Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
53 Cards in this Set
- Front
- Back
|
SHould you ONLY follow EBM?
|
no, you must still use clinical expertise to tailor tx for your indiidual pts
|
|
|
what kind of knowledge should you use alongside EBM?
|
pathphysiology knowledge
|
|
|
what would my practice look like with EBM?
|
always modifying diagnostic and tx techniques according to recent literature.
not relying on dogma throwing "rules" out the window |
|
|
What is POEM and DOE?
|
POEM- patient oriented evidence that matters- pay attention to this because it deals with patient outcomes and regular practice
DOE- disease oriented evidence- don't pay much attention because it is premature research and may not be related to daily practice and hasn't tested for pt outsomes yet |
|
|
what is the cochrane collaboration?
|
an INTERNATIONAL group that conducts systematic reviews to discover POEMs that can change practice
|
|
|
give a baby example of when pathophysiology reasoning got trumped by EBM
|
drs used to recmmend laying babies on their stomach to prevent aspiration while sleeping, but research found that this actually dramatically raised SIDS
|
|
|
give an example of when a DOE showed something to be good, but a POEM showed it to be bad.
what were they measuring? |
ecainide and flecainide showed decrease in ventricular arrythmias (DOE measured arrythmmia effect to be good), but pts on these drugs died more often (POEM measured mortality to be bad)
|
|
|
Randomised controlled trial (RCT)
what is it? |
trial where people are randomly assigned to control or intervention group
|
|
|
what does risk mean?
|
probaility of a bad outcome
|
|
|
What is ARR?
give an example if the intervention group had 12% bad outcomes and the control had 20% |
Absolute Risk Reduction - is 8%
overall how much less bad outcomes happens with intervention? |
|
|
What is NNT
give an example if the intervention group had 12% bad outcomes and the control had 20% |
Number Needed to Treat
100/8 = 12.5 how many people do you need to treat before one person would theoretically be saved from the intervention? |
|
|
How are ARR and NNT related to one another?
|
they are inverse of one another
|
|
|
What is relative risk?
give an example if the intervention group had 12% bad outcomes and the control had 20% |
the risk in the intervention over the risk in the conrol
.12/.20 = .6 |
|
|
What RR would be good, bad, or neutral
|
below 1 is good
1 shows no effect above 1 is bad |
|
|
what does it mean if I say the RR of a drug was 1.5?
|
you will be 50% more likely to have a bad outcome if you take the drug
|
|
|
what is an odds ratio?
how do you calculate it? |
the odds that an intervention created a bigger risk
set up a 2x2 table comparing people that did get bad outcomes and those that didn't multiply each groups numbers and divide between groups |
|
|
is odds ratio and RR the same thing?
|
kind of. they go in the same relative direction, but the numbers don't work out to be the same
|
|
|
what is cumulative incidence/risk?
|
the answer to the question "how far has the disease spread in a certain time interval"
measures freq of disease new cases/population being measured = % cumulative risk |
|
|
highest cumulative risk you can have?
|
100%
|
|
|
what kind of calculation is cumulative risk needed for?
|
relative risk
|
|
|
what happens in a cohort study?
|
you follow a bunch of undiseased people over time and see if they develop the disease eventually.
people are split into exposed to variable of interest vs not exposed groups. |
|
|
two major kinds of cohort studies? what is the difference?.
|
prospective and retrospective
has the disease outcome occured at the time of the study initiation? |
|
|
what is a clinical trial?
|
when you randomly assign people to an exposure vs nonexposure group to test outcomes
|
|
|
What is a community trial?
|
when you randomly assign whole communities rather than individuals to an exposure
ex. comparing communities who are given fluoridated vs non flouridated water for outcomes. |
|
|
why would you do a clinical vs community trial?
|
clinical- for an intervention that would eventually be applied to individuals (i.e. drugs)
community - for an intervention that would eventually be applied to communities like flouridating water |
|
|
what is the difference between incidence and prevalence?
what are they each used to say? |
incidence- how many new cases happened in a given time period
--used to calculate your risk of developing a disease prevalence- how many people have something in a given snapshot ---used to calculate your likelihood of having a disease |
|
|
give an example of a low incidence and high prevalence
|
DES has somewhat of a prevalence, but no incidence over the last couple decades
|
|
|
difference between morbidity and mortality?
