Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
78 Cards in this Set
- Front
- Back
|
What are the special challenges to the immune system in the GI tract?
|
- Tolerance to food antigens
- Tolerance to microbiota but responsiveness to pathogens - Enormous surface area |
|
|
What are the special anatomic features of the immune system in the GI tract?
|
- Tonsils
- Peyer's patches - Lamina propria follicles |
|
|
What are the specialized cells / molecules in the immune system in the GI tract? Functions?
|
- Epithelial cells: mucus secretion
- M cells: luminal sampling - Paneth cells: defensin (antimicrobial) secretion - Secretory IgA, IgM: neutralization - DC subsets: luminal sampling |
|
|
What are the special challenges to the immune system in the respiratory system?
|
Exposure to a mix of airborne pathogens and innocuous microbes and particles
|
|
|
What are the special anatomic features of the immune system in the respiratory system?
|
Adenoids
|
|
|
What are the specialized cells / molecules in the immune system in the respiratory system? Functions?
|
- Ciliated epithelial cells: mucus and defensin secretion
- Secretory IgA, IgM, IgG: neutralization |
|
|
What are the special challenges to the immune system in the cutaneous immune system?
|
Large surface area
|
|
|
What are the special anatomic features of the immune system in the cutaneous immune system?
|
Keratinizing stratified epithelium
|
|
|
What are the specialized cells / molecules in the immune system in the cutaneous immune system? Functions?
|
- Keratinocyte: secretes keratin, cytokines, defensin
- Langerhans cells - DC subsets |
|
|
What is the structure that is found at the crossroads of the GI tract and respiratory tract?
|

Waldeyer's Ring
|
|
|
What are the components of Waldeyer's Ring?
|

- Palatine tonsils (most superior)
- Tubal tonsils - Adenoids - Lingual tonsil (most inferior) |
|
|
What is found within the tonsils of Waldeyer's ring?
|
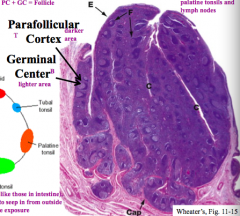
Follicles: consists of Parafollicular Cortex (darker area) and Germinal Center (lighter area)
|
|
|
What is found in the Germinal Center of a follicle?
|
B cells
|
|
|
What is found in the Parafollicular Cortex of a follicle?
|
T cells
|
|
|
What are the characteristics of the mucosal immunity in the esophagus?
|
- Has some mucosal immunity but this tends to be a fairly sterile environment (no endogenous bacteria)
- No large grouping of follicles |
|
|
What are the characteristics of the mucosal immunity in the stomach?
|
- Similar to esophagus
- Acid is its main defense against bacteria - H. pylori is the only bacteria that can really colonize here |
|
|
What are the characteristics of the mucosal immunity in the small and large intestines?
|
Much more developed because the transit times are slower so there is a greater microbiota
|
|
|
What kind of epithelium is found in the oral cavity?
|
Stratified squamous, partially keratinized
|
|
|
What kind of epithelium is found in the esophagus?
|
Stratified squamous, non-keratinized
|
|
|
What kind of epithelium is found in the stomach?
|
Simple columnar epithelium with goblet cells
|
|
|
What kind of epithelium is found in the small intestine?
|
Simple columnar epithelium with goblet cells, crypts, and villi
|
|
|
What kind of epithelium is found in the colon?
|
Simple columnar epithelium with crypts but no villi
|
|
|
What kind of epithelium is found in the anus?
|
Non-keratinized stratified epithelium
|
|
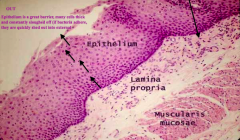
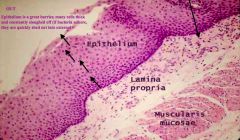
Which part of the GI tract does this represent? How does it function for mucosal immunity?
|
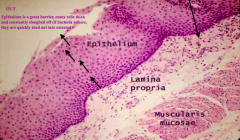
Esophagus:
- Epithelium is stratified squamous and constantly sloughing off - If bacteria adhere to epithelium, they are quickly sloughed before they can get in - Purple dots in Lamina Propria are neutrophils, macrophages, and lymphocytes (physiologic inflammation to be ready for an infection) |
|

