Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
27 Cards in this Set
- Front
- Back
|
Overjet
Overbite Overgrowth you get with these two conditions What to do with supernumary incisors Incisor fractures |
Upper incisors protrude rostrally in relation to lower incisors.
Upper incisors also lie in front of lower. 106, 206, 311, 411 Leave them - long roots, hard to differentiated from normal. Tetanus anti-toxin. 7-10 day antibiotics. Endodontics at specialist or debride exposed pulp and apply calcium hydroxide paste. Young - normally seal off with tertiary dentine without treatment and continue to erupt normally. |
|
|
EORTH
|
Equine odontoclastic tooth resorption and hypercementosis - painful, canine and incisors - older horses, causes periodontitis, resorptive or proliferative changes of dental tissues. No treatment. Loose and painful teeth should be removed.
|
|
|
Retained 'caps'
Causes of diastema |
Remnants of deciduous cheek teeth. Occurs between 2-5yo. Can remove with special cap extractor or long slim elevator. Eruption cysts (3/4yo bumps) due to prolonged retention. Abscessation may occur - early, treat with 2-3 weeks of TMPS.
Lack of angulation of rostral and caudal cheek teeth, dental buds develop too far apart. Widen and pack with impression material. |
|
|
What should you do with small and large overgrowths?
Shear mouth Wave mouth Step mouth Smooth mouth Must all loose teeth be extracted? How often should teeth be examined? |
Small - rasp with carbide rasp. Large - power float and reduce by 3-4 mm a few months apart as could hit pulp otherwise.
Where sharp enamel points merge into steeply angulated (>45o) occlusal surface. Uneven or undulating occlusal surface. After tooth loss, opposing tooth erupts more rapidly. Absence of enamel on occlusal surface of CT in older horses. Can't grind food properly. Cupped out. Senile excavation. No, if due to overgrowths, may reattach once overgrowths gone. Every 6 months. |
|
|
Anatomy of cheek teeth
Where do you find the infundibulum |
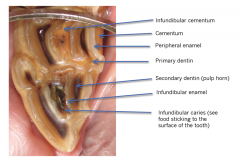
Maxillary teeth
|
|
|
Periodontal disease
|
Only due to eruption of permanent dentition - transient inflammation of periodontal membrane.
Canine teeth - calculus. Secondary to diastema or malocclusions |
|
|
What should you do with a horse with damage to the cheek teeth reserve crowns?
Pattern of idiopathic fractures of CT Midline fractures of maxillary CT |
Conservative therapy. 1-2 weeks antibiotics andfeeding soft diet. Extraction delayed for a few months whilst any other fractures (jaw) heal.
Lateral slab fractures through two lateral pulp cavities. Secondary to advanced infundibular caries. |
|
|
What is indicated with all dental treatments?
What are apical infections usually caused by? What predisposes to them? Infections of caudal 4 maxillary teeth can lead to what? |
Tetanus prophylaxis
Blood or lymphatic infections. Inflammation of the pulp due to impaction. Secondary sinusitis. Chronic malodorous unilateral nasal discharge. |
|
|
How can you extract a cheek tooth?
What is the advantage of endodontic treatment? |
Repulsion - damage to alveolar bone and mandible/maxilla, risks of infection
Lateral buccotomy - Approach through skin and subcutaneous tissue into the alveolus. GA. Haemorrhage, facial paralysis, fistula formation. Oral - standing. Romifidine and butorphanol. Local anaesthesia maybe too. Detach gum around affected tooth at level of alveolus, separator, extractor and pull (20-30 minutes) with forceps once digitally loose. Pack with antibiotic soaked swab and remove in 2 weeks. Tooth can continue to erupt normally. Apex or occlusal surface. |
|
|
What is dysphagia?
What causes it? |
Difficulty swallowing
Oral cavity - pain (teeth), - quidding, tongue (paralysis of CN XII, botulism, restraining horse by tongue), tumours Pharynx - Masticated food both nostrils, coughing due to aspiration. Congenital neonatal neuromuscular dysfunction, cleft palate, GP mycosis, Strangles, botulism, heavy metal poisoning (lead), naso-pharyngeal FBs, naso-pharyngeal tumours, GP disease. Oesophagus - Choke, stricture, diverticulum, perforation |
|
|
Guttural pouches
What are they? Guttural pouch mycosis Which bvs/ns can be affected - symptoms related to these. How can haemorrhage be stopped? Treatment Prognosis |
Eustachian tube diverticulae
Aspergillus fumigatus, invades roof of guttural pouch - destructive and secondary bacterial infections. Blood or mucopurulent discharge from ostium. Grey, black or white fungi. Cranial sympathetic nerve - Horner's syndrome CN7 - Facial paralysis (v rare) CN9, 10, 11 - Pharyngeal paralysis. Laryngeal with 10. 12 - Tongue paralysis (v rare) Internal carotid, internal maxillary artery, internal maxillary vein, external maxillary artery - massive haemorrhage. Balloon or embolising coil up internal carotid to beyond sigmoid flexure to prevent back bleeding then ligating at origin. Natamycin/enilconazole, sprayed onto roof of pouch daily 2-3 times. Depends on nerves damaged. Cases with pharyngeal dysphagia have poorest prognosis. |
|
|
Other guttural pouch conditions
GP empyema/chondroids GP tympany |
Sequel to strangles, abscessation and drainage of retropharyngeal lymph nodes into GPs which have poor natural drainage. Extensive swelling can interfere with airflow - tracheostomy; and can cause dysphagia. Chronic - empyema/chondroids - chronic purulent discharge. Feed from ground. Lavage with lukewarm, very dilute antiseptics. Transendoscopic removal of chondroids or drainage - ventral.
