Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
129 Cards in this Set
- Front
- Back
|
•CLUES
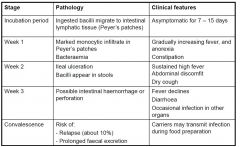
•continuous fever ,often for long time •India,PNG,East Timor,Indonesia travel •weight loss •constipation rather than diarrhoea •splenomegaly •no other clinical findings •sudden GIT bleed or quiet perforation |
TYPHOID (aka enteric fever)
- tyhpoid is a salmonella without diarrhoea |
|
|
Typhoid Pathogens
|
Typhoid
•Salmonella enterica serotype typhi (formerly Salmonella typhi) “paratyphoid” •Salmonella paratyphi A •Salmonella schottmuelleri (S. paratyphi B) •Salmonella hirschfeldii (S.paratyphi C) •Salmonella choleraesuis |
|
|
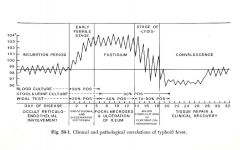
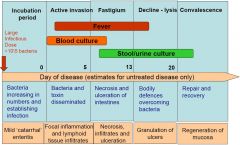
Natural history of enteric (typhoid) fever
|
|
|
|
Clinical and pathological correlations of typhoid fever
|
|
|
|
Typhoid Epidemiology
|

|
|
|
Typhoid fever in Australia
|
•
About 60 cases per year – nearly all imported • Diagnosis is usually made early – by blood culture • Treatment is based on antibiotic susceptibility tests - ceftriaxone, cefotaxime: no resistance; antibiotics of first choice - ampicillin, chloramphenicol : resistance is frequent - fluoroquinolones resistance is emerging - azithromycin potentially useful |
|
|
Story of typhoid Mary
|
- prisoner in new york
|
|
|
Causes of dysentery/infective colitis
|
•Shigella species (shigellosis, bacillary dysentery)
•Campylobacter jejuni •Enterohaemorrhagic E.coli (EHEC, or verotoxic E.coli) •Entamoeba histolytica (amoebiasis) •Clostridium difficile (pseudomembranous colitis) |
|
|
Dysentery
|
Dysentery (formerly known as flux or the bloody flux) is an inflammatory disorder of the intestine, especially of the colon, that results in severe diarrhea containing blood and mucus in the feces[1] with fever, abdominal pain,[2] and rectal tenesmus (a feeling of incomplete defecation), caused by any kind of infection.
|
|
|
Infective colitis
|
In medicine, colitis (pl. colitides) refers to an inflammation of the colon and is often used to describe an inflammation of the large intestine (colon, caecum and rectum)
|
|
|
Clinical features of dysentery
|
•
Incubation period is 1-3 days •Fever is almost invariable •Symptoms include colicky pain in lower abdomen, rectal urgency, tenesmus (sensation of incomplete rectal emptying) •Stools are frequent but of small volume; there may be blood and mucus; microscopy reveals many polymorphs +/- red cells. •Duration is 2-20 days •Antibiotic treatment hastens recovery |
|
|
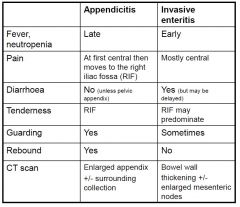
Appendicitis versus invasive enteritis
|
|
|
|
Inflammation of GIT called?
|
In medicine, enteritis, from Greek words enteron (Small Intestine) and suffix -itis (Inflammation), refers to inflammation of the small intestine. It is most commonly caused by the ingestion of substances contaminated with pathogenic microorganisms.[1] Symptoms include abdominal pain, cramping, diarrhea, dehydration and fever.[1] Inflammation of related organs of the gastrointestinal system are:
gastritis stomach gastroenteritis stomach and small intestine colitis large intestine enterocolitis large and small intestine |
|
|
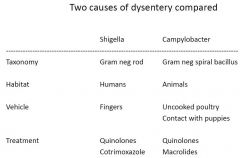
Shigella Vs Campylobacter
|
|
|
|
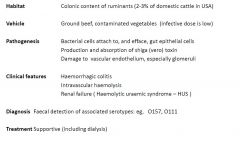
Enterohaemorrhagic E.coli (EHEC)
|
|
|
|
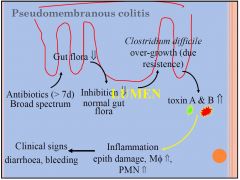
Clostridium difficile colitis
|
•
Is the consequence of overgrowth and toxin formation by C.difficile following antibiotic use. •Is more common in the elderly •May cause a characteristic pseudomembranous appearance on colonoscopy. •Is diagnosed by detection of toxins in stools. •Is treated by cessation of antibiotics and administration of oral metronidazole (or vancomycin) |
|
|
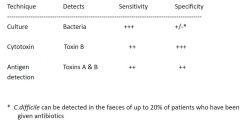
Diagnosis of Clostridium difficile - associated colitis
|
|
|
|
A/B offenders in Clostridium difficile
|
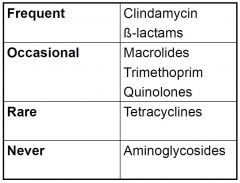
- very age related
|
|
|
Causes of diarrhoea in hospitalised patients
|
•Antibiotics (including C.difficile colitis)
•Noroviruses (in epidemics) •Hyperosmolar solutions (“tube feeds”) •Elixirs containing sorbitol or mannitol •drugs, eg, colchicine •Ischaemic colitis |