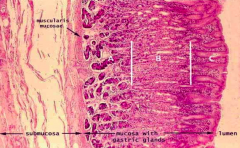
Which part of the GI tract does this represent? How does it function for mucosal immunity?
|
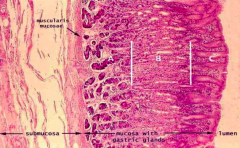
Stomach:
- Immune cells are littered throughout the lamina propria (a lot more of these immune cells near the epithelial surface and less near the submucosal surface) |
|
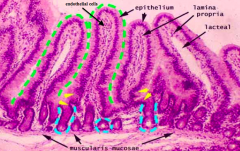
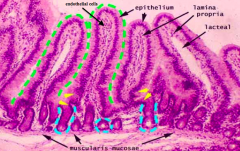
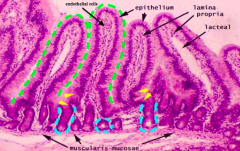
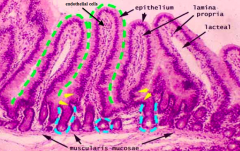
Which part of the GI tract does this represent? How does it function for mucosal immunity?
|
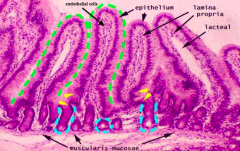
Small Intestine:
- Increasing accumulation of immune cells within lamina propria - Slower migration patterns / less propulsive contractions, so there are more bacteria in this environment so need more immune cells - Immune cells found in lamina propria in the villi |
|
What would a sign of a diseased/infected specimen?
|
If you started seeing immune cells in the submucosal space that means they are proliferating and spilling out of the lamina propria
|
|
|
What is the first place that the arterioles/venules and lacteals drain from the villi in the small intestine?
|
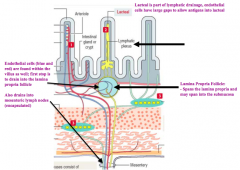
Lamina Propria Follicle: spans the lamina propria and may span into the submucosa
Eventually drains into the mesenteric lymph nodes |
|
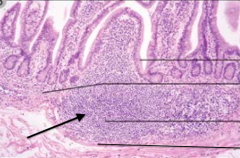
What is the arrow pointing out?
|
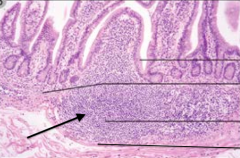
Lamina Propria Follicle (contains B and T cells)
|
|
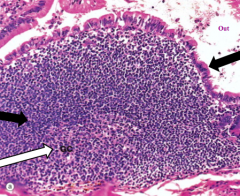
What is this an image of in the ileum?
|
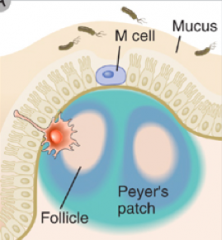
Peyer's Patch
- Left black arrow: Parafollicular cortex (darker, contains T cells) - White arrow: Germinal center (lighter, contains B cells) - Right black arrow: Follicle Associated Epithelium (in close association with the Peyer's patch so that the bacteria can go directly into the T and B cell rich area) |
|
|
What cells channel bacteria into the Peyer's patches?
|
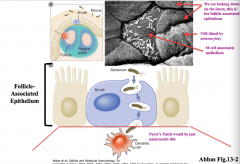
M cells
|
|
|
What kind of receptors recognize free antigens?
What kind of receptors recognize cell-associated antigens? |
- Free antigens: B cell receptors
- Cell-associated antigens: T cell receptors |
|
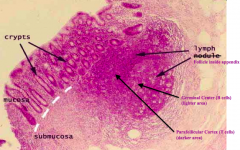
Which part of the GI tract does this represent? How does it function for mucosal immunity?
|
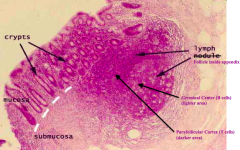
AppendixAppendix
- Has a colonic like epithelial surface - Crypts but no villi - Immune cells in the lamina propria - Lymph follicles underneath epithelium contains germinal center (light w/ B cells) and parafollicular cortex (dark w/ T cells) |
|

Which part of the GI tract does this represent? How does it function for mucosal immunity?
|

Colon:
- Crypts but no villi - Basal level of immune cells in lamina propria - Physiologically inflamed immune tissue (not infected) |
|
|
How do immune cells move into tissues?
|
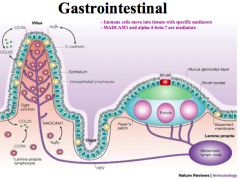
Mediators:
- MADCAM1 - α4β7 |
|
|
What are the barrier / structural cells of the mucosal immune system?
|
Epithelial cells
|
|
|
What are the innate immune cells of the mucosa?
|
- Dendritic cells
- Macrophages - NK cells - Neutrophils - Eosinophils - Mast cells |
|
|
What are the adaptive immune cells of the mucosa?
|
T cells:
- CD4: Th1, Th2, Th17 - CD8 B cells: - IgA producing |
|
|
What molecules help maintain the tight junctions between epithelial cells?
|
- Claudin
- Occludin - E-cadherin - Tight junctions - Adherens junctions |
|
|
What Antigen Presenting Cells contribute to mucosal immunity?
|
- Dendritic cells
- Activated macrophages - Follicular dendritic cells (only found in germinal centers) |
|
|
What are the two responses an intestinal dendritic cell can have? How do you know which is happening?
|
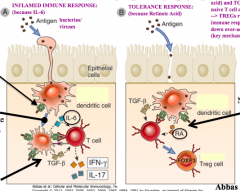
- Inflamed immune response - presence of IL-6
- Tolerance response - presence of Retinoic Acid |
|
|
What do TLR receptors that recognize antigen extracellularly release?
|
NFkB
|
|
|
What do TLR receptors that recognize antigen intracellularly release?
|
IFN
|
|
|
What "gut-homing" molecules are found on IgA-secreting B cells and effector T cells, to help these cells re-circulate back to the gut mucosa?
|

