Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
18 Cards in this Set
- Front
- Back
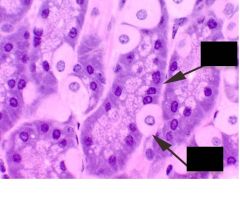
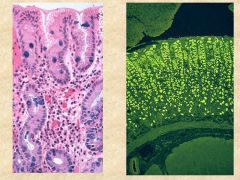
What are the cell types seen here? What section of the stomach are we in?
What is the function of each cell? |
Top = chief cell (purple, basophilic- produce pepsinogen
Bottom = parietal cell (pink, looks like fried egg)- makes HCl and Intrinsic Factor We are in the fundus/body (where these cells are mostly found). Cardia = mainly mucous cells |
|
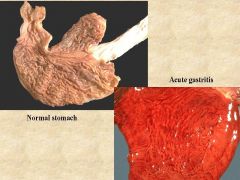
What changes do you suspect on histology in a person with acute gastritis?
|
Acute gastritis- will likely show fibrinous exudate, reactive looking epithelium with neutrophils.
|
|
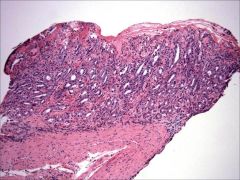
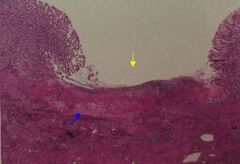
What is the difference between erosion and ulceration?
Which one is shown above? |
Erosion= superficial loss of epithelium (shown here, no mucous cells seen on top and active, neutrophilic infiltrate).
Ulceration = full thickness loss of mucosa |
|
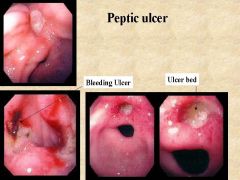
90% of Chronic gastritis is as a result of ______.
What are other causes of Chronic gastritis? What are some features seen on endoscopy? |
H pylori infection = most common.
Others= autoimmune, Chemical/reactive (from NSAIDS, bile reflux secondary to gastric bypass, or EtoH), uremia/radiation. Note hyperemia and edema formation. Some ulceration. |
|
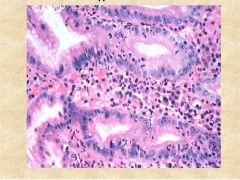
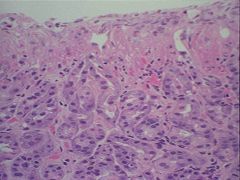
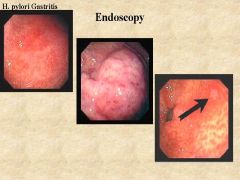
What is the causative agent of this individual's gastritis? What further imaging could be done to confirm this?
What part of the stomach is this? |
H.pylori Gastritis. Most likely in antrum (H-pylori doesn't like parietal and chief cells).
Characterized by dense lymphoplasmocytic infiltrate in the LP. You also see neutrophils (ACTIVE inflammation). Use alcian blue stain or electron microscopy to confirm. |
|
What is the major complication associated with HP gastritis?
|
Can lead to atrophy of the stomach with intestinal metaplasia. Can lead to adenocarcinoma.
May induce MALT tissues --> marginal zone lymphoma. |
|
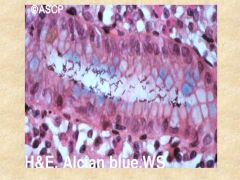
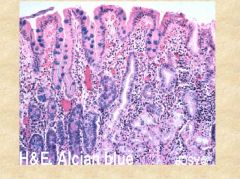
What type of chronic gastritis does the person above have?
What might the antibodies shown in the immunofluorescence image be to? |
Autoimmune chronic gastritis (note- no parietal or chief cells seen in the body of stomach on left). Instead, you see intestinal metaplasia.
Anti-parietal cell or Anti-IF antibodies might be found. Pts develop B12 deficiency, Pernicious anemia. *note: the pathogenesis is likely T-cell mediated attack of cells that releases IF, allowing the body to form antibodies. |
|
|
HP infection vs Autoimmune gastritis
Location? Predoimate cell infiltrate? Abs in serum? Complications? |
1. Location: HP in antrum, AI in body
2. Cells: HP = plasma cells, polys. AI = lymphocytes 3. Abs: H. pylori vs. Parietal cells/IF 4. Complications: HP = peptic ulcer, adenocarcinoma, lymphoma. AI = atrophy, pernicious anemia, neuroendocrine tumor, adenocarcinoma |
|
Where do 98% of ulcers in the body form (hint: two locations)?
What does it look like on histology? |
Mostly Antrum and Duodenal bulb.
On histology looks like ulcer (full loss of surface mucosa) and granulation tissue seen. |
|
|
What is the most common type of gastric polyp? What type of polyps are associated with chronic PPI use?
When do we get concerned about polyps? |
Hyperplastic polyp= most common. Fundic gland polyps = associated with chronic PPI use (because they decrease acid production --> lead to hyperplastic response by parietal cells)
Worry when polyp >1.5cm (could be dysplasia, biopsy it). |
|
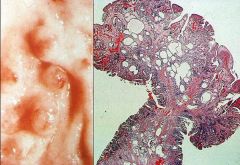
What are the histologic features of the polyp shown above?
Where in the stomach is it typically found and what condition is it associated with? |
Hyperplastic polyp= polypoid shape with dilated glands.
Typically found in antrum of stomach. Associated with chronic gastritis. |
|
|
What is the second most common type of solid tumor in the world? Where in the world is it most prevalent?
What demographic is typically affected by Intestinal type? By the Diffuse type? |
Gastric carcinoma - mostly Asia >South America >> USA
Intestinal type - M>F, usually over 50. Associated with H pylori Diffuse type - M=F, younger patients, no environmental influence. Familial cancer (E-cadherin mutation). |
|

