Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
21 Cards in this Set
- Front
- Back
|
What is a breech presentation
|
Breech: fetus whose buttocks are adjacent to the cervical canal
|
|
|
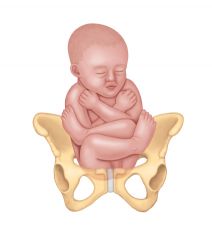
Describe a frank breech presentation
|

Hips flexed, legs extended so that feet are adjacent to fetal head
|
|
|
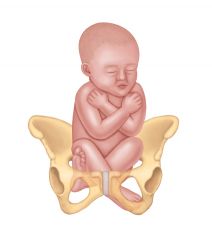
Describe the complete breech presentation
|
Both hips and knees are flexed
|
|
|
Describe the incomplete breech presentation
|
One or both hips are not completely flexed
|
|
|
Describe the footling and kneeling breech
|
Footling - one or both feet are the presenting part
Kneeling - one or both knees are the presenting part |
|
|
Risks in labour with breech presentation
|
Fetus - increased risk of harm because risk of cord compression between cervix and body and breech crowns
Risk of dystocia Cord prolapse Always think has the fetus adopted this position because of an underlying abnormality? |
|
|
Risk factors for a breech presentation
|
Maternal RF
pelvis (contracted) uterus (shape abnormalities, intrauterine tumours, fibroids) extrauterine tumours causing compression grand multiparity Maternal-fetal RF placenta praevia amniotic fluid (poly/oligohydramnios) fetal prematurity multiple gestation congenital malformations abnormalities in fetal tone and movement aneuploidy |
|
|
Diagnosis of breech
|
Physical examination
Ultrasound Vaginal examination during labour |
|
|
Management of breech
|
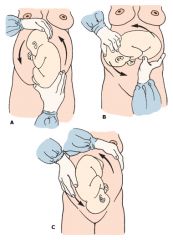
Ceasarean
External cephalic version (fetus turned to breech via manipulation of mother's abdomen) - 65% success rate - must be > 37 weeks, singleton, unengaged presentating part |
|
|
Name some long term complications associated with breech presentations
|
Increased risk of mild deformations (frontal bossing, low set ears, prominent occiput)
|
|
|
How is presentation defined
|
The part of the fetus that leads into the birth canal
vertex (occiput), face, brow, breech (frank, footling, complete, incomplete) shoudler compound (limb and head of breech) |
|
|
Diagnosis of fetal malpresentation
|
During labour through internal examination of the cervix
|
|
|
Risk factors for face and brow presentation
|
multiparity
cephalopelvic disproportion prematurity polyhydramnios fetal anomalies (anencephaly, neck mass) Contracted pelvis (brow) |
|
|
Management of brow presentations
|
50% will convert to normal vertex presentation
Allow spontaneous labour to progress. Monitor closely, if arrest of labour - CS Persistent brow is not compatible with vaginal delivery |
|
|
Management of face presentation
|
Mentum anterior or transverse - allow labour to progress - can give oxytocin augmentation
Mentum posterior - must CS |
|
|
What is the most common cause of obstructed labour
|
cephalopelvic disproportion
|
|
|
What is the most common type of breech presentation?
|
Frank
hips flexed, knees extended so that feet are adjacent to fetal head |
|
|
CI to external cephalic version
|
CI - previous CS, previous myomectomy, oligohydramnios, PROM, placenta praevia, abnormal US, hypertension, suspected IUGR, uteroplacental insufficiency
|
|
|
Risks of external cephalic version
|
abruption
cord compression |
|
|
Maternal complications of obstructed labour
|
intrauterine infection following prolonged ROM
bladder/rectal trauma - stress incontinence ruptured uterus - haemorrhage vesico-vaginal fistula or recto-vaginal fistula |
|
|
RF for breech presentation
|
Polyhydramnios
Preterm labour Multiparity Multipel gestation Fibroids Uterine anomaly |