![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
144 Cards in this Set
- Front
- Back
|
Does the esophagus contain a serosa? |
No. |
|
|
What type of muscle makes up the upper 1/3 of esophagus? |
striated muscle |
|
|
What type of muscle makes up the lower 2/3 of esophagus? |
smooth muscle |
|
|
What is the blood supply to the thoracic esophagus? |
vessels from aorta |
|
|
What is the blood supply to the cervical esophagus? |
inferior thyroid a. |
|
|
What is the blood supply to the abdominal esophagus? |
left gastric a. and inferior phrenic aa |
|
|
What is the venous drainage of the esophagus |
azygous and hemiazygous vv |
|
|
What is the lymphatic drainage of the esophagus? |
upper 2/3 drain cephalad, lower 1/3 drains caudad |
|
|
Where does the R vagus n travel as it exits the chest? |
along the posterior wall of the stomach (becomes celiac plexus) |
|
|
What is the criminal n of Grassi? |
can cause persistently high levels of acid if undivided in vagotomy (on R vagus n) |
|
|
Where does the L vagus n travel as it exits the chest? |
on the anterior wall of the stomach, goes to liver and biliary tree |
|
|
What is the path of the thoracic duct? |
travels from right to left at T4-5 as it ascends and inserts into the left subclavian vein. |
|
|
Where is the upper esophageal sphincter? |
15cm from incisiors |
|
|
What comprises the upper esophageal sphincter? |
cricopharyngeus mm (prevents air swallowing) innervated by recurrent laryngeal n |
|
|
What is the resting pressure of the UES? |
60mmHg (relaxes at 15mmHg) |
|
|
Where is the most common site of esophageal perforation? |
cricopharyngeus (also most common site for foreign body |
|
|
What causes aspiration with a brainstem stroke? |
failure of cricopharyngeus to relax |
|
|
Where is the lower esophageal sphincter |
40cm from incisors Tonically contracted, inhibitory neurons cause relaxation . NOT an anatomic sphincter |
|
|
What is the resting pressure of the LES? |
15mmHg (relaxes to 0) |
|
|
What is the surgical approach to the cervical esophagus? |
Left |
|
|
What is the surgical approach to the upper 2/3 thoracic esophagus? |
Right (to avoid aorta) |
|
|
What is the surgical approach to the lower 1/3 of the esophagus esophagus? |
Left |
|
|
What is the reflex arc of hiccoughs? |
vagus-->phrenic-->sympathetic chain T6-12 |
|
|
What is better for picking up an esophageal mass when patient has dysphagia? Barium swallow or EGD? |
barium swallow |
|
|
What are some common causes of pharyngeal disorders? |
Difficulty getting food from mouth to esophagus Myasthenia gravis, muscular dystrophy, stroke Liquids worse than solids |
|
|
Tx for Plummer vinson syndrome? |
dilation for esophageal web, iron replacement, screen for oral cancers |
|
|
What is Zenker's diverticulum? |
false diverticulum caused by high pressure during swallowing caused by failure of relaxation of cricopharyngeaus |
|
|
Where do Zenker's diverticula occur? |
between pharyngeal constrictors and cricopharyngeus posteriorly |
|
|
How do you diagnose Zenker's diverticula? |
Barium swallow or manometry EGD increases risk of peforation |
|
|
What is the tx for zenkers diverticula? |
cricopharyngeal myotomy thru left neck incision EITHER resect or suspend diverticula (left cervical incision, leave drains, esophagram on POD1 |
|
|
What is a traction diverticula? |