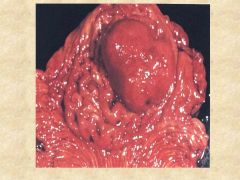
What is the most common site in the stomach for a gastric carcinoma? Which type of Gastric carcinoma is shown above?
What would the pathology of this type of carcinoma look like? |
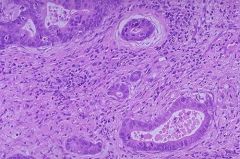
Antrum = most common (because that is where H pylori live). Ulcerative type gastric carcinoma (associated with Intestinal adenocarcinoma).
Would look like glands invading into the lamina propria and submucosa. |
|

What type of carcinoma is shown here?
What would the appearance of this be on pathology? |
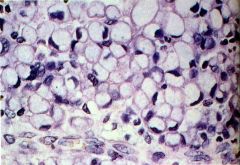
Diffuse type carcinoma (gives the stomach a leather bottle appearance, linitis plastica or diffuse gastric wall thickening)
Signet ring cells found in the lamina propria (essentially globs of mucin within cell with eccentric nuclei). |
|
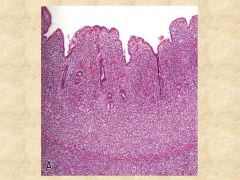
How are gastric cancers staged?
What type of cancer is shown above and how can you tell? |
Based on the depth of invasion (size doesn't make a difference)
Above = MALT lymphoma. Immediately you see that there is no mucosa and it looks like lymphocytic infiltration took over. |
|
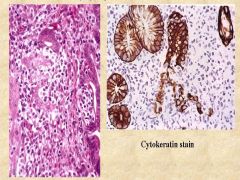
What is the causative agent responsible for this condition? What are the pathognomonic features shown here?
What would staining with CD20 and CD3 look like? |

H pylori = causes marginal zone lymphomas. This is a lymphoepithelial lesions (lymphocytes invading and destroying gland).
B cell positive (CD20) top and T-cell negative (CD3) bottom |
|
What type of stomach cancer is this?
What cells does this tumor derive from? What is the treatment? |
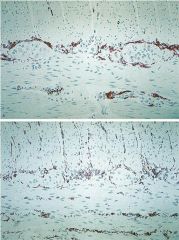
GIST = gastrointestinal stromal tumor. It derives from intestinal cells of Cajal (part of auerbach and myenteric plexus) *normal cells are shown above.
Treatment = surgery or Gleevec (because the mutation is in a tyrosine kinase, c-kit. |
|

What would this tumor stain positive for?
|
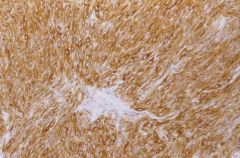
This is a GIST (GI stromal tumor), stains positive for c-kit (a tyrosine kinase).
|