|
|
Management of acute enteric infections
|
1. Take an appropriate history
2. Assess the degree of dehydration 3. Measure serum electrolytes and creatinine 4. Perform diagnostic tests (some cases) 5. Replace lost fluid and electrolytes 6. If hospitalised….………maintain a fluid balance chart monitor serum electrolytes 7.Control nausea and vomiting 8.Use antidiarrhoeal agents sparingly 9.Use antimicrobial agents only when indicated 10. Prevent spread of disease |
|
|
1. Take an appropriate history
|
•Speed of onset and duration
•Stool characteristics •Abdominal pain •Food consumed in previous 48 hours – health of other family members •Fever •Travel – both inside and outside Australia •Current illnesses/medications (especially antibiotics) •Sexual activity/preference |
|
|
2. Assess the degree of dehydration
|
•ASK the patient/mother about the number of bowel motions, frequency of vomiting, thirst and urine output
•LOOK at the patient’s mental state, eyes, mouth/lips/tongue, breathing, jugular venous pressure •FEEL skin turgor, capillary refill, pulse and blood pressure (including postural BP), fontanelle (babies) |
|
|
3. Measure serum electrolytes
|
•Na+
•K+ •Cl- •HC03- •Anion gap •Urea •Creatinine |
|
|
4. Diagnosis of enteric infections
|
|
|
|
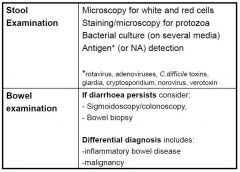
Stool examination…….
|
•
Detects a pathogen in relatively few cases. •Is expensive – the potential range of tests is very large. •Is more useful in enteroinvasive and colonic infection. •Is important for surveillance and control of food-borne diseases. •Is more cost-effective when test algorithms are adopted. |
|
|
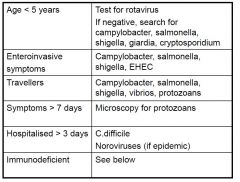
Algorithms for stool examination
|
|
|
|
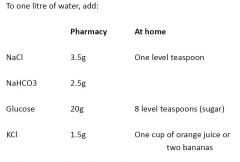
5. Oral rehydration solutions
|
•
Oral is as effective as parenteral therapy (Bangladesh, 1971) –and is much cheaper and safer. “Potentially, the most important medical advance of the century” (Lancet 1987;2;300). •Glucose 2% (or sucrose 4%) much increases intestinal absorption of sodium and water. •Bottled fruit juices and soft drinks contain too much sugar and will make diarrhoea worse. •Solutions can be home made (see www.who.int/child-adolescent-health) or commercial. •Feeding/breast feeding should be continued – but avoid cow’s milk products |
|
|
Oral rehydration solutions
|
|
|
|
7. Drugs for nausea and vomiting
|
•
Dopamine receptor antagonists Act on basal ganglia Are only partially effective May cause dystonia and dyskinesia, especially in the young. Metoclopramide (“Maxolon”) Prochlorperazine (“Stemetil”) (causes drowsiness and hypotension) •5-hydroxytryptamine (5HT3) receptor antagonists Ondansetron (see NEJM, April 20, 2006, p.1698) |
|
|
8. Antidiarrhoeal agents
|
Use in children is discouraged.
Do not use opiates in suspected shigellosis, C.difficile or EHEC colitis •Diphenoxylate + atropine “Lomotil”, “Lofenoxal” PBS •Loperamide “Imodium”, “Gastro-Stop” PBS •Kaolin “Kaomagma” OTC |
|
|
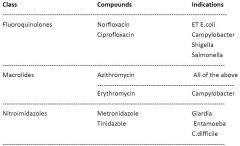
9. Antimicrobials for enteric infections
|
|
|
|
10. Prevention of enteric infections
|
• National surveillance of foodborne pathogens
• Handwashing after defaecation • Hygienic preparation and refrigeration of food • Quality systems in commercial food preparation • Regulated and reticulated water supplies • Pasteurisation of milk • Childhood vaccination (rotavirus, polioviruses, hepatitis A) • Advice and vaccination for travellers |
|
|
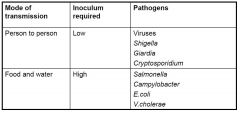
Modes of transmission of enteric pathogens .
|
|
|
|
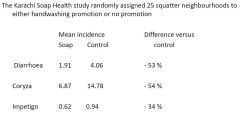
Effect of handwashing on child health
- Karachi Soap Health |
|
|
|
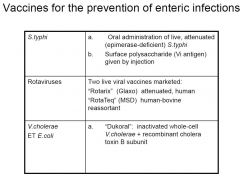
Vaccines for the prevention of enteric infections
|
|
|
|
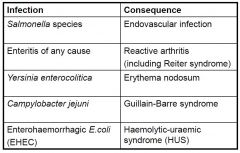
Remote manifestations of enteric infections
|
|
|
|
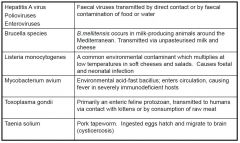
Some systemic infections which follow consumption of contaminated food or water
|
|
|
|
Enteric infections in severe immunodeficiency
|
•The frequency of all enteric infections is increased – therefore, culture stools for all bacterial pathogens.