True diverticula due to inflammation, granulomatous dz or tumors |
|
|
Where do traction diverticula occur? |
lateral in mid esophagus |
|
|
What are the symptoms of traction diverticula? |
regurgitation of undigested food, dysphagia |
|
|
What is the tx for traction diverticula? |
resection if symptomatic with primary closure, may need XRT if due to malignancy leave alone if asymptomatic |
|
|
What is an epiphrenic diverticulum? |
Due to esophageal motility disorders |
|
|
Where are epiphrenic diverticula located? |
distal 10cm of esophagus |
|
|
What is the tx for epiphrenic diverticula? |
resection and esophageal myotomy on side opposite diverticulectomy |
|
|
Symptoms of achalasia? |
dysphagia, regurgitation, weight loss, respiratory symptoms |
|
|
What is the pathophysiology of achalasia? |
failure of LES relaxation --> lack of peristalsis due to neuronal degeneration in muscle wall (autoimmune destruction of neuronal ganglion cells) |
|
|
What does the manometry reading show in achalasia? |
increased LES pressure, incomplete LES relaxation, no peristalsis |
|
|
What is the radiologic appearance of achalasia on barium swallow? |
Birds beak. May have dilated, tortuous esophagus with epiphrenic diverticulae need EGD to rule out cancer |
|
|
Treatment of Achalasia |
balloon dilatation of LES (80% effective) Meds: nitrates, Ca channel blockers Botox : 60% recurrence If FAIL then do Heller myotomy 2 cm below GE junction on stomach and 6.5 cm proximally on esophagus (longitudinal and circular mm) |
|
|
What is a Heller myotomy ? |
For achalasia. Exposure with left thoracotomy (or laparoscopic), myotomy of lower esophagus only (cardia) . Need a partial fundoplication (toupet) to hold open myotomy /prevent reflux |
|
|
What infection can cause symptoms similar to achalasia? |
Trypanosoma cruzi (Chagas disease) |
|
|
What are the symptoms of diffuse esophageal spasm? |
chest pain, may have dysphagia, psych history |
|
|
What does the manometry of diffuse esophageal spasm show? |
strong non-peristaltic unorganized contractions, LES relaxes normally |
|
|
Tx for diffuse esophageal spasm |
calcium channel blockers, trazadone, Heller myotomy (upper and lower esophagus) if other measures fail . surgery usually not as successful as in achalasia |
|
|
What are the symptoms of nutcracker esophagus? |
chest pain, dysphagia |
|
|
What does the manometry of nutcracker esophagus show? |
high amplitude peristaltic contractions (>180mmHg), LES relaxes normally |
|
|
Tx for nutcracker esophagus? |
Same as for diffuse esophageal spasm
calcium channel blockers, trazadone, Heller myotomy (upper and lower ES) if other measures fail . |
|
|
What does scleroderma do to the esophagus? |
fibrous replacement of esophageal smooth muscle. Loss of LES tone, reflex, strictures, lack of peristalsis on manometry |
|
|
What is the treatement for esophageal scleroderma? |
PPI, reglan. esophagectomy if severe |
|
|
What features of the stomach and esophagus protect from GERD? |
LES competence, normal esophageal body, normal gastric reservoir |
|
|
In a patient with heartburn what does dysphagia or odynophagia suggest? |
esophageal tumor |
|
|
In a patient with heartburn what does bloating suggest?
|
aerophagia and delayed gastric emptying |
|
|
In a patient with heartburn what does epigastric pain suggest?
