![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
71 Cards in this Set
- Front
- Back
|
Elimination |
The excretion of waste products |
|
|
Variables influencing Bowel Elimination |
-Stress -Medication -Diet -Exercise -Diagnostic Studies -Illnesses |
|
|
Developmental Considerations |
Age affects what a person eats and the body’s ability to digest nutrients and eliminate waste. The stools of an infant are markedly different from those of an older person. *Because patients are often reluctant to discuss their bowel habits and stool characteristics, nurses need to be familiar with bowel concerns pertinent to each developmental group. |
|
|
Effects of food on bowel elimination |
High-fiber foods, such as whole grains and bran, dried peas and beans, and fresh fruits and vegetables, increase the bulk in fecal material. *High fiber foods recommended for the older adult along with water intake |
|
|
Infant Developmental Considerations |
-The stool characteristics depend on whether the infant is being fed breast milk or formula. -The stools of both breastfed and formula-fed infants may have curds and mucus. -Infants have no voluntary control over bowel elimination. -liquid stool -stool color matches food |
|
|
Toddler Developmental considerations |
-Between the ages of 18 - 24 mths voluntary control of defecation becomes possible. -Daytime bowel control is attained by 30 mths but varies with each child. -May become constipated due to picky eating |
|
|
School-Aged Child, Adolescent, and Adult Developmental considerations |
From childhood into adulthood, defecation patterns vary in quantity, frequency, and rhythmicity. *high risk for constipation |
|
|
Older Adult developmental considerations |
Constipation is often a chronic problem for older adults. Diarrhea can also result from physiologic or lifestyle changes. |
|
|
Effect of medication on stool |
Antacids: can make stool grey or white Aspirin, Anticoagulants: can make stool red or black Antibiotics: can make stool green *May cause diarrhea or constipation |
|
|
Stool Collection |
1.Hand hygiene 2.Wear disposable gloves (medical asepsis) 3.Do not contaminate outside of container 4.Observe agency policy for obtaining, packaging and transporting of specimen |
|
|
Stool Characteristics |
-Shape -Odor -Volume -Consistency -Constituents |
|
|
Elimination Diagnostic Studies |
A. Esophagogastroduodenoscopy B. Colonoscopy C. Sigmoidoscopy D. Upper GI series *The ingestion of barium during diagnostic procedures, such as a barium enema, may result in constipation or impaction if it is not completely eliminated after the procedure. |
|
|
BOWEL ELIMINATION FACTORS TO ASSESS |
1.Usual Patterns 2. Aids 3.Recent changes 4.Problems 5.Presence of an ostomy |
|
|
Indirect visualization studies |
•Upper GI series •Small bowel series •Barium enema •Abdominal ultrasound •Magnetic resonance imaging (MRI) •Abdominal Computed Tomography (CT) *useful for detecting obstructions, strictures, inflammatory disease, tumors, ulcers, and other lesions, and for diagnosing a hiatal hernia and other structural changes in the gastrointestinal tract. |
|
|
Occult Blood |
blood that is hidden in the specimen or cannot be seen on gross examination, can be detected with screening tests. *Nurses may perform tests for occult blood in the stool at the bedside within an institution or outpatient setting, or by patients at home, allowing for low-cost inpatient and outpatient screening. More commonly, the sample is sent to a medical laboratory for processing. |
|
|
Outcome Identification for pts w/o specific bowel elimination problems |
The patient will: -Have a soft, formed bowel movement every 1 to 3 days without discomfort -Explain the relationship between bowel elimination and dietary fiber, fluid intake, and exercise -Relate the importance of seeking medical evaluation if changes in stool color or consistency persist |
|
|
Planning Interventions for pts w/ specific bowel elimination problems |
The pt will: -Describe the functioning and purpose of the ostomy -Ingest an adequate amount of fiber -Monitor the amount and consistency of stools -Express acceptance of the ostomy -Demonstrate skin care for the ostomy -Respond to the urge to defecate in a timely manner -Maintain the integrity of perineal skin |
|
|
Promoting regular bowel habits |
Promote regular bowel habits in well and ill patients by attention to: -timing -positioning -privacy -nutrition -exercise. |
|
|
Methods to evacuate the bowel |
