Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
64 Cards in this Set
- Front
- Back
|
right lateral
|
What view(s) should be taken to evaluate the neck?
|
|
|
If have right breed
- 2-3 mo old bulldog - Always had prob breathing - May have pneum Static dz - Lumen of trachea doesn’t change much with repeated views (not like trach coll) |
When would you be suspicious of laryngeal hypoplasia?
|
|
|
inspiration (extrathoracic)
expiration (intrathoracic) |
When during respiration do you expect to see a tracheal collapse?
|
|
|
1. Mandible
2. Axis (C2) 3. Bullae 4. Nasopharynx 5. Oropharynx 6. Soft Palate 7. Epiglottis 8. Cricoid Cartilage 9. Hyoid Apparatus 10. Trachea T. Thyrohyoid Bone B. Basihyoid Bone C. Keratohyoid Bone E. Epihyoid Bone S. Stylohyoid Bone |

|
|
|
similar to the size of the cricoid cartilage
|
What should the tracheal size be?
|
|
|
epiglottic mass
marked dilation/ overinflation of oropharynx and nasoparynx |

|
|
|
neck neoplasia that has invaded trachea
|

|
|
|
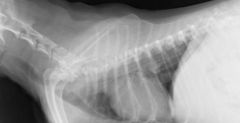
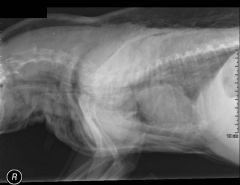
hypoplastic trachea
decreased generalized lumen of the trachea - static (no change with repeated images) bulldog that is 2-3 mo old and has always had difficulty breathing |

|
|
|
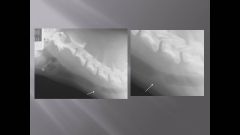
tracheal stenosis
hx of trauma - recent anesth - FB - bite wound |
|
|
|
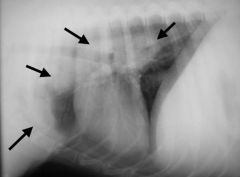
intrathoracic and mainstem bronchi collapse
|
|
|
|
mainstem bronchi collapse
|
|
|
|
extrathoracic tracheal collapse
|

|
|
|
normal mainstem bronchi
|

|
|
|
redundant tracheal membrane
|

|
|
|
tracheal mass
Looking for: - Narrowing of tracheal lumen - Dilation cranial to lesion |

|
|
|
Overinflation of naso/oropharynx
Epiglottis pushed down so really trying to suck in air with all they have (sign of dyspnea) look for tracheal obstruction caudally (mass/ foreign body/ stenosis) |
|
|
|
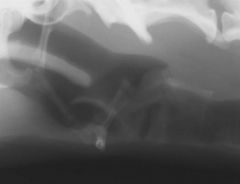
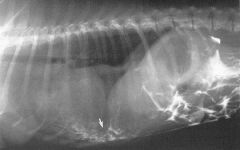
tracheal rupture
notice all the air under the skin |
|
|
|
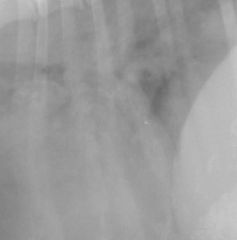
tracheal foreign body (bifurcation of main stem bronchi)
|
|
|
|
tracheal foreign body
|
|
|
|
high kVp
- thorax has inherent contrast minimize exposure time - breathing causes blurring take at peak inspiration (usually) use grid if > 10 cm |
What technique do you want to use for the thorax?
|
|
|
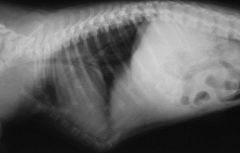
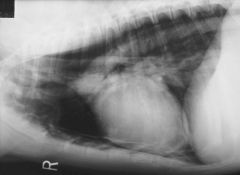
Right lateral
- Heart “egg shaped” - Diaphragmatic crura parallel to each other - Right crus more cranial (cd vena cava enters right crus) - gas in fundus of stomach - Better for assessing changes in the LEFT lung lobes |
|
|
|
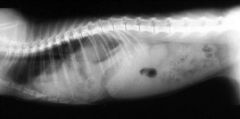
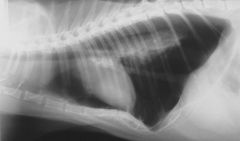
Left lateral
- Heart rounded - Diaphragmatic crura diverge - Left crus more cranial (cd vena cava enters cd into right crus) - gas in pylorus - Better for assessing changes in the RIGHT lung lobes |

|
|
|
DV
diaphragm has one smooth dome |
|
|
|
VD
diaphragm has 3 domes |

|
|
|
right lung
b/c shows up on left lateral and not on the right lateral |
|
|
|
expiratory film
|
|
|
|
close to the lung of interest
*there is no dependent lung* |
For a large animal radiograph being taken with horizontal beam, where do you place the film
|
|
|
pectus excavatum
only see clin signs if severe |
|
|
|
pectus carinatum
no clin significance |
|
|
|
rib fractures
they will heal fine with rest |

|
|
|
extrapleural mass
|

|
|
|
pulmonary mass
notice acute angle with thoracic wall |

|
|
|
primary rib tumor
ddx 1. OSA 2. OSA 3. OSA 4. CSA 5. fungal/ abscess if hunting dog |