1) α4β7 integrin (recognizes MadCAM in GI endothelium)
2) CCR9 (recognizes CCL25 - mucosal trafficking signal) |
|
|
What kind of cells is α4β7 integrin found on? What is its function on these cells?
|

- Found on IgA secreting B cells and effector T cells trying to get to the gut
- Binds to MadCAM (mucosal addressin) on gut endothelial cells |
|
|
What kind of cells is CCR9 found on? What is its function on these cells?
|

- Found on IgA secreting B cells and effector T cells trying to get to the gut
- Binds to CCL25 - a mucosal trafficking signal to help these cells return to gut |
|
|
What can Dendritic cells in Peyer's patches or mesenteric lymph nodes present? How?
|
Retinoic Acid (RA) from dietary vitamin A through expression of retinal dehydrogenases
|
|
|
Why is there elevated retinoic acid in gut tissues?
|
Intestinal epithelial cells also express retinal dehydrogenases
|
|
|
How do IgA-secreting B cells and effector T cells get back to the gut mucosa?
|

- Follow the gradient of CCL25 (mucosal trafficking signal which is recognized by CCR) on these cells)
- Once it gets to the GI, the α4β7 being expressed on these cells binds to MadCAM on the GI endothelium |
|
|
What cytokines are produced by Th1 cells? What are these defending against? Role in disease?
|

- Release IFN-γ
- Defending against intracellular microbes - Involved in immune-mediated chronic inflammatory diseases (eg, IBD and infectious enterocolitis) (often auto-immune) |
|
|
What cytokines are produced by Th2 cells? What are these defending against? Role in disease?
|

- Release IL-4, IL-5, and IL-13
- Defending against helminthic parasites - Involved in allergies |
|
|
What cytokines are produced by Th17 cells? What are these defending against? Role in disease?
|

