urease - to produce NH3 → ↑ pH of stomach (allow H. pylori to survive) - may also erode mucus barrier 2. Cytotoxins & mucolytic enzymes - bacterial protease, lipase - damage mucosa → ulcerogenesis |
|
|
How NSAIDs causes peptic ulcer? |
- disrupt normal mucosal defense & repair →making mucosa more susceptible to acid |
|
|
Patients with peptic ulcer may come with these symptoms - which are? |
- recurrent epigastric pain * burning pain * sensation of hunger - anorexia, nausea - anemia (if bleeding) |
|
|
If peptic ulcer is NOT treated, what can happen? (complications) |
- hemorrhage (melena, hematemesis) - acute perforation with peritonitis - gastric outlet obstruction - dehydration - visible gastric peristalsis |
|
|
What does it mean with gastric outlet obstruction in peptic ulcer? What will happen? |
Ulcer may cause scarring, spasm & inflammation May lead to: - loss of appetite (LOA) - persistent bloating - abdominal distention - nausea, vomiting * loss of weight (LOW) * alkalosis (loss of HCl) * dehydration (loss of K) |
|
|
What can be seen in patients with acute perforation with peritonitis? |
- sudden, intense epigastric pain |
|
|
Two types of peptic ulcers? |
- duodenal ulcer - gastric ulcer |
|
|
Which one is more common? (duodenal ulcer vs gastric ulcer) |
Duodenal ulcer - 4x more common than gastric ulcer |
|
|
Where is the location for duodenal ulcer and gastric ulcer? |
DU - in first few cm of duodenum GU - in stomach |
|
|
What are common MAJOR risk factors of both DU & GU? |
- H. pylori infection - NSAIDs |
|
|
Other MAJOR risk factors for DU & GU? |
DU - steroids GU - smoking - reflux of duodenal contents - stress - burns |
|
|
How to differentiate pain from DU & GU? |
Both have epigastric pain DU - more consistent * can even awake patients at NIGHT - typically BEFORE meals - relieved by eating / drinking milk GU - less consistent - DURING / AFTER MEAL - relieved by antacids (NOT by eating!) |
|
|
How can we describe patients's weight with DU & GU? |
DU - gain weight GU - loss of weight |
|
|
How to diagnose peptic ulcers? |
- clinical presentation * by differentiating epigastric pain - upper GI endoscopy * take multiple biopsies TRO malignancy - test of H. pylori infection - CT * TRO perforation, peritonitis |
|
|
How to initially manage peptic ulcers? |
Treat underlying causes: - eradicate H. pylori - smoking cessation - reduce NSAIDs / steroids |
|
|
[Repeat] How to eradicate H. pylori? |
1. PPI + 2 ATB - amoxicillin / metronidazole - clarithromycin 2. If unsuccessful, try Bismuth + PPI + 2 ATB 3. Long term acid suppression - if all therapies failed |
|
|
Can we treat peptic ulcer with surgery? |
YES - Billroth I (for chronic GU) - Billroth II (for DU) |
|
|
What happens in Billroth I? |
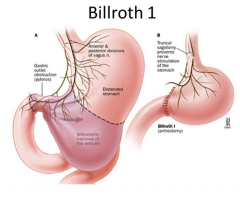
Billroth I - gastroduodenostomy (for GU) - to ↓ stomach capacity * so, food direct to duodenum |
|
|
What happens in Billroth II? |
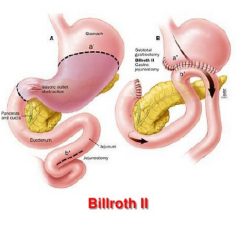
Billroth II - gastrojejunostomy (for DU) - quick emptying of stomach - leave duodenum there (needed for digestion) * income of pancreatic juice / bile |
|
|
Complications of Billroth surgery? |
1. Dumping syndrome 2. LOW 3. Anemia 4. Metabolic bone disease 5. ↑ risk of gastric cancer 6. Diarrhea, maldigestion |
|
|
What is dumping syndrome? |
Diarrhea - due to hyperosmolar food draw water into small intestine lumen Abdominal discomfort |
|
|
How anemia can occur after Billroth procedure? |
- removal of part of stomach → marked ↓ of gastric acid production → acid is needed to dietary Fe to readily absorbable form in duodenum |
|
|
How metabolic bone diseasecan occur after Billroth procedure? |
Malabsorption of vitamin D & calcium |
|
|
Types of gastric carcinoma? |
1. Adenocarcinoma (95%) - mainly 2. Gastrointestinal Stromal Tumor (GIST) (1-3%) 3. Gastric Lymphoma (2%) 4. Gastric Carcinoid (1%) |
|
|
Gastric carcinoma is dangerous, why? |
- poor prognosis - majority is INCURABLE at diagnosis * symptoms appear late (in advanced stage) |
|
|
There are varieties of appearance in gastric carcinoma - for examples? |
1. Malignant ulcer / polyp 2. Leather bottle stomach - diffuse infiltration of submucosa with fibrosis - small stomach with thick walls |
|
|
Most common cause of gastric carcinoma? |
H. pylori |
|
|
What are risk factors of gastric cancer? |
1. Nitrosamine in diet 2. Smoking 3. High alcohol intake 4. Chronic gastritis 5. Gastric polyps 6. Family history |
|
|
