Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
125 Cards in this Set
- Front
- Back
|
Are minor congential anomalies of the biliary tract common or rare?
|
common
|
|
|
Are major congenital anomalies of the biliary tract common or rare?
|
rare
|
|
|
What is the clinical significance of minor congenital anomalies of the biliary tract?
|
These have no clinical significance unless surgery is needed-we do not want to injure the gall bladder or ducts inadvertently.
|
|
|
Abberant location of the gall bladder and irregular but functional biliary tract branches-->are these examples of minor or major anomalies?
|
Minor anomalies
|
|
|
5-10% of gall bladders are embedded in the liver. What type of anomaly (major or minor) is this an example of?
|
Abberant location-->Minor anomaly
|
|
|
What is a folded fundus called?
|
Phrygian cap
|
|
|
A golding over of the fundus of the gall bladder is called what?
|
Folded fundus or phrygian cap.
|
|
|
Gall bladder: agenesis, duplicated, bilobed-->these are all examples of a major or minor gall bladder anomaly?
|
Major anomaly
|
|
|
Are congenital anomalies involving location major or minor?
|
Minor
|
|
|
Are congenital anomalies involving structure major or minor?
|
Major
|
|
|
Bile duct structural anomalies are often associated with what?
|
Other anomalies, involving the heart, spleen, or GI tract (all the one-sided structures)
|
|
|
Bile Duct: Agenesis of all or part, Atresia-fetal, perinatal, Polysplneia (multiple spleens) are all examples of a minor or major anomaly?
|
Major anomaly
|
|
|
What is cholelithiasis also known as?
|
Gallstones
|
|
|
What are the 2 major types of cholelithiasis?
|
1.Cholesterol Stones
2.Pigment (bilirubin) stones |
|
|
-Common in western, industrialized nations.
-Common in Mexican and Hispanic & Native Americans -When the stones form individually, they are usually round, whereas when they form in large numbers simulataneously, will have a faceted surface WHAT TYPE OF CHOLELITHIASIS? |
Cholesterol Stones
|
|
|
Cholesterol Stones
|
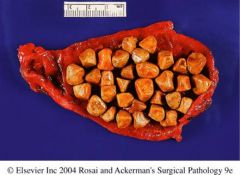
What type of cholelithiasis?
|
|
|
What causes cholesterol gallstones?
|
1.High cholesterol or low bile salts-->crystallization of cholesterol, forming gallstones
2.Bile Stasis |
|
|
What are the 2 most important factors for increased risk of high cholesterol?
|
Increased age, female gender (estrogen)
|
|
|
Changes in hormone or nervous control of BG, and starvation, can lead to what?
|
Bile Stasis-->Cholesterol Stones
|
|
|
Increased cholesterol, decreased lecithin, and decreased Na taurocholate all cause what?
|
Increase risk of cholesterol stone formation
|
|
|
What is the pathogenesis of cholesterol stone formation?
|
1.Increase chol
2.Decrease Lecithin 3.Decrease Na taurocholate |
|
|
1.Supersaturated bile
2.Hypomotile GB (stasis) 3.Accelerated nucleation 4.Mucus hypersecretion All of these simulatneous defects are needed for what? |
Cholesterol Gallstone formation
|
|
|
What are the 4 simultaneous defects needed for cholesterol gallstone formation?
|
1.Supersaturated bile-liver hypersecretion
2.Hypomotile GB (stasis) 3.Accelerated nucleation-proteins that aid in stone formation 4.Mucus hypersecretion-acts as "scaffolding" for stone formation |
|
|
What do pure cholesterol gallstones look like?
|
Rare, yellow, radiolucent
|
|
|
What do cholesterol gallstones mixed with other components looke like?
|
Radio-opaque (white, grey, black) but usually sill remain difficult to see on x-ray.
|
|
|
Chol Gallstones
|

What is this?
|
|
|
Chol Gallstones
|

What is this?
|
|
|
-Often involved with infections not seen in the US, and hence are more prevalent in non-western, developing countries.