•Collect multiple stool specimens in fixative for optimal detection of enteric protozoans •If these tests are negative, consider: –Microsporidia –Mycobacterium avium –Cytomegalovirus •Endoscopy and biopsies may be necessary |
|
|
Enteric pathogens which cause persistent diarrhoea (these are all protozoans)
|
•Giardia lamblia
•Cryptosporidium parvum •Entamoeba histolytica •Cyclospora cayetanensis •Isospora belli |
|
|
Diarrhoea
|
Frequent (>3 times/day) and fluid stool usually resulting from the disease of small intestine and involving increased fluid and electrolyte loss
|
|
|
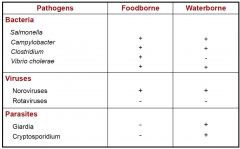
Food or waterborne Pathogens
|
|
|
|
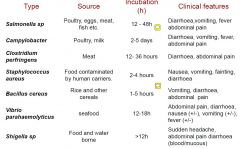
Microbial Food Poisoning
|
the quicker ones are usually pre-formed toxin mediated
Staphylococcus aureus Nasal carriers Egg ,milk dishes Clostridium perfringens Animal faeces Meat and gravy Bacillus cereus Environment Rice Clostridium botulinum Soil Preserved vegetables |
|
|
Case 1 - Gastroenteritis
Within 16 hours of breakfast 2 of a groups of 4 scouts were admitted to hospital with vomiting and diarrhoea. Breakfast consisted of fried fish rissoles and some were still available for inspection. The third scout chose to have sausages. The rissoles had been prepared the night before by the 4th scout, left overnight and lightly fried in the morning. Cues •Vomiting and diarrhoea •3/4 scouts had fish rissoles •2/4 scouts sick •16 hours after breakfast |
- incubation period suggests either bacteria or viral (parasites are long and preformed toxins quicker)
- MacConkey Agar; lactose fermiting +ve for Salmonella sp. |
|
|
Salmonella – Clinical Disease
- disease course |
•Asymptomatic colonisation
–Chronic colonisation in 1-5% of patients •Gastroenteritis –Most common, usually self-limiting •Enteric fever –Invasive enterocolitis –Bacteremia followed by colonisation of gallbladder and then re-infection of intestines (enterohepatic circulation) |
|
|
Invasive Salmonella Infection
|
|
|
|
Enteric Fever Complications
|
•Bacteremia
–Disseminated infection (“rose spots” on skin) –Secondary sites: osteomyelitis, endocarditis, meningitis •Haemorrhage from intestinal ulcers •Perforation leading to peritonitis |
|
|
Case 2 - Gastroenteritis
During an 8 day period 3 of 8 infants in a neonatal intensive-care unit develop diarrhoea. Only one of the 4 staff admits to illness, and her symptoms were minimal. A centralised kitchen facility produces the infants‟ feeds made up according to individual formula. Cues •Diarrhoea (3/8 infants) •Neonatal intensive-care unit, 8 day period of infant sickness •Formula feeds •1/4 staff with minimal symptoms |
- watery stool sample (secretory diarrhoea)
- Rotatvirus |
|
|
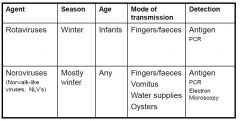
Rotavirus
|
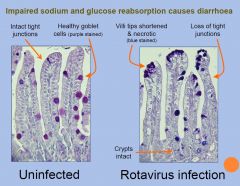
•RNA virus, the most common cause of infant diarrhoea
•Ubiquitous worldwide, 95% of children infected by 3 to 5 years of age •Viruses survive at room temperature, treatment with detergents and acidic pH in a stomach •Acute gastroenteritis, as many as 1010 viral particles per gram of stool may be released during disease |
|
|
Rotatvirus Pathogenicity
|
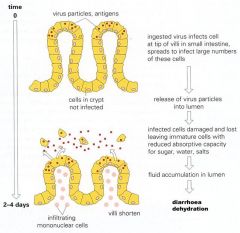
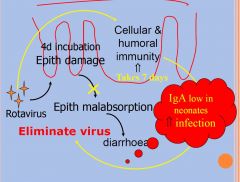
Rotavirus is the most common cause of
severe diarrhea among children and elderly (often in winter) The incubation period for rotavirus disease is approximately 2 days The disease is characterized by vomiting and watery diarrhea for 3 - 8 days; fever and abdominal pain occur frequently. Why? Immunity after infection is incomplete, but repeat infections tend to be less severe than the original infection |
|
|
Case 3 – Pseudomembranous colitis
An elderly in-patient who was treated with antibiotics for RTI complains of fever and severe diarrhoea (>3 times per day, >2 days duration) beginning on the eighth day of treatment and persisting despite cessation of the antibiotic Cues •Fever and severe diarrhoea after eight-day course of antibiotic •Persistent diarrhoea after antibiotic withdrawn •Respiratory tract infection (primary) |
C. Difficile
|
|
|
Case 3 – Pseudomembranous colitis
An elderly in-patient who was treated with antibiotics for RTI complains of fever and severe diarrhoea (>3 times per day, >2 days duration) beginning on the eighth day of treatment and persisting despite cessation of the antibiotic Cues •Fever and severe diarrhoea after eight-day course of antibiotic •Persistent diarrhoea after antibiotic withdrawn •Respiratory tract infection (primary) |
Colitis due to overgrowth of Clostridium difficile
