![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
24 Cards in this Set
- Front
- Back
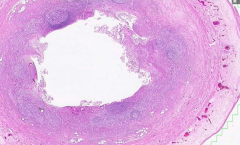
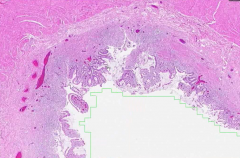
Section taken from appendix |
Normal appendix
*Thin serosa, lymphoid tissue in submucosa, no inflammatory cells in muscularis |
|
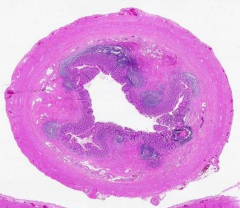
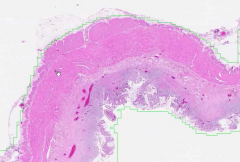
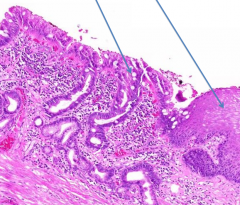
Section taken from appendix |
Acute Appendicitis
*General architecture maintained, but no clear mucosa visible and ulceration apparent *Presents w/ RLQ pain w/ rebound tenderness and N/V |
|
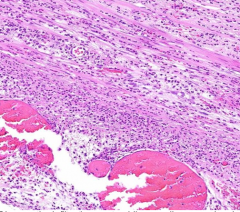
Section taken from appendix |
Acute Appendicitis
*Many neutrophils and some eosinophils that infiltrate b/w smooth mm cells *Thinned out muscularis makes appendix prone to rupture *Dilated BV |
|
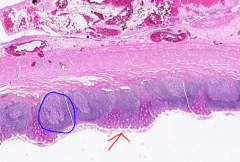
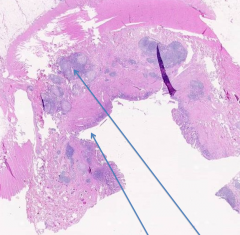
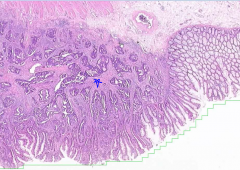
Section taken from appendix |
Normal Appendix
*Red arrow points to colonic epithelium w/ crypts *Lymphoid follicles in submucosa |
|

From GB |
Chronic Cholecystitis
*Thickened muscularis due to bile sludge or stone obstruction *Fibrosis
|
|
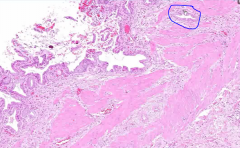
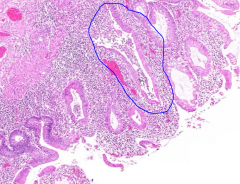
From GB |
Chronic Cholecystitis
*Hypertrophy of mm leads to trapping of epithelium = "Rokitansky-Aschoff Sinus" (blue) *May find collections of foamy histeocytes
|
|
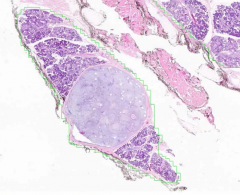
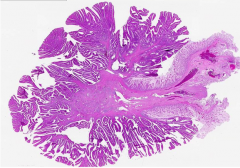
From Parotid Gland |
Pleomorphic Adenoma
* Dark purple = normal serous & mucinous glands, Light purple mass = tumor *Pseudo-encapsulated = high rate of reoccurance *predominantly in females in parotid
|
|
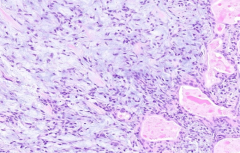
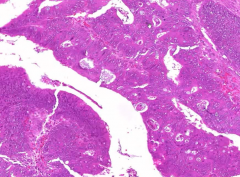
From Parotid Gland |
Pleomorphic Adenoma
*Chrondromyxoid tumor of spindle myoepithelial cells and epithelial ductal cells (pink) *Benign but can transform to malig. |
|
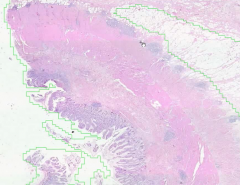
From SI |
Crohn's Disease
*Transmural inflammation (vs. Ulcerative Colitis which is limited to mucosa) *Tip has fat necrosis that leads to adhesions and fistulas *Hyperplasia of muscularis propria |
|
From SI |
Crohn's Disease
*Ill-defined granuloma (top) *Fissure (deep and narrow) ulcer *Skip Leisons |
|
From Terminal Illeum |
Ulcerative Collitis
*Inflammation limited to mucosa (musclaris is untouched!) -- may spill over into submucosa
|
|
From Terminal Illeum |