-Most common in Asian countries WHAT TYPE OF CHOLELITHIASIS? |
Pigment (bilirubin) stones
|
|
|
pigment (bilirubin) stones
|
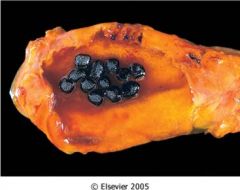
What type of cholesthiasis?
|
|
|
Why are pigment (bilirubin) stones produced?
|
Any disorder that favors production of unconjugated bilirubin will favor pigment stone formation.
|
|
|
What are the 2 main types of pigment (bilirubin)stones?
|
1.Brown
2.Black |
|
|
Which type of pigment stone is radioluscent, which is opaque?
|
1.Brown: Radioluscent
2.Black: Radio-opaque |
|
|
Where do brown pigment (bilirubin) stones form from?
|
Form in infected bile ducts
|
|
|
Where do black pigment (bilirubin) stones form from?
|
Form in sterile bile in GB
|
|
|
What type of pigment (bilirubin) stones are responsible for chronic intravascular hemolysis?
|
Black pigment (bilirubin) stones
|
|
|
How does the epidemiology of cholesterol stones differ from the epidemiology of pigment stones?
|
1.Cholesterol Stones: Increase in Wester Industrialized countries, Mexican and Native Americans
2.Pigment Stones: Increase in Non-Western/Developing countries; Asia |
|
|
What is cholesterolosis?
|
-An incidental finding (no clinical significance) in which there is hypersecretion of cholesterol from liver into the GB
|
|
|
Normally what does the GB do will excess cholesterol?
|
-Normally, the mucosa of the GB will take up the excess cholesterol and convert it to esters, and then eliminate it
|
|
|
In cholesterolosis, where do excess esters from the liver accumulate?
|
Esters accumulate in the lamina propria of the mucosa.
|
|
|
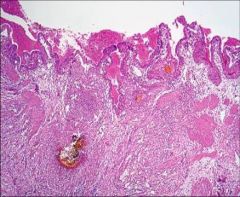
Cholesterolosis-->With xs. cholesterol, esters accumulate in the lamina propria of the mucosa.
|
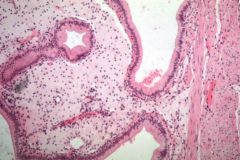
What does this show?
|
|
|
Cholesterolosis-->Mucosa with yellow flecks; "strawberry GB"
|
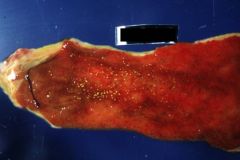
What is shown?
|
|
|
In cholesterolosis, what does the GB look like on dissection?
|
-Mucosa with "yellow flecks" flecks; "strawberry GB"
-(Microscopically forms a club-like swelling of the mucosal surface which corresponds grossly as a yellow flecked surface of the mucosa. |
|
|
Cholelithiasis
|
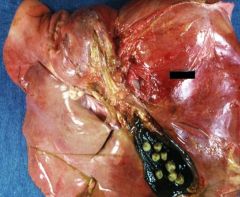
Shown is a gross illustration of what?
|
|
|
Are patients with cholelithiasis symptomatic?
|
Usually not, only 1/3 of patients present with symptoms, usually PAIN
|
|
|
In cholelithiasis, what is pain usually associated with?
|
Pain is associated with the stone obstruction?
|
|
|
What is the consequent inflammation associated with GB obstruction in cholelithiasis called?
|
Cholecystitis
|
|
|
What is intermittent GB pain due to obstruction called in Cholelithiasis?
|
Colicky
|
|
|
In cholelithiasis, are small stones or large stones at a greater risk for obstructions?
|
Small stones
|
|
|
In cholelithiasis, what do large stones often do? What is this called?
|
Large stones do not often obstruct, but can erode their way out of the GB, and into the small intestine and obstruct it-->called gallstone ileus
|
|
|
Empyema, perforation, fistulae, inflammation of biliary tree (cholangitis) are all complications of what?
|
Cholelithiasis
|
|
|
What sized stones increase the risk of GB carcinoma?
|
All sized stones
|
|
|
What is GB inflammation called?
|
Cholecystitis
|
|
|
What is cholecystitis often associated with?
|
Gallstones
|
|
|
What is one of the most common indications for abdominal surgery?
|
Cholecystitis
|
|
|
What are the risk factor for cholecystitis similar to?
|
Same as those for gallstones.
|
|
|
What is an acute chemical irritation, inflammation of an obstructed gallbladder called?
