![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
63 Cards in this Set
- Front
- Back
|
what are the 4 methods evaluating if it is actually a confounding association? |
1. stratification- if potential cofounder's stratum specific are simiar, calculate adjusted RR/OR and see if differs from crude 2.multivariable analysis- control for potential confounder in multivariable analyss and see if adjusted RR/OR differs from crude RR?OR 3. standardisation 4. matched analysis |
|
|
steps for stratification |
1. calculate the measure of association between the measruement and outcome (crude, univariat or unadjusted) 2. divide exposire by strata level of potential confounder 3. for each stratum, calculate the measure of association between the exposure and outcome (calculate the stratum-specific measures of association) 4. compare stratum-speicific measures of association |
|
|
stratification picture illustration |
|
|
|
stratification pros and cons |
pros: - easy for small numner of variables with limited number of strata - permits evaluation of confounding - permits evaluation of effect modification cons: - usually some residual confounding - not feasible for dealing with lots of variables with many strata |
|
|
what is multivariable anaysis |
- efficient for estimating the measure of association whilst controlling for multiple potential confounders - works in situations where stratification won't - specific techniques vary dependsing on data types- multiple regression, poison regression... etc |
|
|
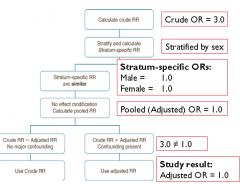
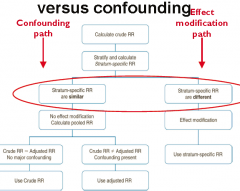
picture illustration of modification vs confounding |
|
|
|
what is the general guideline for confounding evaluation |
if controlling for confounding changes the measure of assocaition by 10% or more, we generally consider that confounding was afecting the association |
|
|
residual confounding |
due to unmeasured or imperfectly measure confounders (need to consider the impact of this) - you can only control what you've measured (if you haven't measured it, most likely ave no clue) |
|
|
how can you control confounding in design? analysis? |
design: randomisation restriction matching
analysis : stratification multivariable standardisation macthed analysis |
|
|
using unmatched analysis leads to under-estimation of the OR |
so confounding can lead to distortion of the true association |
|
|
what does an effect modifier do? |
measure the effect between the exposure and the outcomeat different strata of the effect modifier |
|
|
what are some ethical ideas that patient, investigator and physician have to bear in mind? |
patient: right state in mind, no mental patients investigator- treat every partient faily physician: act if he were thinking of himself |
|
|
what are some ethical failures? |
- harm to men, no consent, deception, inducement, exploitation of vulnerable group, scientific misconduct, no monitoring or stopping the study, conflict of interest, harm in the design of a study |
|
|
how do we prevent unethical studies? |
- moral emphasis in prefessional training - codes and guidelines |
|
|
what are the 6 NEAC guidelines? |
1. respect for person- automy 2. justice 3. beneficience, and non-maleficience 4. integrity 5. diversity 6. addressing conflict of interest |
|
|
what are the current ethical codes? |
international: declaration of helsinki NZ: national ethics advisory committee |
|
|
respect for persons |
rights of individual privacy and informed consent. right to withdraw from study |
|
|
justice |
fair distribution of the benefits and burdens of participation in a study
|
|
|
beneficience and non maleficence |
do good, do not harm. benefits should outweigh harm- clinical equipoise |
|
|
integrity |
conduct honest, thoughtful inquiry and rigour analysis accept responsibility of action |
|
|
diversity |
investigators undertstand, respect and recognise diversity among participants |
|
|
addressing conflict on interest |
- professional judegement concerning a primary interest - influenced by secondary interest |
|
|
you have to inform the consent what are the two types? |
1. direct or substitute 2. if the person has a legal guardian, need a substitution
it should always be obtained in writing |
|
|
what are the three elements in consent |
1. capacity- ability to understand , evaluate and make decision to participate or not greater than 18 2. information. is it complete and fully understood appropriate reading leel on information sheet (plain language) 3. voluntariness (free power and will and have the choice to withdraw) |
|
|
what are the 5 types of vulnerable groups. |
1. foetus/pregnant women 2. older people 3. diabilities 4. prisoners 5. children |
|
|
informed consent children, what extra needs to be done? |
another copy of consent form is needed for partient, guardians |
|
|
define equipoise within a clinical trail |
- the evidence is eually poised as to the overall balance of risks and benefits of each of the interventions offered in the study - it can not be determinded inadvance which the groups in the proposed study will be better off |
|
|
how did concepts about the research ethics come into existence |
- a moral framework for professional behaviour that does back to hippocrates - violation of mora precepts led to the development of codes and guidelines |
|
|
origins of human subject research study |
hippocrates medical practice and medical ethics, physicians should abstain from whatever os mischievous and deleterious - doess not deal with research with humans, does not mention the principle of informed consent |
|
|
berlin medical association- more of a patient treatment perspectiverather than research 1928 |
ethical code develop, a ot of unethical for the nazi doctors mainly concerned with experimental research 1964 helsinki |
|
|
what is the defnition of screening |
examination of a group to separate well persons from those who have an undiagnosed pathologic condition or who are at high risk. |
|
|
what is the purpose of screening? |
- identify disease before it would normally be diagnosed - reduce mortality and morbidity - to limit the impact of the disease on comunity - to identify a compensable disability |
|
|
what are the five principles of screening |