Ulcerative Collitis
*Broad ulcer in mucosa only *Continuous leisions |
|
From Terminal Illeum |
Crypt Abscess in Ulcerative Collitis
*Lymphocytes and Neutro's filing cyrpt *Crypt dropout and loss of normal architecture |
|
From esophagus |
Barret's Esophagus
*Salmon-velvety plaque *Intestinal Metaplasia w/ goblet cells (left) *Right shows normal of squamous epithelium *Increased risk of AdenoCA if dysplasia present |
|
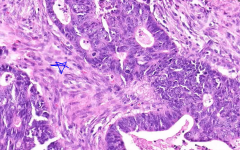
From Colon |
Adenocarcinoma of Colon
*Hyperchromatic cells forming tubular structures and increased mitotic figures w/ desmoplastic stroma (blue star) that indicates invasive CA |
|
From Colon |
Adenocarcinoma of Colon
*pale right = submucosa *Blue star = desmoplastic stroma *Complex/Cribiform Glands (vs normal glands on right)
|
|
From Colon |
"Dirty Necrosis" in Adenocarcinoma of Colon
*Glandular structure filled w/ dead nuclei *If you find this type of necrosis in liver, you can deduce that it is a MET from colon |
|
From Colon |
Pedunculated polyp w/ Tubulovillous Adenoma
*villi architecture w/ tubules underneath *darker purple due to loss of mucus producing goblet cells *NO dysplasia in stalk = curative polypectomy! |
|
From Colon |
Pedunculated polyp w/ Tubulovillous Adenoma
*High grade dysplasia indicated by 'pencil-shaped' nuclei, cribiforming/complex glandular vs. lower left corner = low grade |
|
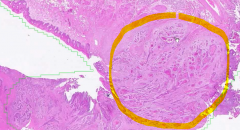
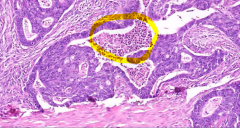
From tongue |
Squamous Cell Carcinoma of the Mouth
*Desmoplasia (paler area circled) w/ large islands of keratin-producing cells
*Also see SCC in Anus |
|
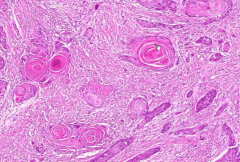
From Tongue |
Squamous Cell Carcinoma of the Mouth
*Keratin pearls indicating SCC *Assoc. w/ tobacco (chewing & smoking) & EtOH *NOTE: HPV-driven tumors that occur in post. mouth have more basaloid cell histo |
|
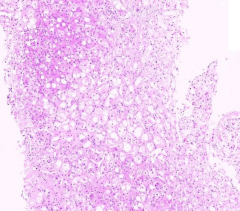
From Liver |
Alcoholic Steatohepatitis
*Paler than normal liver due to increased fat infiltration *Inflammatory cells among hepatocytes (*main way to tell this is due to EtOH vs NASH) |
|
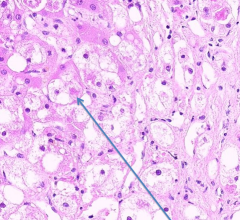
From Liver |
Alcoholic Steatohepatitis
*Mallory Hyaline Bodies = diagnositic! |
|
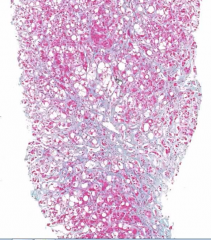
Trichrome Stain of Liver |
Alcoholic Steatohepatitis
*Blue = Fibrosis *'Tram-track' (peri-sinusoidal) fibrosis (vs viral hepatitis that has fibrosis in thick bands) *Fibrosis centered around central vein (zone 3) in both alcoholic liver and NASH
|