|
Acute calculus cholecystitis
|
|
|
Blockage of neck or cystic duct-->bile cannot flow out-->bile becomes toxic lysolecithin (detergent)-->this disrupts the mucosa leading to prostaglandin release, inflammation, dysmotility, distention, and eventually decreased blood flow-->ischemia of GB tissues-->possible necrosis and serious side effects
This sequence describes the pathogenesis of what? |
Acute calculus cholecystitis
|
|
|
RUQ pain, fever, anorexia, N/V...these are all clinical features of what?
|
Acute calculus cholecystitis
|
|
|
What does hyperbilirubinemia without jaundice indicate? And in what illness is this found?
|
Acute calculus cholecystitis
|
|
|
-Hyperbilirubinemia without jaundice
-Increased WBC's -Increase serum alkaline phosphatase -Previous episode(s) likely -Surgical emergencies may happen if necrosis occurs These are clinical symptoms of what illness? |
Acute calculus cholecystitis
|
|
|
What is the difference b/w Acute calculus cholecystitis and Acute Acalculus cholecystitis?
|
1.Acute calculus cholecystitis-->with gallstones
1.Acute Acalculus cholecystitis-->withOUT gallstones |
|
|
In what illness are patients severly ill with additional circumstances such as severe trauma, burns, multi-system organ failure, sepsis, postoperative state, postpartum state?
|
Acute Acalculus Cholecystitis
|
|
|
What is Acute Acalculus Cholecystitis due to?
|
Due to ischemia and poor perfusion of the GB
-cystic artery is an end artery, no collaterals -essentially patients start at end point of acute calculus cholecystitis, they begin with decreased mucosal profusion -At a much greater risk for complications |
|
|
What illness can rarely be due to a bacterial infection?
|
Salmonella typhi, stapylococci, clostridia
|
|
|
Often clincial features of this illness are insidious. They are obscured by serious conditions not related to the gallbladder. We must maintain a high level of suspicion to avoid the risk of gangrene and perfusion. What illness?
|
Acute Acalculus Cholecystitis
|
|
|
Acute Cholecystitis GB-->GB is ENLARGED with thickened walls, RED-purple in color, may be BLOTCHY due to neutrophil migration to the serosa, showing a suppurative, fibrin-filled exudates
|

What is shown?
|
|
|
Wall of GB in Acute Cholecystitis. Edema, hyperemia (red). If gangrenous: green-black (necrotic) with perforation
|

What is shown?
|
|
|
-Acute Cholecystitis: Microscopioc Morpholgy
-Acute inflammatory reaction with neutrophils, edema, BV congestion |
What is shown?
|
|
|
What is the differential diagnosis of acalculous v calculous cholecystitis?
|
No specific differences except for absence or presence of stones
|
|
|
1.Usually associated with gallstones
2.Thought to be due to recurrent attacks of cholecystitis 3.In 1/3 of cases (E.coli, enterococci) are found in GB, but not thought to be the cause WHAT IS THE ILLNESS? |
Chronic Cholecystitis
|
|
|
What does the GB serosa look like in chronic cholecystitis?
|
Smooth serosa
|
|
|
What does the GB wall look like in chronic cholecystitis?
|
Thick, opaque, gray-white wall, NOT red
|
|
|
What does the GB lumen look like in chronic cholecystitis?
|
Clear green-yellow mucoid bile
|
|
|
What does the GB mucosa look like in chronic cholecystitis?
|
Preserved mucosa
|
|
|
What is a "porecelain" GB wall? And what illness is it associated with?
|
1.Wall is calcified (associated with cancer)
2.Chronic cholecystitis |
|
|
What are hyrdops? And what illness is it associated with?
|
Hydrops=clear secretions into GB
Associated with chronic cholecystitis |
|
|
Chronic Cholecystitis-->hydrops, clear secretions into GB
|
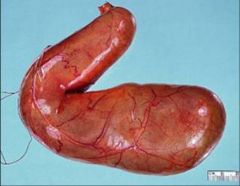
What is shown in this GB?
|
|
|
Chronic Cholecystitis: "Porcelain" GB-->wall is calcified (associated with cancer)
|

What is shown?
|
|
|
-Smooth serosa
-Thick, opaque grey-white wall, NOT red -Clear, yellow mucoid bile in lumen -preserved mucosa -"Porcelain" GB: wall is calcified (associated with cancer) -"Hydrops" clear secretions into GB What illness? |
Chronic Cholecystitis-Gross Morphology
|
|
|
-Lymphocytes, plasma cells, macrophages
-Whiteness and thickness of wall comes from fibrosis -Rokitansky-Ashoff sinuses WHAT ILLNESS? |
Chronic-Cholecystitis-Microscopic Pathology
|
|
|
What are Rokitansky-Ashoff sinuses? In what illness are they found?
|
1.Invagintion of mucosal epithelium deep into wall of GB. Benigh reactive change that mimics invasive carcinoma.