|
|
|
rib met
lysis/ irregular bone formation |

|
|
|
rib mets
|

|
|
|
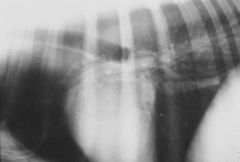
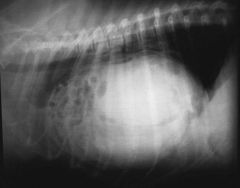
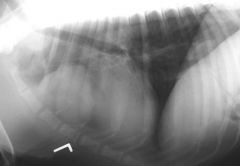
diaphragmatic hernia
|
|
|
|
congenital diaphragmatic hernia
incidental finding until proven otherwise |

|
|
|
stomach herniation
|

|
|
|
stomach herniation
|

|
|
|
celiogram of diaphragmatic hernia
Inject iodinated (NOT barium!) contrast medium into the peritoneal cavity Lift the hindquarters of the dog to get the contrast to flow cranially If there is an abnormal hole in the diaphragm, the contrast will show up in the pleural space Pitfall: Plugging of diaphragmatic rent with organs, fibrin etc. - If don’t see it leak, doesn’t mean you don’t have it, but if it does leak, into thorax, then you have confirmed hernia |
|
|
|
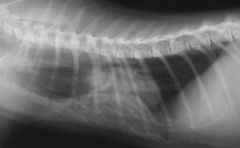
Hiatal hernia
- Stomach coming through the esophageal hiatus Transient lesion cd-dorsal on lung lobe that comes and goes, then consist with sliding hiatal hernia - Usually not a prob (can have vomiting or severe dz if entrapment) |

|
|
|
Peritoneal-pericardial diaphragmatic hernia (PPDH)
- Abdominal contents in the pericardial sac |
|
|
|
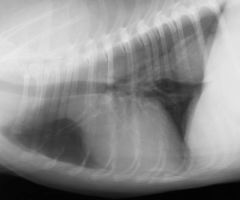
Normal Mediastinum
Structures that are normally seen - Trachea - Heart - Aorta - Caudal vena cava - Fat Structures occasionally seen - Gas in the esophageal lumen - Thymus (Dogs < 1 yr) Structures NOT normally seen Won’t see an outline of these strx physiologically - Cranial vena cava, brachiocephalic trunk - Lymph nodes - Sternal - Cranial mediastinal - Tracheobronchial - Outer surface of trachea and esophagus |

|
|
|
Mediastinal shift due to recumbent atalectasis (pull force)
The mediastinum (with the cardiac silhouette) is shifted to one side on the DV or VD radiograph Due to: Pull forces - Recumbent atelectasis - They see this multiple times every day - Dog was laying on right side x few min then do VD = heart on right side - Previous lung lobectomy - Bronchial obstruction … - Decreased volume of lung b/c lung collapses Push forces - Intrathoracic masses - Diaphragmatic hernia - Chest wall deformities … - Pectus excavatum |

|
|
|
Mediastinal shift due to diaph hern
The mediastinum (with the cardiac silhouette) is shifted to one side on the DV or VD radiograph Due to: Pull forces - Recumbent atelectasis - Previous lung lobectomy - Bronchial obstruction … - Decreased volume of lung b/c lung collapses Push forces - Intrathoracic masses - Diaphragmatic hernia - Chest wall deformities … - Pectus excavatum |

|
|
|
enlarged sternal LN
Neoplastic (less likely inflammatory) process affecting thoracic wall, thymus, cranial mammary complexes, pleura or peritoneum. Make sure to check the abdominal cavity! |

|
|
|
generalized mediastinal lymphdenopathy
lymphoma or fungal dz (blasto) |
|
|
|
generalized mediastinal lymphadenopathy
lymphoma or fungal dz (blasto) |

|
|
|
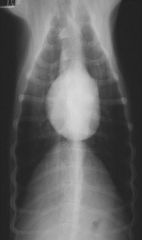
cranioventral mediastinal mass
most likely lymphoma or thymoma |
|
|
|
cranioventral mediastinal mass
most likely lymphoma or thymoma |

|
|
|
caudodorsal mediastinal mass
most likely paraesophageal mass or hiatal hernia |
|
|
|
caudodorsal mediastinal mass
most likely paraesophageal mass or hiatal hernia |

|
|
|
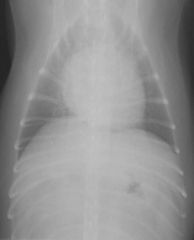
mediastinal effusion
Recognized by - Decreased visualization of mediastinal structures - Diffuse widening of the mediastinum |
|
|
|
mediastinal effusion
Recognized by - Decreased visualization of mediastinal structures - Diffuse widening of the mediastinum |

|
|
|
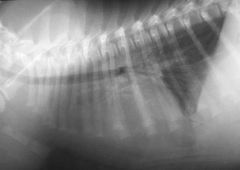
pneumomediastinum
notice that you can see the azygous and aorta |
|
|
|
pleural effusion
notice fissure lines |

|
|
|
pleural effusion
notice fissure lines |

|
|
|
pleural effusion
|

|
|
|
pleural effusion
|

|
|
|
DV view of pleural effusion
On a DV view, fluid gravitates ventrally and accumulates dorsal to the sternum -> silhouetting of heart and fluid |

|
|
|
VD view of pleural effusion
On a VD view, fluid gravitates dorsally and accumulates around the caudodorsal lung fields -> heart still visible |

|
|
|
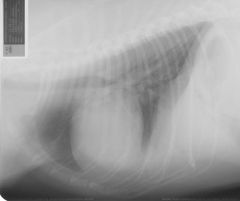
pneumothorax
|

|
|
|
pneumothorax
|

|
|
|
tension pneumo
|
|