|
|
|
Colitis due to overgrowth of Clostridium difficile
|
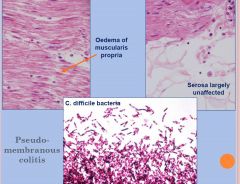
•Anaerobic, spore-forming Gram-positive rod
•Spores resistant to heat, drying and alcohol •Coloniser of the intestines of 5% of healthy adults and ~60% of healthy infants •A normal colonic microflora confers „colonisation resistance‟ against C.difficile •Transmitted within hospital units •through contaminated hands, direct contact or through equipment IMMUNE TO ALCHOL RUB IN HOSIPITIALS •Recurrent disease is common |
|
|
Virulence factors of Clostridium difficile
|

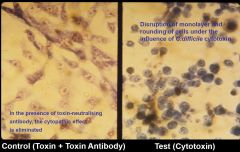
•Enterotoxin (toxin A) indices cytokine production with hypersecretion of fluid; produces haemorrhagic necrosis
•Cytotoxin (toxin B) induces depolymerisation of actin with loss of cellular cytoskeleton •The majority of C.difficile strains are A+B+ |
|
|
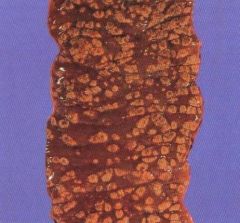
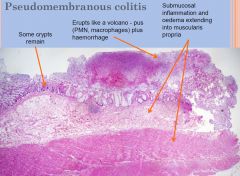
Section of colon of patient with pseudomembraneous colitis. Numerous yellow raised plaques (ie rounded deposits of purulent exudate) superimposed on an erythematous, haemorrhagic mucosa
|
|
|
Laboratory Diagnosis Clostridium difficile
|
•Specimen – faeces
–Small volume, largely blood and mucus (“red currant jelly”) •Bacterial culture –Selective media for anaerobes (CCFA) –~20% of isolates are non-toxigenic/non-pathogenic •Toxin detection (easier and faster than culture) –Tissue culture and cytotoxin neutralisation –Immunoassays (toxins A and B) •Latex agglutination or EIA based –PCR based (toxins A and B) •most sensitive method |
|
|
Cytotoxin neutralisation assay
|
|
|
|
Novel Treatment of reccurrent C.difficile
|
- faceal transplant
|
|
|
Invasive infection
|
•Invasive infection (gastroenteritis, enterocolitis)
• microorganism invades the intestinal mucosa eg osteomyelistis due to salmonella |
|
|
Non-invasive gastroenteritis
|
•Non-invasive gastroenteritis
• microorganism exist in intestinal lumen |
|
|
Toxin-mediated infection
|
•Toxin-mediated infection
• disease is caused by bacterial exotoxin, bacteria do not invade the tissues, in some cases do not even enter the body (botulism, staphylococcal toxin) |
|
|
Prevention of Food Poisoning
|
•Meat dishes should be served hot or should be rapidly refrigerated
•Food safety –Fruit should be washed –Raw food kept away from cooked food –Thaw frozen food fully before cooking •Kitchen hygiene –Hand washing, proper cleaning of cutlery and utensils –Bulk reheating should be avoided –Control vermin (flies, cockroaches etc) –Exclusion of carriers from food-handling •Health inspectors, legislation |
|
|
Mucosa Surface
|
• The most common portal of entry
of microbes per oral INTESTINAL MUCOSA SURFACE... • The surface is about 400 m2 in humans • The most vulnerable site for pathogenic invasion • The balance between immunity and infection (challenge) will determine the outcome |
|
|
Number of anaerobic
bacteria in the gastrointestinal tract |

|
|
|
INTESTINAL DEFENSE
|
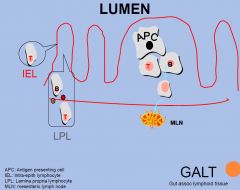
Innate (non-specific immune system)
Barriers: intact epithelium Cellular: Mφ, PMN, Natural Killer cells Humoral: IgA, IgG, IgM and IgE, complements, Acquired Cellular: cytotoxicity Humoral: antigen specific antibody Innate immune system prevents infection Acquired immunity resolves infection (delayed response) |
|
|
Rotatvirus Microscopy
|
|
|
|
Roatvirus Pathogenesis
|
|
|
|
Dx and Tx of rotavirus
|
Diagnosis may be made by rapid antigen
detection of rotavirus in stool specimens Strains may be further characterized by enzyme immunoassay or RT-PCR, but not commonly done Approach to treatment: rehydration and supportive measures; may require IV due to villi destruction |
|
|
Pseudomembranous colitis
Mortality and morbidity |
While most patients with C difficile colitis
Pseudomembranous colitis recover without specific therapy, symptoms may be prolonged and debilitating. C difficile associated diarrhea can be a serious condition with a mortality rate as high as 25% in elderly patients who are frail (often due to toxic megacolon). Mortality rates have also risen over the past decade and reflect an increase in admissions and the virulence for C difficile More common in elderly people, and old age may promote susceptibility to colonization and disease |
|
|
Toxic Megacolon
|
Toxic megacolon (megacolon toxicum) is an acute form of colonic distension.[1] It is characterized by a very dilated colon (megacolon), accompanied by abdominal distension (bloating), and sometimes fever, abdominal pain, or shock.