|
|
|
what are the other five principles |

|
|
|
two types of screening |
- organised (proactive) screening (target population invit to attend for testing) - opportunistic screening (person present to a doctor for another reason) |
|
|
framework |
well vs sick financial incentives ethics of screening |
|
|
additional qa reqired |
those with positive results need further investigation |
|
|
current screening policies 4 types |
1. cervical screening 3 years ages 20-69 2. breast cancer: 2 years two view
mammographyy age 45-69
3. colorectal cancer screening, flexible |
|
|
what are the other cancer screening? |
lung cancer skin cancer ovarian cancer oral cancer |
|
|
diagrame |

|
|
|
informed consent |
- the procedure - risk to benefit ratio - ensure awareness of possiblity of erroneous result - discuss subsequent management of abnormalities detected - inform about need for screening |
|
|
advantages of flexibility sigmoidoscopy |

|
|
|
4 points about screening frequency |
- average lead time - distribution of lead times obtained by screening - availability of resource - acceptability |
|
|
screening test reliability |
cosistency of results when repeat examinations are performed on the same person under the same condition - biological variability (blood pressure) - method or measurement variability - intraobserver variability - interobserver variability |
|
|
what are the four main areas of failure in screening |
- a low uptake of screening by those at risk - the frequency of false negative results - the failure to act on abnormalities detected at screening - the failure of the treatment of abnormalities detected |
|
|
what are the benefits of screening? |
- improved prognosis for some cases detected by screening - less radical treatment which cures some cases - resource savings - reassuracne for those with negative tests
|
|
|
what are the harms of screening |
- longer morbidity for those prognosis is unchange - over-treatment of questionable abnormalities - resource costs - false reassurance for rhose with false negative results - anxiety and sometimes morbidity for those with false positive results - hasards of screening test |
|
|
what are the rganisational requirements? |
- managerial guidelines for screening programmes exist - need for recognition as public health programmes - public health leadership - respect from and for clinicians
|
|
|
how to monitor of the cervical screening programme
|
- a set of indicator and perforamce target have been aggreed - the independence monitoring group measures the performance of the programme against these targets |
|
|
what are the two main types of association? |
1. non-causal- due to chance, bia or confouning 2. likihood of an outcome occurring depends on the presence of the exposure |
|
|
what are the three causal factors |
1. component cause- facotr contributes towards disease causation but not sufficient to cause disease on its own 2. sufficient cause- factor that inevitably initiate or produces disease 3. necessary cause- factor required for development of a given disease/outcome |
|
|
facts about component causes |
- very few componetn causes are necessary and sufficient - more commin s necessary... or vise versa |
|
|
why do causal association matters? |
- causal pies indicate component causes to target - targeting component causes for interventions and public health action - should be amenable to modification |
|
|
bradford hill criteria list all 7 |
1. temporal sequencing 2. strength of association 3. consistency 4. biological plausibility 5. specificity 7. experiment evidence |
|
|
temporal sequencing |
exposure must precede outcome best demonstrate in cohort RCT and most case control |
|
|
strength of association |
the stronger the association the less likely it is to be bias or confounding
but a small effect seen consistently may still be causal. if exposure common or too rare- hard to rule out confoudning |
|
|
consistency |
the same result found across different study designs suggest unlikely to be due to chance, bias or confounding
but lack of consistency can be due to a range of factors other than causality |
|
|
dose response relationship |
if the risk of developing the outcome changes with the level of duration of the exposure, supports causal association
but not always linear
|
|
|
biological plausibility |
a plausible biological mechanism for the effect of the exposure on the outcome can support causality
but lack of plausible mechanism may be due to current stage of knowledge |
|
|
specificity |
if an exposure is specifically related to one outcome, this supports causality
but many exposures are causally associated wih a variety of outcomes |
|
|
experimental evidence |
well designed and conducted ransomised conrolled trails provide strong evidence for causality
but often not always feasible or ethical so have to rely on other study designs |
|
|
cohernece |
ssociation should not conflict what is already known. a |
|
|
analogy |
relating to known causal associations, can make an analogy to anything |