|
PUD or tumor |
|
|
What is the first line therapy for GERD? |
Empiric PPI (omeprazole 99% effective) give for 3-4 weeks with escalating dose if ineffective |
|
|
When a patient fails medical therapy for GERD, what is the next step? |
pH probe (best test), endoscopy, histology, manometry |
|
|
What is the resting LES pressure in a patient with GERD? |
< 6mmHg |
|
|
What are the indications for surgery in a patient with GERD? |
failure of medical tx, avoidance of lifetime meds, young patients, refractory complications (bleeding, stricture) |
|
|
What are the steps of a Nissen Fundoplication? |
divide short gastrics, pull esophagus into abdomen, approximate the crura, 270 (partial) or 360 deg wrap of gastric fundus around esophagus. Secure wrap with single U stitch of prolene pledgeted on outside. Pass a 60Fr mecury weighted bougie through GE junction prior to closure |
|
|
What is the phrenoesophageal membrane an extension of? |
the transversalis fascia |
|
|
What are complications of a Nissen fundoplication? |
injury to the spleen, diaphragm, esophagus, pneumothorax |
|
|
What is a Belsey fundoplication? |
approach through chest , close hiatus |
|
|
What is a Collis gastroplasty? |
when not enough esophagus to pull down, staple along stomach cardia to make new esophagus |
|
|
What is the most common cause of dysphagia post-Nissen? |
wrap is too tight (often resolves on its own, give clears x 1 week, dilate) |
|
|
What is a type 1 hiatal hernia ? |
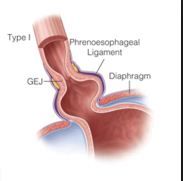
Most common. Sliding hernia from dilation of hiatus. Often associated with GERD |
|
|
What is a type 2 hiatal hernia? |
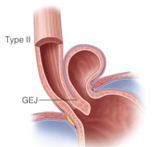
Paraesophageal hernia, hole in diaphragm along esophagus. LES not necessarily in chest. Associated with chest pain, dysphagia, early satiety |
|
|
What is a type 3 hiatal hernia |
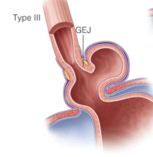
Combined type 1 and type 2 |
|
|
What is a type 4 hiatal hernia |
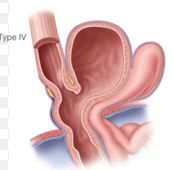
Entire stomach in chest plus another organ |
|
|
Why do type II hiatal hernias need to be repaired? |
High risk of incarceration do a Nissen with repair to anchor stomach and preserve LES function |
|
|
What is a schatzki's ring? |
narrowing of the lower esophagus that can cause difficulty swallowing (dysphagia). The narrowing is caused by a ring of mucosal tissue (which lines the esophagus) or muscular tissue.
at squamocolumnar junction |
|
|
What is the treatment of schatzki's ring? |
dilation and PPI. Do not need to resect |
|
|
What type of hiatal hernia is associated with Schatzki's ring? |
sliding hernia (type 1) |
|
|
What is Barrett's esophagus? |
squamous metaplasia to columnar epithelium due to GERD |
|
|
What is the risk of cancer in Barrett's esophagus? |
50x greater risk for adenocarcinoma must be confirmed by 2 pathologists |
|
|
What is the tx for Barrett's esophagus |
PPI or Nissen. Surgery will not prevent malignancy or cause regression of columnar epithelium Need lifetime surveillance with EGD High grade dysplasia : 3-month intervals; 4 quadrant Bx’s at 1-cm intervals for entire length of HGD and Bx of any suspicious areas |
|
|
What is the Tx for severe Barrett's dysplasia? |
esophagectomy if sick patient with limited reserve can do endoscopic resection |
|
|
What is the route of metastasis in esophageal tumors? |
submucosal lymphatics |
|
|
What are the symptoms of esophageal tumors? |
dysphagia (mostly solids), weight loss |
|
|
Risk factors for esophageal cancer? |
ETOH, tobacco, achalasia, caustic injury, nitrosamines, Barrett's |
|
|
What is the best initial test to look for esophageal tumors? |
Barium esophagram |
|
|
What makes an esophageal tumor unresectable? |