|
|
|
Clinical Presentation of C. Difficle
|
Most patients develop diarrhea during or shortly
after starting antibiotics. 30% of patients may have already completed their Pseudomembranous colitis antibiotics [symptoms may develop up to 10 weeks later]. Symptoms often include the following: Mild-to-moderate watery diarrhea that is rarely bloody Cramping abdominal pain Anorexia Malaise Fever, especially in more severe cases Dehydration Lower abdominal tenderness Rebound tenderness - raises the possibility of colonic perforation and peritonitis |
|
|
Pseudomembranous colitis Pathology (microscopic)
|
|
|
|
Pseudomembranous colitis Pathology (microscopic - layers)
|
|
|
|
Pseudomembranous colitis Pathogenesis
|
|
|
|
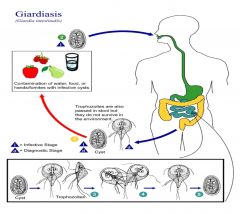
Giardia Microscopic Pathology
|

Giardia lamblia is a flagellated protozoan, a noninvasive
pathogen, flat or sickle-shaped or pear shaped. Number of outbreaks in NSW in the past (contaminated food/water) Can be as low as 10 cysts per infection. Cysts are stable. IgA & IL-6 are important in clearance of Giardia. Immune compromised, malnourished are often infected. Giardia can evade immune clearance through continuous modification of the major surface antigen. Causes watery diarrhoea worldwide but the mechanisms of pathogenicity and the major host defenses against Giardia infection are not well characterized... - common in blue moutains waters |
|
|
Intestinal
Spirochaetosis (IS) |
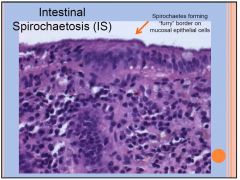
HUMAN INTESTINAL SPIROCHAETOSIS (IS)
Defined at histological biopsy by the presence of spirochetal microorganisms attached to the apical cell membrane of the colorectal epithelium. Intestinal spirochetes are heterogeneous group of bacteria Prevalence rates low where living standards high HIV-infected and children at high risk of colonization. Clinical significance of individual colonization unclear Spirochete invasion beyond epithelium may cause GI symptoms (diarrhoea +/- blood; responds to metronidazole). If no invasion usually asymptomatic (but can be symptomatic ?Why?). Rare cases of spirochetemia and multiple organ failure can occur in critically ill patients with IS. |
|
|
Strongyloides
threadworm |
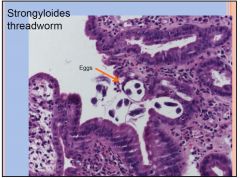
• From contaminated water; larvae penetrates skin>lung>intestine.
• They can autoinfection in immune compromised patients, e.g HIV, persistent life time • Accompanied by peripheral eosinophilia |
|
|
CMV
(stomach) |
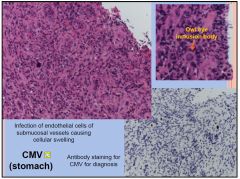
Massive inflammation
plus ulceration Cytomegalovirus infection is a common viral illness. Infection in children and adults is usually without symptoms but occasionally, symptoms similar to glandular fever can occur. Immunocompromised more at risk. Most severe form of the disease occurs in infants born to mothers who became infected for the first time while pregnant. Symptoms: Healthy people often have no symptoms. Small number of people will experience a glandular fever like illness with a sore throat, aches and pains and sore glands. Symptoms usually last two to three weeks. |
|
|
HELICOBACTER
IN STOMACH |
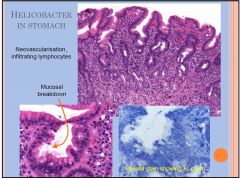
Increased IEL and LPL
50% of world population are infected; 80% of infected individuals are asymptomatic Detected by endoscopic biopsy; screened by the carbon urea breath test (patient drinks 14C-labelled urea, bacterium metabolizes to CO2, detected in the breath) Associated with most peptic ulcers – infection weakens the protective lining of stomach allowing acid to erode the mucosal epithelium and cause ulceration Associated with increased risk of stomach cancer |
|
|
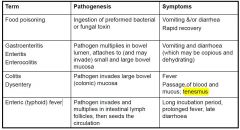
Pathogenesis and Sx of these clinical terms
Food poisoning Gastroenteritis Enteritis Enterocolitis Colitis Dysentery Enteric (typhoid) fever |
|
|
|
Tenesmus
|
A. Rectal tenesmus - a clinical sign, where there is a feeling of constantly needing to pass stools, despite an empty colon. When the word "tenesmus" is used by itself, this is usually what is meant.
