Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
103 Cards in this Set
- Front
- Back
|
main components of hemostasis
|
blood vessels
platelets coagulation system |
|
|
major events in normal hemostasis
|
formation of primary platelet plug (primary hemostasis)
formation of insoluble clot of cross-linked fibrin (secondary hemostasis) clot retraction and fibrinolysis |
|
|
blood vessels fxn in hemostasis
|
structural
- interactions between platelets and coagulation factors - esp subendothelial collagen neuromechanical - vasoconstriction biochemical - endothelial synthesis and metabolism of bioactive molecules |
|
|
the coagulation system involves interconnected _____, _____, and _____ pathways that are maintained in delicate balance
|
pro-coagulant
anti-coagulant fibrinolytic |
|
|
platelet production regulated by
|
thrombopoietin
|
|
|
platelet lifespan
|
~ 1 wk
|
|
|
what activates platelets
|
soluble (ex thrombin) and insoluble (collagen)
undergoes shape change and fxnal change |
|
|
what are the major fxns of platelets in hemostasis
|
adhesion to damage blood vessels
aggregation with other platelets (really impt) - formation of platelet plug - localization of coagulation on platelet surface release of bioactive substances (ex granule contents, TXA2, has both pro and anticoagulant activity) evenual clot retraction |
|
|
structure of platelet
|
flat disk shape when quiescent, spherical with pseudopodia when activated
dense tubular system (modified ER) is a reservoir for calcium membrane invaginations form network w/in platelet (open canilicular system) involve release of contents expansion of surface area when activated alpha and dense granules contain many bioactive molecules including calcium, ADP, fibrinogen, vWF, histamine, serotonin cytoskeletal components miantiain shape, mediate shape change, aslo involved in release of granule contents and receptor interactions surface receptors include GPIIb-IIIa (fibrinogen receptor) and GPIb (vWF receptor) |
|
|
when give aspirin or other NSAIDs, what important part of the coagulation system are you interfering with
|
arachidonic acid (TXA2 released by platelets)
|
|
|
total solids vs total protein
|
total solids
- on chemistry total protein - refractometer |
|
|
leukocytes
what areas are associated with what part of a teenage soldier's life |
storage pool
- boot camp blood vessel - flight to war zone tissue - battle ground |
|
|
leukocytes
proliferation pool |
immature, blastic looking, big nucleus, probably can't tell if erythroid or myeloid
myeloblasts - prob can't tell if erythroid or myeloid |
|
|
the storage pool of leukocytes is found
|
within the maturation pool
|
|
|
we sample leukocytes from ____ pool
the number in this pool is affected by what why take multiple samples throughout day |
circulating pool
the number in the circ pool is affected by bone marrow and what is going on in the tissues very dynamic process (so check mult times throughout day |
|
|
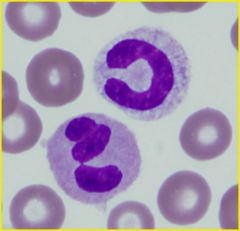
RBC
segmented neutrophil (lower left) band (upper right) |
|
|
neutrophil fxn
|
Phagocytosis and killing of bacteria and other pathogens
Inflammatory mediators Tissue damage they are immature 18 yr old boys -> just want to go kill stuff and tear stuff up |
|
|
what is the signal (radio call) to tell the new recruits (neutrophils) to land the plane, get off, and fight there?
