Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
16 Cards in this Set
- Front
- Back
|
Phases of Ventricular Cell AP and names
|
Phase 4 - rest/diastole
Phase 0 - depolarization/upstroke Phase 1 - early repolarization Phase 2 - plateau Phase 3 - repolarization |
|
|
Phase 4 channels and permeability
|
Phase 4 (rest/diastole) – dominated by KIR channel (producing IKr current) & PK. More permeable to Na then other cells.
|
|
|
Phase 0 channels and permeability
|
Phase 0 (upstroke of AP) – ↑ in PNa
|
|
|
Phase 1 channels and permeability
|
Phase 1 (early repolarization) – transient ↑ PK & ↓PNa (channel inactivation)
|
|
|
Phase 2 channels and permeability
|
Phase 2 (plateau) - ↑ PCa (VGCa channels) & ↓PK (indirectly V, dependent Mg2 blocks channel)
|
|
|
Phase 3 channels and permeability
|
Phase 3 (repolarization) - ↓PCa (channel inactivation) & ↑PK (voltage gated “delayed rectifiers” and then ↑↑PK (Mg2 removeed and IK1 restored)
When IK1 is restored so is resting membrane as in Phase 4. |
|
|
Ventricular Cells relative permeability
|
At rest (phase 4) – the Na permeability is higher and thus Na/K ATPase density is higher.
Generally cells at rest have low ion permeabilities requiring less E at rest. However, Cardiac muscle has high ion permeabilities at rest. Again like the resting situation cardiac muscle is opposite of the general rule. During activation most cells have increased ion permeability. Cardiac muscle has decreased ion permeabilities during activation = this allows sustainable high rates of contraction without the loss of K gradient. K+ efflux is spared. |
|
|
AP diagram in Ventricular Cell
|

|
|
|
Significance High K permeability in cardiac function
|
10X fold higher PK results in more stable resting EM. This means ↓ risk for arrhythmias leaving the ventricles a slave to the pacemaker cells.
|
|
|
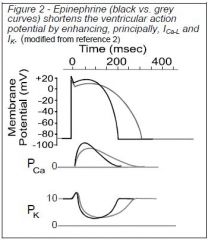
NE /Epinephrine affect on ventricle AP
|
Shortens ventricular AP
NE released from sympathetic fibers resuts in activation of PKA. The kinase (P) Ca-L(voltage gated), KR (rapid), KS(slow) channels. PCa is altered after the initial slope. Reason for the same initial is that it is a voltage gated channel and thus dependent on the same voltage change. Sympathetic (NE) results in 25-35% ↓ AP time BUT 50-75%↓↓ time betw/ AP. |
|
|
Epi/NE affect on Ventricle AP
|
|
|
|
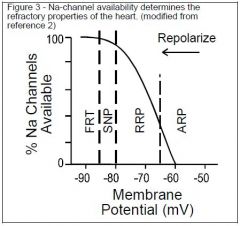
Refractory Periods Diagram
|
|
|
|
Order of the 3 refractory periods
|
Absolute refractory period (<50% Na available)
Relative refractory period (<95% Na available) - larger stimulus produces a smaller than normal propagated AP Supranormal period - slightly smaller stimulus produces normal propagated response Full recovery time |
|
|
Normal QT interval
|
QT interval (0.12 – 0.2 seconds) – measures time beginning ventricular depolarization to end of ventricular repolarization
|
|
|
Prolonged QT
|
Therefore a prolonged QT represents a slow ventricular depolarization-repolarization cycle. Arrthymias are common at elevated HR. Additionally, at elevated HR, ventricular filling ↓ as well as CO ↓. This is because less time is spent in refilling because the contraction time cannot decrease and heart is being told to ↑HR leaving only the PR interval to decrease (P wave + PQ segment).
|
|
|
Common cause prolonged QT syndrome
|
Genetic Mutations in
1. Delayed rectifier K channels Delayed activation (90% of cases) ↓ probability of opening ↓ sensitivity to PKA modulation 2. Voltage gated Ca channels 3. Voltage gated Na channels |