B. Vesical tenesmus - a clinical sign, where there is a feeling of constantly need to urinate, despite an empty bladder. |
|
|
Function and flora of the gut
|
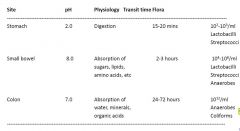
95% of the dry weight of faeces is bacteria
|
|
|
Food Poisoning
|
•
follows ingestion of pre-formed toxin. •has a rapid onset*, with symptoms clearly related to ingestion of contaminated food. •may be epidemic when food is catered. • causes vomiting and/or diarrhoea*. Fever is slight or absent. •is best diagnosed by culturing the food. •is treated symptomatically •DD includes other causes of sudden onset of vomiting, especially vestibular disease * Except botulism |
|
|
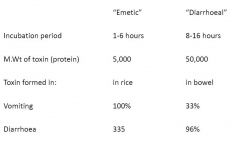
Enterotoxins of Staphylococcus aureus
|
• are proteins secreted by S.aureus
• resist hydrolysis by gastric and jejunal enzymes • are stable to 100oC for 30 minutes • are strong inducers of cytokine formation e.g., IL1. • cause nausea and vomiting following peripheral stimulation of the vomiting centre • induce symptoms within 1-6 hours of ingestion, with a duration of less than 12 hours |
|
|
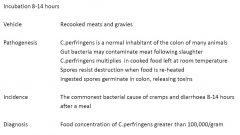
Clostridial food poisoning
|
|
|
|
Two types of Bacillus cereus food poisoning
|
|
|
|
Some non-microbial causes of food poisoning
|
Heavy metals: Nausea and vomiting
Mutant zucchinis: Cramps and vomiting Reef fish: Ciguatera poisoning Mushrooms: Hallucinations, hepatic necrosis Blue-green algae: “Barcoo spews” Methanol: Metabolic acidosis |
|
|
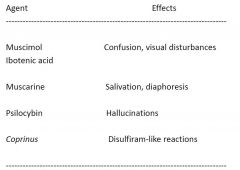
Short-acting mushroom toxins
|
|
|
|
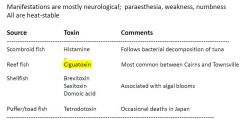
Marine biotoxins
|
|
|
|
Ciguatera poisoning
|
•
Ciguatoxins are heat-stable, lipid-soluble polyethers which accumulate in the muscles of tropical fish, especially large coral trout and Spanish mackerel. • Most Australian disease follows consumption of reef fish caught on the Queensland coast between Cairns and Mackay. • Usually begins with vomiting, diarrhoea and abdominal pain. • Followed by paraesthesia and dysaesthesia in the arms, legs and perioral regions, as well as myalgia, muscle cramps and weakness. •Neurological symptoms resolve within weeks but may recur during periods of exercise or alcohol consumption. |
|
|
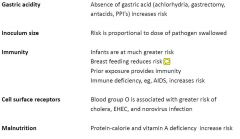
Factors influencing frequency of disease
|
|
|
|
Two common causes of viral enteritis
|
|
|
|
Norovirus infection
|
Incubation period: 24-48 hours
Duration of illness: 12-60 hours Vomiting in > 50% of cases Outbreaks are more frequent: •in winter •in closed communities, eg, cruise ships, barracks •in hospitals, nursing homes* * spread is enhanced by immobility, incontinence, dementia. Spread to staff is the rule |
|
|
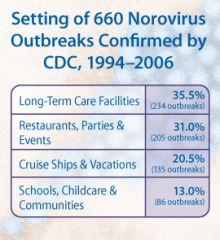
Outbreaks of norovirus more likely in...
|
|
|
|
Oysters as a source of norovirus infection
|
•Oysters are filter feeders and therefore concentrate water-borne viruses
•Oyster beds in bays and estuaries may be contaminated with sewage from nearby boats and dwellings •Without expensive molecular techniques, norovirus contamination of oysters is difficult to detect •Oysters are usually eaten raw or lightly cooked (noroviruses are relatively heat stable) •International transportation of frozen oyster meat may lead to widespread outbreaks of disease (as in Australia, Clin Infect Dis, 2007;44:1026) |
|
|
Norovirus Immunisation
|
•
Short lived immunity, different serotypes a challenge for vaccine development • Also not cell culturable • Virus- like particles are immunogenic when given to human volunteers serum IgG, mucosal IgA, cellular responses • Murine strains have been cultured ? Possibility of antivirals? |
|
|
Calicivirus
|
The Caliciviridae family are a family of viruses, members of Class IV of the Baltimore scheme. They are positive-sense, single stranded RNA which is non-segmented.