|
morbidity- illness/disease
mortality- death |
|
|
how would you go about reporting mortality? give an example.
|
83 per 100,000
if 83 out of 100,000 people with lung cancer died in a year. |
|
|
is a person either morbid or not?
|
no, they can have co-morbidities
|
|
|
What is an open clinical trial?
|
a clinical trial where there is no control group
|
|
|
what is a double blind vs triple blind study?
when would you use a triple? |
double- subject and observer don't know who has tx
triple- also the person analyzing the data doesn't know triple is used when the data is "soft" or can be interpreted multiple different ways |
|
|
what is a crossover clinical trial?
|
where the participants receive both treatments consecutively, but do not know in which order
|
|
|
what is a pilot study?
|
a study condiucted on a small scale to see if it should be conducted for real.
fleshes ot problems and tells you how you should design the real study |
|
|
what is a observational descriptive vs observational analytical study?
when is each performed? |
both require no intervetnion
descriptive is when we don't have much info analytic is when we have enough info to formulate a hypothesis to analyze the data to test |
|
|
NOW WE DO EBM VIA DIT!
what are case-control studies? dissect |
when we look at people who have the disease (case)
and people who don't have the disease (control) and find out what the case has/does that the control does not |
|
|
what conclusions can you draw from case control studies?
|
risk factors ASSOCIATED with a disese
no causation |
|
|
Who may do a case cotnrol study?
|
CDC
|
|
|
What are two qualities about a case control study?
|
observational and retrospective
|
|
|
opposite of observational?
|
experimental
|
|
|
what exactly does cohort mean?
what does a cohort study have to involve in terms of peritciipants? |
a group of people with something in common (exposure or non exposure)
you need at least two cohorts for a cohort study |
|
|
what is the difference between odds ratio vs relative risk?
when would you use each? which is better? |
odds ratio is just an approximation of relative risk when you don't know the exactl risk percentage (total population of interest and their outcomes)
relative risk is better |
|
|
what is the basic calculation for risk vs odds?
|

|
|
|
what is the risk vs odds of rolling a 2 in a 4 sided die?
|
risk- 25% or 1 out of 4
odds- 33% or 1 to 3 |
|
|
why are odds used in horse racing?
|
it is a fair payout where if you multiply the amount of the bet by the odds, you are expected to break even
|
|
|
when does odds ratio approximate relative risk and when can it not?
|
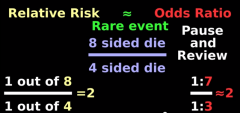
only when the risk is small
|
|
|
if teens normally have 80% of them grow taller and an elixir increases that by 10%, what is the relative risk vs the odds ratio? do the math
|
RR- .9/.8 = 1.125 = 12.5% more likely than control to grow taller
OR- 90:10/80:20 = 9/4 = 2.25 = odds are more than 2 times greater sooo misleading! |
|
|
how you you put a RR of .8 into words?
|
the risk of developing a disease was decreased by 20% in persons exposed compared to those unexposed
|
|
|
2 ways to put into words a RR of 3.3
|
1. the risk of developing a disease was 230% greater than the unexposed group
2. the experimental grop was 3.3 times more likely to develop the disease than the unexposed group |
|
|
when may a RR of 3 be significant vs not significant.
|
depends on how they first started out.
if they started out at a high baseline of risk, then it is impressive (ex. 30% --> 90%) but .1% to .3% is not impressive |
|
|
between RCT, Cohort, and Case-Control, rank them in order of most to least prone to bias
what sort of RR or OR should we want from each to be impressed? |
most: case control (OR>4), cohort(RR>3), RCT (even a little)
|
|
|
what can case-control studies only be measured by? why?
|
odds ratio because for a given risk, you only know the # of people with it who got the disease vs didn't get it.
you don't know the true population |
|
|
what is the difference between a case control study and a retrospective cohort study>
|
in case control investigator splits individuals by disease status whereas in retrospective cohort, investigator splits study individuals by their exposure status.
|