|
cytokines
|
|
|
__________ say "This is the battleground dumbasses"
|
inflammatory cytokines
|
|
|
____ is impt in grabbing neutrophils from the circulating pool
|
surface adhesion molecules
|
|
|
if you have a crap ton of cytokines, what happens
|
they can get back to bone marrow and tell it to make more neutrophils
|
|
|
how do you get increased neutrophil production
|
Increased stem cell recruitment
- Pluripotential stem cell commits to myeloid differentiation Increased effective granulopoiesis - Reduced myelocyte attrition Shortened maturation time |
|
|
increased bands in circulation is associated with
|
inflammation somewhere in the body
left shift they aren't fully developed, but they are sent out to meet increased demand |
|
|
differentials for extreme neutrophilia
|
pyo-something
hemolytic anemia Hepatozoon americanum tumor secreting G-CSF or GM-CSF chronic granulocytic or myelogenous leukemia leukocyte adhesion deficiency |
|
|
differentials for neutrophilia
|
physiologic (epi) response
stress (steroid) response acute inflammation chronic inflammation pyo-something hemolytic anemia Hepatozoon americanum tumor secreting G-CSF or GM-CSF chronic granulocytic or myelogenous leukemia leukocyte adhesion deficiency |
|
|
differentials for neutropenia
|
excess tissue demand
sequestration (pseudoneutropenia) decreased granulopoieiss ineffective granulopoiesis peripheral destruction |
|
|
differentials for lymphocytosis
|
physiologic (epi) response
chronic inflammation addison's dz persistant lymphocytosis of cattle lymphocytic or lymphoblastic leukemia |
|
|
differentials for lymphopenia
|
stress (steroid) response
acute inflammation depletion/ loss lymphoid hypoplasia or aplasia |
|
|
toxic change
|
diffuse cytoplasmic basophilia
- retained ribosomes cytoplasmic vacuolation - cytoplasmic granule dissolution Dohle bodies - aggregates of endoplasmic reticulum toxic granulation - primary granules visible *not neutrophil hyperseg* |
|
|
neutrophil hypersegmentation
|
5 or more distinct lobes
prolonged transit - corticosteroid - cushings - late stage chronic infection NOT TOXIC CHANGE |
|
|
differentials for eosinophilia
|
parasites
allergic/ hypersensitivity rxns idiopathic paraneoplastic MCT addison's dz leukemia |
|
|
differentials for basophilia
|
parasitism
allergic rxn hematopoietic neoplasia |
|
|
monocytosis
|
inflammation (acute or chronic)
stress neoplasia (leukemia) secondary to neutropenia |
|
|
what does a stress response look like
|
increased segs and monos
decreased lym & eos |
|
|
what does a physiologic response look like
|
increased segs and lym
|
|
|
what does chronic inflammation look like?
acute? |
chronic
- increased segs, monos, lymp acute - increased segs, monos - decreased lym |
|
|
what causes changes in the circulating pool of neutrophils
|
increased/ decreased marrow influx
demargination increased margination increased emigration |
|
|
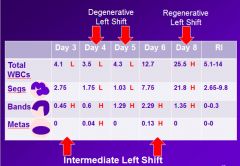
neutrophila - left shift
|
number of segs not enough to meet tissue demand
immature forms released - bands - metamyelocytes |
|
|
neutrophilia
regenerative left shift |
marrow meets tissue demand with release of immature forms
segs outnumber immature forms total WBC count increased |
|
|
neutrophilia
degenerative left shift |
marrow is not meeting tissue demand
immature forms equal or outnumber segs total WBC count is typically normal or decreased neutropenia with segs outnumbering immature forms considered left shift by some |
|
|
what animals are prone to a stress response?
physiologic? |
Stress
- dogs Physiologic - birds - cats - horses |
|

|
|
|
|
neutrophilia - acute inflammation
|
Marrow release exceeds tissue emigration; increased tissue migration also
Left shift - Demand depletes storage pool - Bands release from maturation pool |
|
|
neutrophilia - chronic inflammation
|
Increased granulopoiesis restores maturation and storage pools
Increased release from marrow Increased emigration into tissues +/- Left shift |
|
|
causes of extreme mature neutrophilia
|
tumor secreting G-CSF or GM-CSF
chronic myeloid leukemia |
|
|
chronic myeloid leukemia
|
leukemia of mature neutrophils
M:E ratio severely increased looks just like chronic inflammation for acute ML, see a lot more blasts in bone marrow and in circulation you are backed into dx of CML - rule out everything else |
|
|
extreme neutrophilic leukocytosis
|
> 50,000(dog)
>30,000(cat) pyo-something hemolytic dz (esp IMHA) hepatozoon americanum G-CSF or GM-CSF secreting tumor granulocytic leukemia leukocyte adhesion deficiency |
|
|
neutropenia with degen left shift is assoc with
|
large purulent lesions