- Release IL-17 and chemokines
- Defending against extracellular bacteria and fungi - Involved in immune-mediated chronic inflammatory diseases (often autoimmune) |
|
|
What is the function of complement in the GI?
|
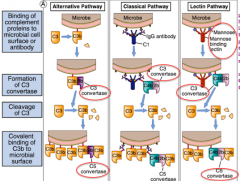
- System of serum and cell surface proteins that interact with one another and other molecules of the immune response to generate effectors of innate and adaptive immune systems
- All pathways lead to C3 convertase→ C5 convertase → MAC complex on microbial surface |
|
|
How do plasma cells class switch in the gut? What does it require?
|
Two mechanisms:
- T-dependent - T-independent - Requires soluble and membrane proteins |
|
|
What is the T-dependent mechanism of class switching in the gut?
|
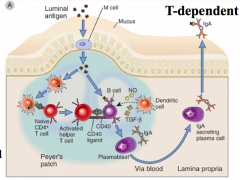
- DCs in Peyer's patch present Ag and activate naive T cells to Th1 cells
- CD40L on Th1 cells and *TGFβ* from DCs activates naive B cells |
|
|
What is the T-independent mechanism of class switching in the gut?
|
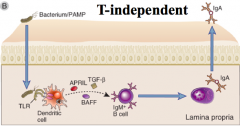
- TLRs on DC stimulates release of TGFβ, APRIL, BAFF with IL6, and Retinoic Acid
* Combination of TGF-β and Retinoic Acid converts naive B cells into an IgA producing plasma cell |
|
|
What is the most prevalent immunoglobulin in the gut?
|
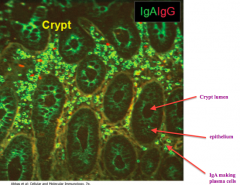
IgA (green)
|
|
|
How do IgA polymerize?
|
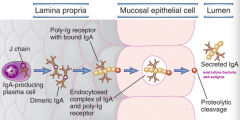
- IgA link together via J chain which links to Poly-Ig receptor expressed on the basolateral surface of the mucosal epithelial cells
- This allows IgA produced by plasma cells to move from inside of the body to the gut lumen |
|
|
What is an immunogen?
|
An antigen that induces an immune response
|
|
|
What is an antigen?
|
A molecule that binds to (is recognized) by antibody or T cells
|
|
|
What factors make a protein more immunogenic (induce a larger immune response)?
|
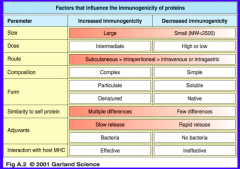
- Larger size
- Intermediate dose (high or low has decreased immunogenicity) - Subcutaneous dosage > Intraperitoneal > IV or Intragastric - Complex composition - Particulate and denatured - Many differences compared to self protein - Slow release adjuvants / bacteria - Effective interaction w/ host MHC |
|
|
What factors make a protein less immunogenic (induce a smaller immune response)?
|
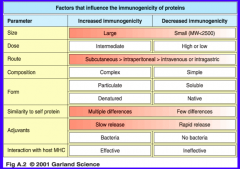
- Smaller size (MW<2500)
- High or low dose - Intragastric or IV route - Simple composition - Soluble and native - Few differences compared to self protein - Rapid release adjuvants / no bacteria - Ineffective interaction w/ host MHC |
|
|
What is hypersensitivity?
|
Excessive or aberrant immune response following challenge with antigen
|
|
|
What causes hypersensitivity?
|
1. Dysregulated or uncontrolled response to foreign antigens resulting in tissue damage and injury
2. Failure of self-tolerance followed by immune responses directed against self-antigens (auto-immune) |
|
|
What are the types of hypersensitivity reactions? Type of immune response?
|
- I: IgE response (immediate)
- II: IgG/IgM response - III: immune complex mediated - IV: T cell mediated |
|
|
What type of hypersensitivity is Type I? Pathological immune mechanism? Mechanism of tissue injury and disease?
|
- Immediate hypersensitivity
- IgE mediated - Mast cells and eosinophils and their mediators (vasoactive amines, lipids, cytokines) cause tissue injury and disease (inflammation) |
|
|
What type of hypersensitivity is Type II? Pathological immune mechanism? Mechanism of tissue injury and disease?
|
- Antibody mediated: IgM and IgG
- Opsonization and phagocytosis, complement and Fc recruitment of leukocytes |
|
|
What type of hypersensitivity is Type III? Pathological immune mechanism? Mechanism of tissue injury and disease?
|
- Immune complex mediated
- Complement and Fc recruitment of leukocytes causes tissue injury and disease |
|
|
What type of hypersensitivity is Type IV? Pathological immune mechanism? Mechanism of tissue injury and disease?
|
- T cell mediated
- CD4: macrophage activated, inflammation - CD8: target cell killing, inflammation |
|
|
What is immunologic tolerance?
|
Specific unresponsiveness of the normal immune system to an individuals own self-antigens
|
|
|
What are the characteristics of T cell tolerance?
|
Long-lived, more complete
|
|
|
What are the characteristics of B cell tolerance?
|
Short-lived, less complete than in T cells and is quiescent in the absent of T cell help
|
|
|
What determines whether an antigen will induce tolerance?
|
- Immunologic maturity: neonates and elderly are immunologically immature and respond poorly to antigens
- Antigenic structure and dose: simpler the molecule and very high or low doses elicits tolerance - Immunosuppressive therapy: enhances tolerance |
|
|
What are the principle factors in the development of auto-immune disease?
|
- Inheritance of susceptibility genes which may contribute to FAILURE of self-tolerance
- Environmental triggers which may activate self-reactive lymphocytes - Uncontrolled immune response |
|
|
How common are auto-immune disorders?
|
1-2% of individuals (however many may be classified as "auto-immune" without formal evidence that the response is specific for self-antigen)
|
|
|
Many auto-immune diseases have been linked to mutations in what genes? Characteristics?
|
Genes encoding MHC
- Incidence of a particular auto-immune disease is often greater in individuals who inherit a particular HLA allele = "relative risk" - Mutations in HLA genes are NOT by themselves the cause of the disease (many with these mutations do not develop disease) |
|
|
How do mutations in MHC contribute to auto-immune disease?
|
- Inefficient in displaying self-antigens → defect in central tolerance
- Antigen presentation by those MHC may not stimulate Treg cells → defect in peripheral tolerance |
|
|
How do you treat auto-immune diseases?
|
Relies on reducing the immune response sufficiently to eliminate symptoms:
- Systemic immune suppression (corticosteroids, antimetabolites, and nucleoside analogs) - Non-systemic immune suppression (Abs to TNF (infliximab) and soluble TNFR (etanrecept) - Plasmapheresis or competitive FcR inhibition |