Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
26 Cards in this Set
- Front
- Back
|
What are the features of ulcerative colitis?
|
Limited to colon (except backwash into the ileum)
Limited to mucosa Begins at rectum, progresses continuously and proximally |
|
|
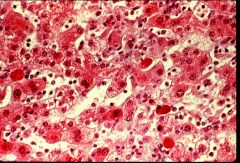
Acute viral hepatitis
|

What is this process?
|
|
|
Coagulative necrosis (from toxic injury)
|

What process is this?
|
|
|
What are the intestinal manifestations of UC?
|
Blood and mucus in stool
Cramping is WORSE with passage of stool Pain more common in LLQ Tenesmus while there isn't anything in rectum (feeling is from inflammation) |
|
|
What is cirrhosis?
|
A diffuse process throughout the liver in which nodules of regenerating hepatocytes are surrounded by bands of fibrosis
|
|
|
What are the intestinal manifestations of UC?
|
Blood and mucus in stool
Cramping is WORSE with passage of stool Pain more common in LLQ Tenesmus while there isn't anything in rectum (feeling is from inflammation) |
|
|
What are the biopsy findings of UC?
|
Crypt distortion (not unique to UC), Acute and chronic infiltrate of PMN’s and lymphocytes
|
|
|
Cirrhosis
|

What condition of the liver is this?
|
|
|
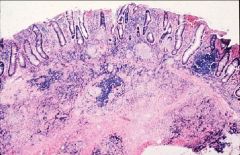
Ulcerative colitis - notice the inflammatory cells in the mucosa.
Crypts are sparse and branching. Crypt abscesses |

What disease is this?
|
|
|
What is mallory hyaline?
|
A dense condensation of cytoskeletal proteins in the cytoplasm of hepatocytes
|
|
|
What are the systemic complications of UC?
|
episcleritis, uveitis, eythema nodosum, pyoderma gangrenosum, peripheral arthritis (seronegative), ankylosing spondylitis and sacro-iliits, sclerosing cholangitis, cholangiocarcinoma
|
|
|
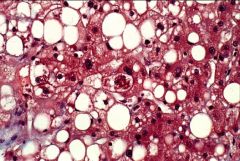
Steatosis
|

What liver pathology is this?
|
|
|
What are the features of Crohn's disease?
|
Involves any part of the GI tract
May be skip lesions Can be transmural GRANULOMA is pathognomonic, but not sine qua non |
|
|
Mallory hyaline
|
What liver pathology is represented by the cell in the center?
|
|
|
What are the intestinal manifestations of Crohn's Disease?
|
Depend on location, extent, and severity
Pain may be periumbilical or RLQ Inflammatory mass may be palpated Nausea/vomiting if in stomach or duodenum, also early satiety, epigastric pain, dysphagia Perianal skin tags, fissures, fistulae Increased pain, distension, borboyrgmi are signs of stenosis and obstruction |
|
|
Acidophils - apoptotic hepatocytes
|

What type of cells are these?
|
|
|
What are linear ulcers indicative of?
|
Crohn's
|
|
|
Ballooning degeneration
|
What are the big, pale cells?
|
|
|
Crohn's (see granuloma, significant inflammation of all layers
|
What disease is this?
|
|
|
What are systemic complications of small bowel syndrome?
|
Gallstones, malabsorption, fatty diarrhea, oxalate stones in kidney
|
|
|
Dysplasia (big, disorganized nuclei)
And frank cancer |

What does this slide show?
|
|
|
What is the potential pathogenesis of IBD?
|
Inappropriate activation of mucosal immune system
Caused by autoimmunity to luminal or mucosal antigen? Response to normal flora? Dysfunctional suppressor T cells Inability to mount reciprocal cytokine response Infection Genetic and environmental contributants |
|
|
What are the specific aspects of the pathogenesis of Crohn's disease?
|
Cell-mediated! -Macrophages and dendritic cells
Induced by Th1 cells --> IFN-g, TNF-a, IL-12 |
|
|
What are the specific aspects of the pathogenesis of ulcerative colitis?
|
Humoral! Autoantigens cross-react with bacterial Ags from normal flora
Lack of regulatory cells Excess CD4 effector cells Th2 response pANCA in 70% |
|
|
What is the stepwise approach for treatment of IBD?
|
1. Aminosalicylates (5-ASA)
2. Corticosteroids 3. Immunomodulatory (6-MP + azothiaprine) 4. Infliximab (for CD) 5. Other agents that sometimes work (methotrexate, cyclosporine) |
|
|
there is no question here
|
Thank God.
|