RLN involvement (hoarseness), Brachial plexus invasion (Horner's syndrome), phrenic nerve invasion, malignant effusion, malignant fistula, airway invasion, vertebral invasion, nodal involvement beyond area of resection Eval with CT scan. Chemo and XRT can downstage |
|
|
What is the most common esophageal cancer? |
adenocarcinoma |
|
|
Where does adenocarcinoma of the esophagus usually occur? Where does it metastasize? |
lower 1/3 of esophagus. Mets to liver |
|
|
Where does squamous cell carcinoma of the esophagus usually occur? Where does it metastasize? |
upper 2/3 of esophagus, mets to lung |
|
|
After evaluation of esophageal carcinoma with CT scan to confirm no mets, what test is performed for locoregional staging? |
EUS (sensitivity for celiac lymph node metastases were 85 and 90%) |
|
|
When is surgical rather than endoscopic resection offered in esophageal cancer? |
cancer that invades the muscularis mucosa, or if there is evidence of lymph node involvement on EUS
|
|
|
What is the mortality associated with esophagectomy? |
5% |
|
|
What percentage of ppl are cured from esophagectomy? |
20% |
|
|
What is the blood supply to the stomach after esophagectomy? |
Right gastroepiploic a. (left gastric and short gastrics are divided) |
|
|
What is involved in the transhiatal approach to esophagectomy? |
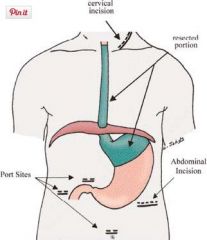
abdominal and neck incisions, blunt dissection of esophagus into thorax. Mortality from leaks decreased with cervical anastamosis |
|
|
What is involved in an Ivor Lewis Esophagectomy? |
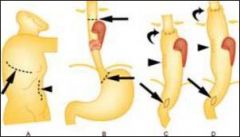
abdominal incision with Right thoractomy , exposes entire intrathoracic esophagus, anastamosis in chest |
|
|
What procedure must be performed in all esophagectomies? |
Pyloromyotomy (because sacrifice vagus) |
|
|
What is a colonic interposition? |
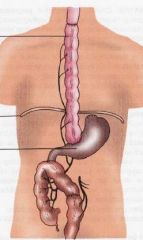
use colon based on marginal vessels as esophageal replacement. Need to make three anastamoses (preserves gastric function in young ppl) |
|
|
When do you get a swallow study in an esophagectomy? |
Postop day 7 |
|
|
How do you manage postoperative strictures in esophagectomy? |
dilation usually |
|
|
What preop chemotherapy is given in esophageal cancer? |
5FU and cisplatin (node positive disease or to shrink tumors) for T2, T3 XRT can downstage tumors |
|
|
What is the treatment for a malignat fistula in esophageal cancer? |
High mortality due to aspiration (3 mos), place a stent for palliation |
|
|
What is the most common benign esophageal tumor? |
Leiomyoma (in muscularis propria lower 2/3rds of esophagus) |
|
|
Do you biopsy a leiomyoma? |
No. can cause scarring which can make subsequent resection difficult |
|
|
What is the treatment for leiomyoma? |
If >5cm or symptomatic excision or extramucosal enucleation via thoracotomy |
|
|
Where are esophageal polyps located? |
cervical esophagus 2nd most common benign tumor can cause dysphagia or hematemesis |
|
|
What is the treatment of esophageal polyps |
If symptomatic (dysphagia, bleeding) can resect with endoscopy or cervical incision |
|
|
What do you NOT do in caustic esophageal injury |
No NGT, no vomiting, nothing to drink |
|
|
What is worse an alkaline or acidic ingestion |
alkaline -->deep liquefacation necrosis, predisposes to cancer |
|
|
What type of necrosis does acidic ingestion cause? |
coagulation necrosis, causes gastric injury |
|
|
What is the treatment algorithm for a caustic ingestion? |
CT scan: look for free air, signs of perforation Endoscopy unless high suspicion of perforation. Do not go past site of severe injury |
|
|
What is the management of a primary burn injury to esophagus? |
See hyperemia Observation and conservative therapy. No oral intake until 3-4 days. Antibiotics May get cervical strictures (need dilations) or GERD (foreshortening) |
|
|
What is the management of a secondary burn injury to esophagus?