Classification of Laxatives: -Bulk-forming (e.g., Metamucil) promotes peristalsis -Stool softener (e.g., Colace) lubricates -Emollient (lubricant, e.g., mineral oil) lubricates -Stimulant (e.g., Dulcolax) promotes peristalsis -Osmotic (e.g., Miralax) more frequent bowel movements -Enema (cleansing or retention) |
|
|
Warning signs of colon cancer |
-Change in the bowel elimination pattern -Blood in the stoolsRectal or abdominal pain -Change in the character of the stool -Sensation of incomplete emptying after bowel movementuu < |
|
|
Colostomy Care |
•Inspect the patient’s stoma regularly •Measure intake and output •Explain each aspect of care •Encourage patient to care for and look at the stoma |
|
|
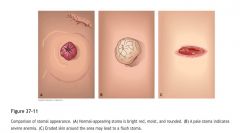
Comparison of stomal appearance |
|
|
|
Location of Ostomies |

|
|
|
PatientTeaching (Post Ostomy)- "The patient will… |
•explain the reason for the diversion and the rationale for treatment." •demonstrate self care behaviors." •describe follow-up care and support services."•report where to purchase supplies in the community." •verbalize fears and concerns." •demonstrate positive body image." |
|
|
Postoperative Pain (Ostomy) |
-Monitor for infection -Monitor for skin breakdown (due to pt not willing to move) -Ambulate -Medication (every 4-6 hours) |
|
|
Factors Affecting Basal Metabolic Rate (BMR) |
•Males have a higher BMR due to larger muscle mass –BMR is about 1 cal/kg of body weight per hour for men –BMR is about 0.9 cal/kg of body weight per hour for women
|
|
|
•Factors that decrease BMR |
-Aging -prolonged fasting -sleep |
|
|
•Factors that increase BMR |
–Growth -infections -fever -emotional tension -extreme environmental temperatures -elevated levels of certain hormones |
|
|
Carbohydrates |
Sugar and Starches Most abundant & least expensive source of calories in the work. •50 to100 g of carbohydrates are needed daily to prevent ketosis( Important for Diabetic pts) |
|
|
Nutrients that supply energy |
1.Carbs 2. Lipids 3. Fats |
|
|
Nutrients that regulate body processes |
1.Vitamins 2.Minerals 3. Water |
|
|
Protein |
•Required for the formation of all body structures •Animal proteins are complete; plant proteins are incomplete. •RDA for adults is 0.8 g/kg of body weight, 10% to 35% total calorie intake |
|
|
Fats |
•Most concentrated source of energy in the diet •RDA not established, should be no more than 20% to 35% total calorie intake Animal fats are saturates Plant fats are unsaturated |
|
|
Trans fat |
Trans fat occurs when manufacturers partially hydrogenate liquid oils; trans fat raises serum cholesterol. |
|
|
Vitamins |
•Needed for metabolism of carbohydrates, protein, and fat •Classified as fat soluble or water soluble |
|
|
Which vitamins affects visual acuity in dim light, formation and maintenance of skin and mucous membranes, and the immune function? |
Vitamin A |
|
|
Vitamins D, E, and K. |
Vitamin D provides calcium and phosphorus metabolism and stimulates calcium absorption. Vitamin E is an antioxidant that protects Vitamin A. Vitamin K helps the synthesis of certain proteins necessary for blood clotting |
|
|
Minerals |
•Organic elements found in all body fluids and tissues •Some function to provide structure in the body, others help regulate body processes •Macrominerals include calcium, phosphorus, and magnesium. •Microminerals include iron, zinc, manganese, and iodine. |
|
|
Water |
•Provides fluid medium necessary for all chemical reactions in the body •Acts as a solvent and aids digestion, absorption, circulation, and excretion |
|
|
Tell whether the following statement is true or false.
Food is more vital to life than water because it provides the medium necessary for all chemical reactions and it is not stored in the body. |
False
Rationale: Water is more vital to life than food because it provides the medium necessary for all chemical reactions and it is not stored in the body. |
|
|
Physical, sociocultural, and psychosocial factors influencing food choices |
Economics culture religion tradition education politics social status food ideology |
|
|
Physiologic and physical factors influencing food choices |
Stage of development state of health medications |
|
|
Developmental Considerations |
•Growth •Activity increases nutritional needs •Age-related changes in metabolism and body composition |
|
|
Risk Factors for Poor Nutritional Status |
•Developmental factors •Gender •State of health •Alcohol abuse •Medications •Mega doses of nutrient supplements |
|
|
Components of Nutritional Assessment |
•History taking –Dietary,medical, socioeconomic data •Physical assessments –Anthropometric and clinical data •Laboratory data –Protein status, body vitamin, mineral, and trace element status |
|
|
Anorexia |