Congenital. Neuromuscular defect or abnormal tissue fold at nasopharyngeal ostium act as one way valve. Unilateral - foley catheter for a few weeks to distort ostium. Or window. Bilateral - surgical enlargement of one of ostia and GP septal perforation or fistula between roof of pharynx and GP. |
|
|
How should you deal with a case of oesophageal choke?
Strictures Diverticulum Perforation |
Sugar beet pulp or pellets. Take off bedding, muzzle, spasmolytics, sedatives (ACP or romifidine and buscopan). Safe for 24 hours. If not cleared - lavage oesophagus. Avoid aspiration - penicillin and metronidazole. If still not clear - sloping table, cuffed ET tube, lavage. Can develop ulceration then stricture if over 36-48 hours.
Balloon dilation - likely to form other strictures. Euth in some. Developmental or rupture of muscular layers. Outpouching (pulsion) or scarring and adhesions (traction). Invert lumen with pulsion and mesh. Risk or recurrent laryngeal nerve damage with this surgery. Traction may heal by second intention healing. Kick, ven |
|
|
Surgical colic
Stomach Non-strangulating lesions of small intestine Strangulating obstructions of small intestine Where can the SI become entrapped? Caecaum Colon Small colon and rectum |
Pyloric stenosis, gastric impaction/dilatation
Ileal/jejunal impaction, intestinal neoplasia,anterior enteritis Pendunculated lipoma, small intestinal volvulus,intussusceptions, thromboembolic colic, SI entrapment Epiploic foramen entrapment, inguinal/scrotal hernia, herniation through mesenteric rent, gastrosplenic ligament, umbilical hernia, diaphragmatic hernia. Caecal impaction, caecocaecal and caecocolic intussusception (can become strangulating as can pass into RVC and draws in caecocolic artery. Caecal infarction. Left dorsal displacement - nephrosplenic entrapment, right dorsal displacement (left colons round body of caecum clockwise or anticlockwise. Colon volvulus/torsion. Enterolithiasis (rare). Atresia coli, small colon impaction, rectal prolapse, rectal tears. |
|
|
First aid for rectal tears
|
Sedate. Epidural or large volume local anaesthetic per rectum. Evaluation and packing. Broad spectrum antibiotics, non-steroidals, referal/surgery in severe.
|
|
|
Causes of ileus
Leads to Diagnosis Treatment Complications |
Inflammation, distension, denervation (grass sickness).
Further distension and pain, dehydration. Rectal or abdominal ultrasound - distended loops of SI with little movement. Reflux. Reflux, supportive therapy, motility stimulants (lignocaine, cisapride, metaclopramide). Stomach may rupture if not refluxed regularly. |
|
|
When should open castration not be performed?
Technique of open Closed Complications |
>4yo, cryptorchid, fractious, donkey
Sedation, analgesia, LA into cord and testicle. Wash. Long deep midline incision over each testicle through ventral skin, subcut scrotal tissues (dartos) and external tunic. Section avascular caudal ligament to exteriorise. Emasculator - spermatic cord transected and crushed. Kept in place 2-4 minutes. Single or two incisions through skin and subcutaneous tissue but not through tunic. Dissection to 10-15 cm below testicle. 2 transfixing ligatures of 4-6 metric absorbable material 2 cm apart. Emasculated 2cm distal to last ligatures. Haemorrhage - count drops, not steady stream. Artery forceps - leave for 24 hours or ligate with absorbable sutures. GA if still bleeds. Post op infections - Tetanus, strep zooepidemicus. Oedema - hand walk 2-3x daily, NSAIDs - phenylbutazone 3-5 days. Evisceration. |
|
|
How do you determine if a horse is cryptorchid?
|
>3 - resting plasma oestrone sulphate
Younger <3 - two blood samples one prior and one 20-30 mins after HCG. Significant rise in testosterone if testicle present. |
|
|
Differentials for epistaxis
Treatment |
Non-traumatic - EIPH, guttural pouch mycosis, ethmoid haematoma
Traumatic - turbinates hit during passing of tube. head trauma - rectus capitis muscles - bleed from pouches. Deep bedded dark box, closed top door for 15 minutes. Packing nose only if more than a few litres shed. |
|
|
What is the most common cause of unilateral nasal discharge?