2.Chronic cholecystitis |
|
|
Chronic Cholecystitis: Microscopic Morphology
1.Lymphocytes, plasma cells, macrophages 2.Whiteness and thickness of wall comes from fibrosis 3.Rokitansky-Ashoff sinuses |
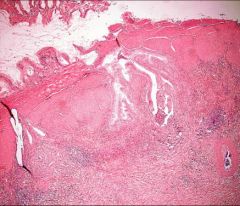
What is shown?
|
|
|
1.Epigastric, RUQ pain, N/V
2.Recurrent attacks 3.Fatty food intolerance CLINICAL FEATURES OF WHAT ILLNESS? |
Chronic Cholecystitis
|
|
|
1.Bacterial superinfection-->cholangitis, sepsis
2.Perforation-->abscess 3.Rupture-->peritonitis 4.Aggravate a pre-existing illness WHAT ARE THESE COMPLICATIONS OF? |
Complications of Acute and Chronic cholecystitis
|
|
|
A stone in any biliary duct, although many consider it to properly refer to a stone in the common bile duct. WHAT IS THIS CALLED?
|
Choledocholithiasis
|
|
|
In choledocholithiasis, where do stones form in the:
1.west 2.asia |
1.West-stones form in GB
2.Asia-stones form in ducts due to infection |
|
|
In choledocholithiasis, what do symptoms depend on?
|
Symptoms depend on where obstruction occurs:
1.obstruction (pancreatitis) 2.Infection (acute cholangitis) 3.Concurrent cholecystitis |
|
|
Bacterial infection of the bile ducts due to obstruction is called what?
|
Acute cholangitis.
|
|
|
How does bacterial infection of the bile ducts occur in acute cholangitis?
|
Enteric bacteria enter ducts via sphincter of oddi due to obstruction.
|
|
|
What bacteria is most commonly involved in acute cholangitis?
|
E.coli or Klebsiella (gram-bacilli)
|
|
|
What is ascending cholangitis?
|
Cholangitis that ascends into intra-hepatic duct system.
|
|
|
What is the classic triad of symptoms in acute cholangitis?
|
Fever/chills, abdominal pain, jaundice
|
|
What is the microscopic morphology of acute cholangitis?
|
Mural neutrophils move toward lumen
|
|
|
Acute cholangitis-->mural neutrophils move toward lumen
|
What is shown in this GB?
|
|
|
What is the most severe form of acute cholangitis?
|
Suppurative cholangitis is most severe form-->purulent bile and spesis
|
|
|
This congenital anomaly involves complete obstruction of the extra-hepatic biliary tree for first 3 months of life...WHAT IS IT?
|
Biliary atresia
|
|
|
What causes congential biliary atresia?
|
Inflammation-->obstruction-->secondary changes in extra-hepatic ducts and hepatocytes-->secondary biliary cirrhosis
|
|
|
-Most frequent cause of death from liver disease in childhood
-50-60% referred for liver transplants WHAT CONGENITAL ILLNESS? |
Congenital Biliary Atresia
|
|
|
What are the 2 main forms of congenital biliary atresia?
|
2 main forms are based on timing of duct obstruction
1.Perinatal form 2.Fetal form |
|
|
Thought to occur after birth, the biliary tree is destroyed. There may be a genetic inheritance, with a viral (reovirus or rotavirus), or toxic insult. WHAT FORM OF CONGENITAL BILIARY ATRESIA?
|
Perinatal form
|
|
|
Occurs intrauterine, often along with other anomalies of organs. WHAT FORM OF CONGENITAL BILIARY ATRESIA?
