Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
14 Cards in this Set
- Front
- Back
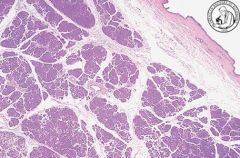
Describe the normal anatomy of the Pancreas
What are two major functions of this organ? |
Divided into acini (clusters of exocrine cells)= stain eosinophilic/basophilic
Endocrine (insulin, glucagon, somatostatin) and Exocrine (zymogen granules). Acini secrete enzyme into ductules. |
|
|
What happens when there's failure of fusion of the dorsal and ventral primordia ( during pancreatic development)?
What congenital anomaly results from ectopic pancreatic tissue resulting in an outpouching of the small intestine wall? |
The major duct of wirsung becomes too small and the santorini duct get's overwhelmed --> release of enzymes into parenchyma --> chronic pancreatitis
Meckel's diverticulum |
|
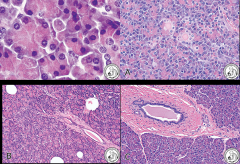
Is this chronic or acute pancreatitis?
What does this syndrome get confused with? Why is it important to diagnose this? |
Chronic pancreatitis- this is the Lymphoplasmacytic sclerosis variant (thought to be autoimmune). Important to diagnose because can be treated with steroids
Clinically mimics pancreatic cancer on radiology (forms mass of inflammatory cell- plasma cell- infiltrate on pancreatic duct). |
|
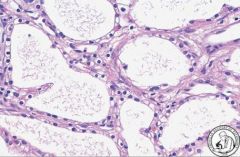
Is this a true cyst? How can you tell?
Autosomal dominant congenital cysts in the pancreas, kidneys, and liver are associated with what disease? |
No- it's a Pancreatic Pseudocyst. Does not have eptihelial lining. Just lined by fibrous tissue (granulation tissue), surrounding the fluid produced by inflammation.
Von Hippel Lindau disease |
|

Is this cystic or solid? Benign or malignant?
What demographic is more commonly seen in? |
Cystic neoplasm- almost always BENIGN. Note the small microcysts and central scars characteristic of this conditioon.
F >>M, older generation "more serious"...'serous' |
|
What type of pancreatic neoplasm is this? What do the cells contain?
What is the appropriate treatment? |
Serous cystadenoma- note the microcysts lined by clear, serous cells rich in GLYCOGEN.
Since it's benign- cure by surgery. |
|

Cystic or Solid? What demographic is this most common in?
In what part of the pancreas does this typically arise? |
Cystic- it can be associated with adenocarcinomas so make sure to screen carefully.
Typically arises in BODY or TAIL. Almost always seen in Females (characterized by ovarian type stroma and mucous type epithelium). |
|

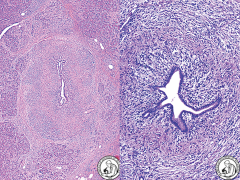
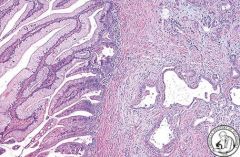
What type of neoplasm is this (cystic or solid)?
How can you distinguish it from a Mucinous Cystadenoma? |
Cystic. It is an Intraductal Papillary Mucinous Neoplasm (IPMN). Note the papillary projections into lumen and dilation of duct (because it is being obstructed).
Unlike mucinous 1- no ovarian type stroma 2- involves LARGER pancreatic duct *note M >F |
|
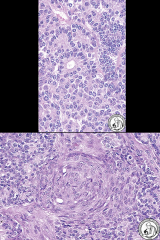
What type of pancreatic neoplasm is this?
|
Intraductal Papillary Mucinous Neoplasm (you can tell because there are papilla lined by mucinous epithelium)
|
|
|
What is the mortality rate in Pancreatic Carcinoma? Why?
What are some risk factors? |
High mortality rate (<5% survive beyond 5 years). Not good screening method. Doesn't tend to manifest till late (when there's invasion).
Risk factors= CIGARETTE smoking, Chronic pancreatitis, DM, Familial history, BRCA2 (in Ashkenazi Jews) |
|
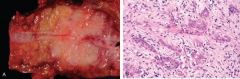
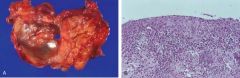
What are some clinical features of the cancer shown above?
What is Trousseau's sign? |
Pancreatic cancer- see the dense fibrous tumor obstructing duct (desmoplastic response).
Pain is 1st symptom. Obstructive jaundice. Weight loss, fatigue, malaise --> " B symptoms" Trousseau's sign = migratory thrombophlebitis (associated with malignancy) |
|
|
An elderly patient comes in with diabetes melitus, what is something that you should DEFINITELY be concerned about?
|
Pancreatic Carcinoma!
DM is a risk for pancreatic carcinoma. But pancreatic cancer can also manifest as new onset DM. |
|
|
Elevation of CEA and CA19-9 are suggestive of?
What are precursor lesions of pancreatic carcinoma called? |
CEA and CA19-9 = tumor marker (elevated in pancreatic cancer)
Precursor lesions (akin to tubular adenoma) --> PanINs (pancreatic intraepithelial neoplasias). They progress in stepwise mutation to pancreatic adenocarcinoma. |
|
What are the most common mutations that lead to pancreatic cancer?
What is the type of pancreatic cancer? |
Most common = KRAS and P16 (tumor suppressor gene).
Also can see SMAD4 and p53 but not as common. Pancreatoblastoma (lots of small blue cells, blasts --> seen in children. Better prognosis than pancreatic ductal CA). |