marked migration into tissue exceeds marrow release poor prognosis if persistent |
|
|
neutropenia - sequestration
|
pseudoneutropenia
endotoxin-induced margination number of neutrophils out in circulation is normal, they are just stuck to vessel wall due to endotoxin |
|
|
neutropenia - decreased granulopoiesis
|
decreased neutrophils at all stages
cancer therapies viral/ rickettisal infections idiosyncratic drug rxns primary or metastatic neoplasia toxins (estrogen/ bracken fern) marrow necrosis or fibrosis pancytopenia |
|
|
neutropenia - excessive ineffective granulopoiesis
|
normal proliferation with maturation arrest
assoc with viral infections and myelodysplasplastic syndromes |
|
|
neutropenia - peripheral destruction
|
anti-neutrophil antibodies mediate destruction
less common than IMHA or IMT |
|
|
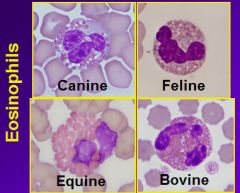
if you were a guest star on the CSI, which blood cell would you use to ID a species
|
eosinophil
|
|
|
neutrophilia - 4 main causes and what they look like
|
physiologic (epi)
- increased segs - increased lym stress (glucocorticoid) - increased segs/monos - decreased lym/eos acute inflammation - increased segs - +/- bands *usually +* - decreased lym chronic inflammation - increased segs - +/- bands (if present, will be less than acute) - increased lym |
|
|
what does pyo-something look like on CBC
|
decreased segs
increased bands degenerative left shift +/- metamyelocytes |
|
|
what does decreased granulopoiesis look like
|
neutropenia of all stages
no left shift |
|
|
what does ineffective granulopoiesis look like
|
normal -> increased proliferating pool
decreased maturation pool decreased storage pool |
|
|
|
|
|
eosinophil fxn
|
Elimination of parasites
Promote inflammatory associated with asthma and allergic diseases Suppress hypersensitivity / allergic reactions Infiltration of certain tumors (assoc w/ mct) |
|
|
eosinophil production and kinetics
|
Maturation parallels neutrophils
Storage pool exists Proliferation stimulated by IL-5 produced by mast cells, macrophages, T-cells Emigrate into skin, lungs, GIT, and endometrium |
|
|
causes of eosinopenia (if our reference range wasn't already 0)
|
Little diagnostic significance
Low end of our range is usually 0 or very close to it Glucocorticoid-associated Cell redistribution, inhibition of mast cell degranulation Acute inflammation Physiologic / epinephrine mediated |
|
|
______ is the largest granulocytic leukocyte
|
basophils
|
|
|
ribbon like segemented nucleus is assoc w
|
basophils
|
|
|
basophil morphology
|
Largest granulocytic leukocyte
Ribbon-like segmented nucleus Variable number of purple granules |
|
|
basophil fxn
|
Elimination of GI parasites
Participate in allergic / hypersensitivity reactions Prevention and promotion of hemostasis |
|
|
basophilia w/o eosinophilia
|
bad bone marrow disorder
probably myelodysplastic dz |
|
|
why do you often see increased monos with neutrocytosis
|
b/c derived from the same bi-potential progenitor cell
|
|
|
which animal is most prone to experience neutropenia after a bout with acute inflammation
|
cow
|
|
|
basophil production & kinetics
|
Numbers are sparse in mammals
Production stimulated by IL-3 Activated by IL-3 or IgE binding |
|
|
lymphocyte morphology
|
Smallest leukocytes
Round to indented nucleus Small amount of cytoplasm Can have granular cytoplasm Ruminants have small and large lymphocytes |
|
|
______ is the smallest leukocyte
|
lymphocyte
|
|
|
plasma cell morphology
|
Eccentric, round nucleus
Pale Golgi zone Abundant, basophilic cytoplasm don't see in blood do see in aspirate (Mott cell - plasma cell in need of exlax) |
|
|
what is a mott cell
|
a plasma cell in need of some exlax
|
|
|
lymphocyte fxn
|
B-cells (and plasma cells)
- Antibody production T-cells and B-cells - Immunoregulation – Directors of the immune system Cytotoxic T-cells and NK cells - Kill virus-infected cells and tumor cells |
|
|
lymphocyte production and kinetics
|
Maturation occurs in secondary lymphoid tissues
Long lived Only leukocyte that recirculates (returns to circulating blood after tissue emigration via lymphatics) |
|
|
____ is the only leukocyte that recirculates
|
lymphocyte
|
|
|
why does addisons dz cause lymphocytosis
|
lack of glucocorticoids that normally prevent lymphocytosis
|
|
|
why do you see lymphopenia with acute inflammation
|
prob due to cortisol excess
|
|
|
____ is the largest leukocyte
|
monocyte
|
|
|
_____ is the largest granulocytic leukocyte
|
basophil
|
|
|
monocyte morphology
|
Largest leukocytes
Nuclei are oval to irregular in shape Cytoplasm - Blue-gray - Vacuoles |
|
|
monocyte fxn