|
Fetal form
|
|
|
-F>M, Asian/African Americans>Caucasian Americans
-Stools initially normal, then pale/acholic (no bile) -Bilirubin increases -Increae in aminotransferase and alkaline phosphatase WHAT ILLNESS ARE THESE THE CLINCIAL FEATURES OF? |
Congenital Biliary Atresia
|
|
|
In biliary atresia, what does an intrahepatic duct liver biopsy show?
|
1.Porta edema/fibrosis
2.Ductile proliferation 3.Parenchymal cholestatsis in ALL ducts |
|
|
What are the features of extrahepatic bile ducts in congenital biliary atresia?
|
Inflammation-->fibrosis & stricture-->obstruction
|
|
|
What type of congential biliary atresia involves the common bile duct only and correctable surgicallY?
|
Type 1 congenital biliary atresia
|
|
|
What type of congenital biliary atresia involves the hepatic duct only and is correctable surgically?
|
Type 2 congenital biliary atresia
|
|
|
What type of congenital biliary atresia is at or above the porta hepatic? Is this correctable by surgery?
|
1.Type III
2.NOT correctable surgically b/c there is not patent ductal system for anastomosis |
|
|
-Complications:
-->cirrhosis by 3-6 mo. age -->death by 2 yrs age -Treatment: -->cure: liver transplantation with donor bile ducts WHAT ILLNESS? |
Congenital biliary atresia.
|
|
|
Congenital dilations of the common bile duct are called what?
|
Cholendocal Cysts
|
|
|
What are choledochoceles?
|
Cystic lesions protruding into duodenal lumen-->assoc. with choledocal cysts
|
|
|
-Most present before 10 years of age, includes:
1.duct dilations 2.diverticuli 3.choledochoceles WHAT ILLNESS? |
Choledocal Cysts
|
|
|
-Symptoms:
-->Jaundice, biliary pain, RUP mass -->More common in females (3-4 times) -Complications: -->Most imp. is increased risk for bile duct carcinoma (for older patients) -->Also have stone formation, stenosis, pancreatitis, and liver changes WHAT ILLNESS? |
Choledocal Cysts
|
|
|
a.Biliary tract tumors
b.Inflammatory polyps c.Adenomyosis THESE ALL HAVE WHAT IN COMMON? |
These are all benign biliary tract tumors
|
|
|
What is adenomyosis?
|
-Benign Biliary Tract Tumor
-Increased number of intramural glands in hyperplastic muscularis (smooth muscle) |
|
|
What are characteristics of carcinomas of GB and extra-hepatic bile ducts?
|
1.Both uncommon
2.Both more in older populations F>M 3.Both diagnosed at stage too late to resect surgically b/c they grow insidiously 4.Both related to chronic inflammation -->West:associated with gallstones -->East:associated with infections, parasitic disease |
|
|
What is the most common site to have carcinoma of the GB?
|
Fundus, neck
|
|
|
Is carcinoma of the GB more common in females or males?
|
Females
|
|
|
Does carcinoma of the GB usually have an infiltrating growth pattern or an exophytic growth pattern?
|
Infiltrating growth pattern
|
|
|
What are most carcinomas of the GB?
|
Adenocarcinomas: may be poor or well differentiated
|
|
|
What are 5% of carcinoma's of the gallbladder?
|
Squamous Cell or Adenosquamous
|
|
|
-Preoperative diagnosis is uncommon-->incidental diagnosis
-In the best case scenario diagnosis should be made before tumor extends due to WHAT 2 THINGS? |
1.Palpable gallbladder
2.Acute cholecystitis |
|
|
What is a cholangiocarcinoma?
|
Carcinoma of extra-hepatic biliary tree
|
|
|
-Painless, progressively increasing obstructive jaundice
-Increase in serum alkaline phosphatase, aminotransferases, direct bilirubin -Males more common than females; 1/3 have gallstones -Increase risk with chronic inflammation: Primary sclerosing cholangitis, ulcerative colitis, choledochal cysts WHAT CARCINOMA? |
Cholangiocarcinoma-Carcinoma of extrahepatic biliary tree
|
|
|
-Infiltrative, malignant glands, that leads to fibrous stromal reaction causing mass to be hard
-What type of cancer? |
Cholangiocarcinoma-->Adenocarcinoma
|
|
|
At junction of R/L hepatic ducts; slow growing, rarely metastasize
WHAT TUMOR? |
Klatskin tumor
|