|
See ulceration, exudates and sloughing prolonged observation (same as primary), TPN |
|
|
Indications for esophagectomy in caustic injury to esophagus |
sepsis, peritonitis, mediastinitus, free air, stomach wall air, crepitance, contrast extrav, PTX, large effusion |
|
|
What is the management of a tertiary burn injury to esophagus? |
deep ulcers, charring, luminal narrowing often need esophagectomy |
|
|
Do you repair caustic perforations of the esophagus? |
NO. need esophagectomy as damage too extensive |
|
|
Most common cause of esophageal perforation? |
Iatrogenic (EGD) Cervical esophagus near cricopharyngeus muscle most common site |
|
|
What is the management of suspected esophageal perforation? |
CXR to look for free air Gastrograffin swallow, then barium swallow (not endoscopy) |
|
|
Criteria for nonsurgical management of esophageal perforation. |
Contained perf as demonstrated by contrast, self draining, no systemic symptoms NPO, IVF, Spitting, broad spectrum Abx |
|
|
What is the treatment for non-contained esophageal perforations dx in < 24 hrs? |
repair primarily and leave drains. Do longitudinal myotomy to evaluate injury, perform intercostal muscle flap to cover repair |
|
|
What is the treatment for non-contained esophageal perforations dx in >48hrs |
Depends on location Neck: Do not perform esophagectomy. Place drains Chest; resection with repair or exclusion and diversion with delayed repair (cervical esophagostomy, staple across distal esophagus, washout mediastinum, place chest tubes – late esophagectomy at time of gastric replacement) |
|
|
Where is Boerhaave's likely to perforate? |
left lateral wall of esophagus 3-5 cm above GE junction |
|
|
What is Hartmann's sign? |
mediastinal crunching on auscultation |
|
|
What esophageal perforation has the highest mortality? |
Boerhaaves. often perforates in distal esophagus--> left pleural effusion |
|
|
What two secreted factors lead to the most damage in GERD? |
gastric acid and pepsin |
|
|
What percentage of patients with symptomatic GERD have no evidence of esophagitis? |
30% |
|
|
What causes esophageal injury in GERD? |
Acid and pepsin |
|
|
study that reveals recurrence of hiatal hernia postoperatively |
Upper GI |
|
|
Which hiatal hernias should be repaired? |
Type 2, 3,4 |
|
|
What are the 3 anatomic areas of esophageal narrowing? |
Cricopharyngeus muscle Compression by the left mainstem bronchus and aortic arch Diaphragm |
|
|
What initiates a swallow? |
CNS |
|
|
What is primary peristalsis in swallowing? |
food bolus and swallow initiation |
|
|
What is secondary peristalsis in swallowing? |
occurs with incomplete emptying and esophageal distention propogating waves |
|
|
What is tertiary peristalsis |
non-propogating, non peristalsing (dysfunctional) |
|
|
What are the steps of swallowing? |
soft palate occludes nasopharynx, larynx rises and airway opening is blocked by epiglottis, cricopharyngeus relaxes, pharyngeal contraction moves food into esophagus; LES relaxes soon after initiation of swallow (vagus mediated) |
|
|
What do you do in a patient that has a perforated esophagus with a history of severe intrinsic disease? |
may need to do an escophagectomy |
|
|
Treatment of leiomyosarcoma? |
esophagectomy |
|
|
How do you diagnose a leiomyoma? |
esophagram, EUS, CT scan (to rule out cancer) |
|
|
What is contained in the fluid of a chylothorax? |
lymphocytes, TAGS |
|
|
Treatment for a postoperative chylothorax? |
Drainage, NPO, TPN, short chain FAs x 1-3 weeks thoracic duct ligation on right side low in mediastinum if >2L per day or refractory |
|
|
What is the postop chemo regimen for esophageal cancer? |
cisplatin and 5FU in node positive dz |
|
|
What margins do you need in an esophagectomy for cancer? |
6-8 cm |
|
|
What nodal involvement is a contraindication for esophagectomy? |
supraclavicular or celiac nodes (M1 disease) |
|
|
most important prognostic indicator in patients with esophageal cancer? |
nodal status |
|
|
What do you see on pathology in patients with Barret's |
goblet cells |
|
|
What is the key maneuver for dissection during a Nissen? |
finding the right crura |
|
|
What is the key maneuver for performing a Nissen wrap? |
finding the left crura |