Calicivirus infections commonly cause acute gastroenteritis, which is the inflammation of the stomach and intestines (e.g. the Norwalk Virus). Symptoms can include vomiting and diarrhea. |
|
|
Calicivirus
•Prevention |
preventing contamination of water, food
especially restricting symptomatic food handlers norovirus is resistant to freezing, heating and standard cleaning solutions use chlorine bleach 1:50 to 1:10 dilution of house-hold bleach (1000 to 5000 ppm) |
|
|
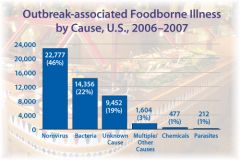
Most common foodborne illness
|
|
|
|
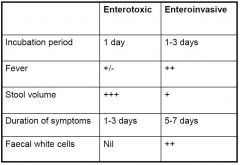
Clinical features of two types of bacterial enteritis
|
|
|
|
Toxigenic Diarrhoea
|
|
|
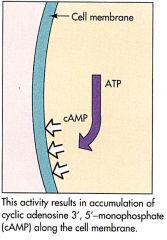
Step 1 Pathogenisis
Cholera |
|
|
|
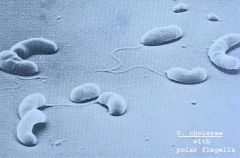
Cholera
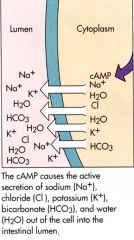
Step 2 |
|
|
|
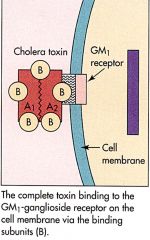
Cholera Step 3
|
|
|
|
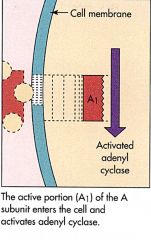
Cholera Step 4
|
|
|

|
father of epidemiology
- John Snow |
|
|
Culturing Cholera
|

requires special agar
- anytime u see rice water stools think CHOLERA |
|
|
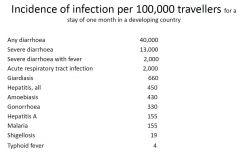
Incidence of infection per 100,000 travellers for a stay of one month in a developing country
|
|
|
|
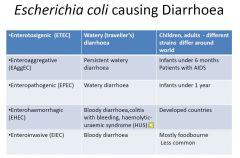
The different types of E.Coli
|
|
|
|
Enteropathogenic E.Coli in the gut
|

on gut surface
- everyone has E.Coli so hard to test |
|
|
Invasive Diarrhoea
|
|
|
|
Two common causes of protozoan enteropathy
|
Giardia intestinalis (previously G.lamblia)
– occurs in infants (& their parents) and travellers. - Slow onset, steatorrhoea, weight loss. - Relapsing infections in patients with IgA deficiency. - Responds to nitroimidazoles. Cryptosporidium parvum – in Australia, occurs mostly as an acute self-limiting illness in infants. -May contaminate poorly filtered water supplies (cysts survive chlorine) -Summer time epidemics associated with swimming pools. -Persistent infection in patients with AIDS -Poor response to antimicrobials. |
|
|
Giardia Path 1
|
|
|
|
Giardia Path 2
|
|
|
|
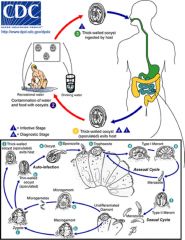
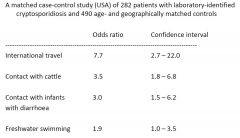
Risk factors for spread of cryptosporidiosis
|
|
|
|
Types of diarrhoea
|
•acute watery diarrhoea – lasts several hours or days, and includes cholera;
•acute bloody diarrhoea – also called dysentery; and •persistent diarrhoea – lasts 14 days or longer. |
|
|
Signs and symptoms of dehydration
|

|
|
|
Acute diarrhoea (infectious)
|
Viral
• rotavirus 33%(11-71%) regardless of geography, economy, methodology • enteric adenoviruses, small round structured viruses, caliciviruses, astroviruses, Norwalk Bacterial • Campylobacter, Salmonella, Shigella, Yersinia and Vibrio species • E.coli (EPEC, EIEC, EHEC, ETEC, EAEC) • Food poisoning - Staph aureus, Listeria Protozoan - Giardia lamblia Parasite - Cryptosporidium |
|
|
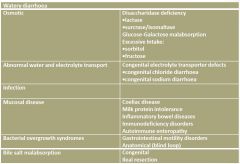
Watery diarrhoea
|
|
|
|
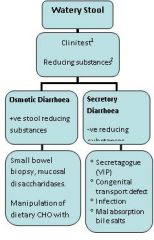
Assessment of watery stools
|
•
1. Stool collection must be fresh as stool osmolality increases after excretion due to continued bacterial fermentation of faecal carbohydrates • Breast fed Infants can exhibit up to ½% reducing substances •2.Sucrose is a non reducing sugar, and not measurable as a reducing substance unless hydrolysed by boiling or acid •Osmotic gap in stool fluid= Serum osmolality (280) – {2X [Na] + [K]}. |
|
|
Osmotic Diarrhoea (osmotic gap >100)
|
•
non-absorbed osmotically active nutrients in the gut lumen results in osmotic retardation of water absorption, leading to watery diarrhoea. • Osmotically active compounds are usually low-molecular-weight compounds such as monosaccharides and disaccharides. • Osmotic diarrhoea is usually due to maldigestion and/or malabsorption of carbohydrates • can be caused by the ingestion of laxatives such as sorbitol or MgCl2. • Unabsorbed carbohydrate present in the lumen of the large bowel is fermented to short chain fatty acids such as butyrate (acidic stools can cause perianal excoriation) • The colon can absorb the anionic forms of these acids in exchange for bicarbonate, causing a mild hyperchloraemic acidosis. |
|
|
Stool osmotic Gap
|
Stool osmotic gap is a calculation performed to distinguish among different causes of diarrhea.