Aetiology |
Sinusitis
Primary infective sinusitis (URT infection - antibiotics, lavage with dilute iodine or saline - may become inspissated), dental apical infection (08-11s -extract offending tooth) or oro-sinus fistula, maxillary sinus cysts (marked swelling), sinus neoplasia, mycotic sinusitis, sinus trauma, intra-sinus PEH lesions. |
|
|
What can cause pharyngeal paralysis?
Intermittent dorsal displacement of the soft palate (gurgling). (Permanent is rare). |
GPM - CN9,10,11; congenital neuromuscular pharyngeal defects, severe strangles infection, hypocalcaemia, lead poisoning, botulism, grass sickness
Very fast exercise. Displaces dorsal to epiglottis - causes airflow obstruction (mainly expiratory). Reduced exercise performance. May be silent. Primary dysfunction of intrinsic palate muscles (tx -fibrose), dysfunction of thyro-hyoid muscle (tie forward), excessive caudal retraction of larynx (myectomy or tongue-tie), damage to pharyngeal branch of vagus nerve (rest, treat inflam/URT infection), epiglottic hypoplasia, excessive tissue flaccidity. |
|
|
Epiglottis
Epiglottic entrapment Subepiglottic cysts Epiglottic retroflexion |
Pouch of mucosa. Treat by sectioning the entrapping membrane. Standard breds (TBs)
Deviate epiglottis dorsally causing airway obstruction. Surgical excision Dorsally angled epiglottis, can get sucked back. |
|
|
Recurrent laryngeal neuropathy (RLN), idiopathic laryngeal hemiplegia, idiopathic laryngeal hemiparesis, laryngeal paralysis (Roaring, whistling)
Treatment |
Idiopathic degenerative neuropathy of the left recurrent laryngeal nerve that innervated the intrinsic laryngeal muscles. Loss of adductor function - no clinical signs. Abductor dysfunction - unable to fully open larynx during exercise. Unilateral can be associated with GP mycosis or damage. Whistle or roar. Don't evaluate in sedated horse.
Mild cases - vocalcordectomy or ventriculectomy. Severe - laryngoplasty (tie-back)prosthesis acts as new CAD muscle. Others - arytenoidectomy, laryngeal re-innervation, tracheostomy, retire. |
|
|
Tracheal collapse
|
Small ponies - stridor, dyspnoea, exercise intollerance. Cartilage deformity or degeneration of dorsal trachealis ligament. Tracheal stent, keep quiet and rested during episodes.
|
|
|
Sarcoids
Types Treatment |
Most common neoplasm effecting horse. Benign but can be locally aggressive. BPV. Spread by flies. Can grow anywhere but common on head, groin, prepuce, axillae, neck.
Occult - thickened skin with roughened surface, often hairless and very slow growing. Verrucous (warty) - dry, horny, cauliflower-like, broad base or pedunculated. Fibroblastic - looks like proud flesh. Firm and nodular, ulcerated. Mixed Nodular - entirely under the skin - can be shelled out. Malevolent sarcoids - rare, most aggressive type. Tumours spread extensively through skin with cords of tumour tissue interspersed with nodules and ulcerating fibroblastic lesions. Nothing, surgery, cryo, BCG very good for periocular, radiation, Liverpool sarcoid cream, intralesional chemotherapy, combination therapy. |
|
|
Can melanomas progress? Treatment
SCC Papillomatosis |
Yes. Leave, excision, cryotherapy, cimetidine (x3 a day for 3 months), chemotherapy
UV radiation, chronic irritation, previous wound, smegma. Excision, cryotherapy, radiation therapy, chemotherapy. Malignant - only treat if haven't metastasised. <2 yo. Papovavirus. Older horses if immunologically naive. Face, head. Regress spontaneously in 3-4 months. |
|
|
What to do with excessive granulation tissue
Skin grafts Preparation of site Types Reasons for failure |
Bandage with moderate pressure, excision of excess tissue, topical steroids - not if infected, biological dressings. Don't use cauterising compounds.
Fresh or granulating wound. Debride. Don't graft if infection present. Topical treatment of recipient site after initial debridement for 1 or 2 bandage changes prior to grafting. Pinch/punch grafts, tunnel grafts, split thickness grafts, full thickness grafts. Excessive movement and infection. Both lead to fluid accumulation between graft and site, prevents adherence. Inadequate preparation (too thick?) or recipient site. |