|
Phagocytize and digest foreign material
Phagocytize and kill organisms Synthesis of CSFs and cytokines Antigen presentation Help eliminate viral-infected cells and tumor cells |
|
|
monocyte production and kinetics
|
Derived from bipotential stem cell
No maturation or storage pools Marginated and Circulating pools Tissue monocytes: - Macrophages - Histiocytes - Specialized mononuclear cells Survive in tissue for weeks to years |
|
|
WBC count via blood smear
|
WBCx/ 40-50x filed x 2000
always do for quality control |
|
|
WBC count automated
|
impedence counters
- relies on the fact that cells are poor electrical conductors - reliable cell counts - unreliable differentials flow cytometer - as cells pass through laser beam, they absorb and scatter light - interruptions in beam determine cell count - light scatter is used to determine cell type |
|
|
impedance counters rely on the fact that____________
what are they reliable/ unreliable at determining |
cells are poor conductors
reliable cell counts unreliable differentials |
|
|
what is used to determine cell count and type in flow cytometer
|
cell count
- interruptions in laser beam as cells pass cell type - light scatter |
|
|
sources of error in WBC count
|
inherent
clumps large platelets fragile WBCs heinz bodies nRBC |
|
|
corrected WBC count
|
(initial WBC count x 100) / (100 + nRBC)
use when nRBC > 10 |
|
|
leukoctye differential
|
100-200 leukocytes counted and classified
% x total WBC count = absolute # of each leukocyte type |
|
|
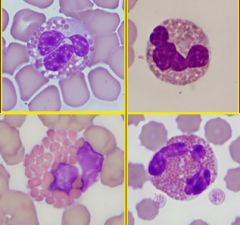
toxic change
|
disturbances in accelerated maturation
seen in patients with - severe bacterial infections - septicemia - acute inflammatory conditions - extensive tissue destruction basophilic cytoplasm - retained ribosomes cytoplasmic vacuolation - loss of granule integrity Dohle bodies - aggregated RER - indiscrete amorphous blue concretions in cytoplasm - can be see in healthy cats toxic granulation - primary granules visible due to altered membrane permeability - allows uptake of reddish-purple stain - rare finding can be difficult to distinguish from monocytes tend to indicate a severe inflammatory condition |
|
|
what does toxic change look like
|
basophilic cytoplasm
- retained ribosomes cytoplasmic vacuolation - loss of granule integrity Dohle bodies - aggregated RER - indiscrete amorphous blue concretions in cytoplasm - can be see in healthy cats toxic granulation - primary granules visible due to altered membrane permeability - allows uptake of reddish-purple stain - rare finding can be difficult to distinguish from monocytes |
|
|
when do you see toxic change
|
in patients with
severe bacterial infection septicemia acute inflammatory condition extensive tissue destruction |
|
|
___ is the term for morphologic changes in neutrophil cytoplasm due to disturbances in accelerated maturation
|
toxic change
|
|
|
what is loss of granule integrity in neutrophils termed
|
cytoplasmic vacuolation (toxic change)
|
|
|
what is the term for retained ribosomes in neutrophils
|
basophilic cytoplasm (toxic change)
|
|
|
what is the term for aggregated RER in neutrophils
|
Dohle bodies (toxic change)
|
|
|
neutrophil hypersegmentation
|
prolonged transit time
neutrophil with 5 or more distinct lobes secondary to - steroid excess (corticosteroid administration, cushing's, late stage chronic inflammation) - neutrient deficiencies (B12, folic acid, or cobolt) - poodles with hereditary macrocytosis - MDS |
|
|
neutrophil hyposegmentation
|
left shifted maturation
pelget- huet anomaly - abnormality of the leukocytes to segment (so none will be segmented) - eos and baso also hyposeg - nuclear chromatin still tighly condensed - cellular fxn is normal - seen in so dog breeds, cats, rappids, and horses pseudo-pelger-huet anomaly - transient, acquired - seen in cattle neutrophils - dog swith severe inflammation - cats with FeLk induced myeloid leukemia asynchronous maturation of neutrophils |
|
|
reactive monocytes
|
increased cytoplasmic basophilia
seen with inflammatory conditions |
|
|
reactive lymphocytes
|
increased amt of more basophilic cytoplasm
- represent stimulated T or B cells seen with acute and chronic inflammatory dz |
|
|
lymphoblasts
|
immature lymphocytes characterized by a
- larger cell - less dense nuclear chromatin - visible nucleoli - variable amt of basophilic cytoplasm inidicate lymphoid malignancy not commonly found in peripheral blood |
|
|
reactive change
|
nonspecific finding indicating immunologically stimulated cells
- monocytes - lymphocytes increased cytoplasmic basophilia inidicative of inflammatory conditions |