Which types of chronic gastritis can lead to gastric cancer? |
- (MAINLY)gastritis caused by H. pylori infection - autoimmune gastritis (with pernicious anemia) - Menetrier's disease |
|
|
Nitrosamines are high in which diet? Why? |
Carcinogenic - smoked foods - pickled vegetables |
|
|
Patients with gastric carcinoma may have these early symptoms, which are? |
1. Dyspepsia - may suggest peptic ulcer 2. Abdominal pain 3. ALARM symptoms - anemia (due to occult blood loss) - LOW (dietary restriction) - anorexia - recent onset of progressive dyspepsia - melena / hematemesis (uncommon) 4. Dysphagia - cancer in cardiac region obstruct esophageal outlet |
|
|
Late symptoms of gastric carcinoma? |
5. Early satiety - tumor obstruct pyloric region 6. Upper GI bleeding 7. Gastric obstruction 8. Perforated malignant ulcer |
|
|
Gastric carcinoma may have more symptoms after metastasis. For examples? |
Usually appear after early symptoms 1. Ascites - when metastasis to peritoneum - build up of fluid in abdomen 2. Jaundice - when metastasis to liver - yellowing of eyes and skin 3. Virchow's node - enlarged swollen LN above left clavicle (abdominal lymphatic fluid drain here) 4. Fracture - weakening of bone (bone metastasis) |
|
|
How can we diagnose gastric carcinoma? |
1. Serology - FBC (RBC, WBC, PLt), U&E, Hb, Fe - LFT (liver metastasis) 2. Gastroscopy with multiple biopsies - endoscopy - biopsy - can check HER2 genes & proteins 3. Barium swallow (upper GI series) - use X-ray to look for abnormal sites 4. Abdominal / chest CT - for staging - may combine with endoluminal US (to access local spread accurately) 4. PET scan |
|
|
Stages of gastric cancer? |
I - confined to gastric wall - mucosa + submucosa II - mucosa + submucosa - muscularis mucosa + subserosa III IIIA - mostly already spread to serosa IIIB - spread to nearby organs (spleen, transverse colon, liver) + LN (1-2) IIIC - spread to nearby organs (spleen, transverse colon, liver) + LN (3/>) IV - distant metastasis |
|
|
Management of gastric cancers depends on? |
1. If the tumor is resectable - early gastric ca. (T1-T2 / N0-N1) 2. If presence of distant metastasis - palliative treatment |
|
|
If tumor is resectable, what should we do to the gastric cancers? |
1. Proximal total gastrectomy / distal esophagectomy - for tumors in gastroesophageal junction / cardiac of stomach 2. Total gastrectomy (with roux-en-y anastomosis) - for tumors in body of stomach 3. Subtotal gastrectomy - for antral tumors 4. Neoadjuvant chemotherapy |
|
|
What can be done as palliative treatment for gastric carcinoma? |
1. Limited gastrectomy - to palliate bleeding / perforated tumors 2. Endoscopic laser ablation / endoluminal stent - for obstructiong tumors 3. Chemotherapy 4. Radiotherapy |
|
|
Medications use for chemotherapy of gastric carcinoma? |
Combine: - 5-FU (fluorouracil) - doxorubicin - mitomycin - cisplatin |
|
|
5 years survival of gastric carcinoma? |
1. If TiS / T1 N0 M0 (80%) 2. If T2-T3 with N1 M0 (20-60%) 3. If M1 (3% only) |
|
|
What is gastrointestinal stromal tumors (GIST)? |
All non-lymphoid & non-epithelial tumors of GIT - derived from mesenchymal precursor cells in gut wall |
|
|
How GIST can occur? |
- mutations of growth factor receptor gene, C-KIT - previous radiation therapy to abdomen for other tumors |
|
|
Examples of GIST? |
- leiomyomas / leiomyosarcomas - lipomas / liposarcomas - fibrosarcromas - GANTs (GI autonomic nerve cell tumors) |
|
|
Locations of GIT that we can find GIST? |
WHOLE GIT - most commonly stomach (60-70%) - others - rectum, small intestine (20-25%) |
|
|
Patients with GIST may have these symptoms... |
Depends on location - but, usually have: - bleeding - dyspepsia - obstruction |
|
|
How to diagnose GIST? |
1. Endoscopy, with biopsy 2. Endoscopic US - for staging |
|
|
How to treat GIST? |
1. Surgical removal - if small tumor - excision - if large tumor - treat with Glivec (anti-CD-117 Ab) before surgery 2. Tyrosine kinase inhibitor - imatinib |
|
|
What is gastric lymphoma? |
Almost always Non-Hodgkin Lymphoma (NHL) - most commonly B-cell |
|
|
Overview about Non-Hodgkin Lymphoma? |
Disorders involving malignant monoclonal proliferation of lymphoid cells in lymphoreticular sites - LN - bone marrow - spleen - liver - GIT |
|
|
Gastric lymphoma may have similar symptoms with? |
Gastric carcinoma |
|
|
How to treat gastric lymphoma? |
- resection & adjuvant chemotherapy - radiochemotherapy (for advanced stage) |