A low stool osmolic gap can imply secretory diarrhea, while a high gap can imply osmotic diarrhea.[1] It is calculated with the equation 290 − 2 * (stool Na + stool K).[2] The 290 is the value of the stool osmolality. The stool osmolality is usually not directly measured, and is often given a constant in the range of 290 to 300.[3] A normal gap is less than 50.[4] High osmotic gap causes of osmotic diarrhea include celiac sprue, chronic pancreatitis, lactase deficiency, lactulose, laxative use/abuse, and Whipple's disease. Low osmotic gap causes of secretory diarrhea include toxin-mediated causes (cholera, enterotoxigenic strains of E. coli) and secretagogues such as vasoactive intestinal peptide (from a VIPoma, for example). Uncommon causes include gastrinoma, medullary thyroid carcinoma (which produces excess calcitonin), factitious diarrhea from laxative abuse[5] and villous adenoma. |
|
|
Osmotic Diarrhoea workup
|
•
Cannot malabsorb a nutrient that has not been ingested • useful to obtain a dietary history in patients suspected of osmotic diarrhoea • ascertain the nature of the carbohydrates being ingested • the age of introduction of the carbohydrate • compare with the age of onset of symptoms • For example, the onset of osmotic diarrhoea seen with the introduction of fruit into the diet suggests the diagnosis of congenital sucrase–isomaltase deficiency • Autosomal recessive, presents with weight loss, diarrhoea, bloating and flatus, requires dietary management. |
|
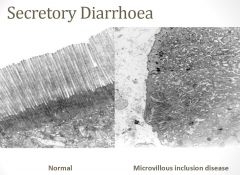
Secretory diarrhoea (osmotic gap <50)
|
•
Electrolytes are absorbed by a variety of active transport or passive transport processes. • Anions such as chloride and bicarbonate can be absorbed or actively secreted. • This varies according to the region of small or large intestine. • Regulation of gastrointestinal fluid and electrolyte transport is closely integrated by humoral and neural factors involved in fluid and electrolyte homeostasis. • Abnormal fluid and electrolyte transport can be due to inherited defects in specific electrolyte transporters, but more commonly it is due to mucosal damage or inflammation. |
|
|
CONGENITAL Secretory diarrhoea
|
•
Congenital sodium diarrhoea and congenital chloride diarrhoea are rare inherited disorders of Na/H exchange and Cl/HCO exchange, respectively. They cause: • • diarrhoea in utero which results in polyhydramnios • • profuse diarrhoea, obvious from birth • • systemic electrolyte disturbances. |
|
|
Acquired Secretory Diarrhoea
|
Acquired
• Isolated water and salt malabsorption is very rare in childhood in the developed world. However, defective salt and water transport can contribute to diarrhoea in: • • disorders which damage or inflame the mucosa of small or large intestine • • bile salt malabsorption (bile acids irritate the colonic mucosa and act as potent stimulants of secretion). • Excessive salt and water loss in the stool may lead to dehydration and electrolyte disturbances. Treatment may require salt and water replacement in addition to treatment of the underlying disease. |
|
|
Secretory vs Osmotic Diarrhoea
|
Secretory
Secretory diarrhea means that there is an increase in the active secretion, or there is an inhibition of absorption. There is little to no structural damage. The most common cause of this type of diarrhea is a cholera toxin that stimulates the secretion of anions, especially chloride ions. Therefore, to maintain a charge balance in the lumen, sodium is carried with it, along with water. In this type of diarrhea intestinal fluid secretion is isotonic with plasma even during fasting.[5] It continues even when there is no oral food intake. Osmotic Osmotic diarrhea occurs when too much water is drawn into the bowels. If a person drinks solutions with excessive sugar or excessive salt, these can draw water from the body into the bowel and cause osmotic diarrhea.[6] Osmotic diarrhea can also be the result of maldigestion (e.g., pancreatic disease or Coeliac disease), in which the nutrients are left in the lumen to pull in water. Or it can be caused by osmotic laxatives (which work to alleviate constipation by drawing water into the bowels). In healthy individuals, too much magnesium or vitamin C or undigested lactose can produce osmotic diarrhea and distention of the bowel. A person who has lactose intolerance can have difficulty absorbing lactose after an extraordinarily high intake of dairy products. In persons who have fructose malabsorption, excess fructose intake can also cause diarrhea. High-fructose foods that also have a high glucose content are more absorbable and less likely to cause diarrhea. Sugar alcohols such as sorbitol (often found in sugar-free foods) are difficult for the body to absorb and, in large amounts, may lead to osmotic diarrhea.[5] In most of these cases, osmotic diarrhea stops when offending agent (e.g. milk, sorbitol) is stopped. |
|
|
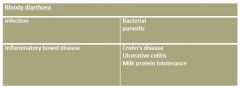
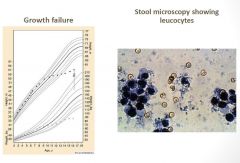
Bloody Diarrhoea
|
•
Blood is not always obvious in the stool. • Presence of leukocytes on stool microscopy indicates the presence of colitis. • Malabsorption of fluid and electrolytes by inflamed colonic mucosa is a major factor contributing to diarrhoea. • Malabsorption of nutrients is uncommon in milk colitis and inflammatory bowel disease. • Excessive blood and protein loss from the inflamed intestinal mucosa can cause iron deficiency anaemia and hypoproteinaemic oedema. • This is called protein-losing enteropathy; this can be assessed by measuring stool alpha 1 antitrypsin levels. |
|

|
Crohn’s Disease
|
|
|
Crohn’s Disease
|