Lack of appetite |
|
|
Dietary Data |
•24-hour recall method •Food diaries/calorie counts •Food frequency record •Diet history |
|
|
Factors to Assess for Nutritional Status |
•Dietary data •Medical and socioeconomic data •Anthropometric data •Clinical data •Biochemical data |
|
|
Nursing Interventions |
•Teaching nutritional information •Monitoring nutritional status •Stimulating appetite •Assisting with eating •Providing oral nutrition •Providing long-term nutritional support |
|
|
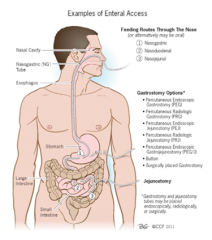
Enteral Nutrition |
•Alternate form of feeding that involves passing a tube into the gastrointestinal tract to allow the instillation of the appropriate formula. •Tube passes through the nose or mouth, down through the esophagus, and into the stomach or intestine (duodenum or jejunum) —Must have functioning GI tract —IF THE GUT WORKS, USE IT! —Exhaust all oral diet methods first. |
|
|
Nasogastric and Orogastric Tubes |
Levin Tube Dobb hoff Tube Salem Sump Tube |
|
|
Enteral Feeding Routes |
|
|
|
Short-Term Nutritional Support |
•Using the nasogastric or nasointestinalroute •Confirming NG feeding tube placement –Radiographic examination –Measurement of aspirate pH and visual assessment of aspirate –Measurement of tube length and tube marking –Carbon dioxide monitoring –Confirming nasointestinal tube placement |
|
|
Long-Term Nutritional Support |
•An enterostomal tube may be placed through an opening created into the stomach (gastrostomy) or into the jejunum (jejunostomy). •A gastrostomy is the preferred route to deliver enteral nutrition in the patient who is comatose. •Placement of a tube into the stomach can be accomplished by a surgeon orgastroenterologist via a percutaneous endoscopic gastrostomy (PEG) or asurgically (open or laparoscopically)placed gastrostomy tube. |
|
|
Parental Nutrition |
•Delivery of nutrients intravenously, via the bloodstream. •Central Nutrition: Total Parental Nutrition (TPN) •Peripheral Parental Nutrition (PPN) |
|
|
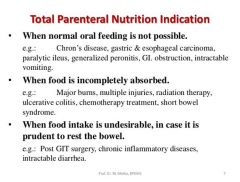
Total Parental Nutrition Indication |
|
|
|
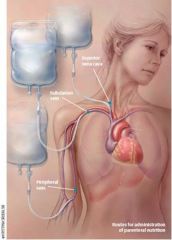
Routes of Administration TPN/ PPN |
|
|
|
Total Parenteral Nutrition (TPN) |
•Highly concentrated •Hypertonic nutrient solution •Meet sthe patient’s nutritional needs •Administered through a central venous access device •Multilumen catheter into the subclavian vein, or a peripherally inserted central catheter(PICC) |
|
|
Peripheral Parenteral Nutrition (PPN) |
•Less concentrated nutrient solution •For short-term nutrition -lasting less than 2 weeks •Administered through a peripheral vein |
|
|
Complications of TPN |
•Insertion problems •Infection and sepsis •Metabolic alterations •Fluid,electrolyte, and acid–base imbalances •Phlebitis •Hyperlipidemia •Liver and gallbladder disease |
|
|
Perioperative Phase |
Starts when the surgeon & pt manually decide that surgery is necessary and ends when pt enters the operating room. |
|
|
Intraoperative Phase |
Starts when the pt enters the operating room and ends when patient enters the PACU (post anesthesia care unit) |
|
|
Postoperative Phase |
Starts when the pt enters the PACU and ends with complete recovery from surgery. |
|
|
Caring for the Postoperative pt |
1.Immediate (provided in the PACU, prevents complications from anesthesia or surgery) 2. Ongoing (assessment) |
|
|
Respiratory |
-Coughing and deep breathing (increases lung expansion, helps expel anesthetic gases, facilitates oxygenation) |
|
|
Incentive Spirometer |
helps increase lung volume and promote inflation of the alveoli. |
|
|
Cardiovascular |
-monitor vital signs, cardiac rate, and rhythm, skin color and cognition -assess for peripheral pulses -watch for hypotension, hypertension, tachycardia, bradycardia -tachycardia is an early symptom of shock -compare postop with preop data -decreased urine output |
|
|
Central Nervous System |
-reorient pt to surroundings -recovery from general anesthesia requires neurological checks with anesthesia checks |
|
|
Postop Complications |
-Hemmorrhage -Shock -Thrombophlebitis -Respiratory complications -Pulmonary emboli -Pneumonia -Atelectasis -Surgical site complications (dehisince, fistula, etc.) |
|
|
Hypothermia (<96F) can lead to: |
-Poor would healing -hemodynamic stress (general condition of the body) -Cardiac disturbances -Coagulopathy (ability for blood to clot) -Delayed recovery from anesthesia -Shivering |
|
|
Wound management |
-Dressing checks -Wound Checks -Drainage assessment -Drains (penrose, Hemovac, Jackson-Pratt) -Wound complications (Dehiscence, Evisceration, Fistula, Infection) |