![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
287 Cards in this Set
- Front
- Back
|
Define Endocrinology |
isthe study of the endocrine system, secretions and their role at target cellswithin the body. The endocrine and nervous system are the major contributors tothe flow of information between cells and tissues |
|
|
What two systems maintain homeostasis |
Nervous system endocrine system |
|
|
The endocrine system maintains a complicated relationship with both the _______ system and the ______ system to assist in development, growth, and metabolism |
The endocrine system maintains a complicatedrelationship with both the nervous systemand immune system to assist indevelopment, growth and metabolism |
|
|
The endocrine system uses what to convey different tissues |
Hormones (chemical messengers/neurotransmitters) |
|
|
Hormones transport via the bloodstream to target cells within the body. It is here that they bind to receptors on the cell surface. T/F |
True |
|
|
Could a neurotransmitter be a hormone? |
Yes,epinephrine- produced in the adrenal gand. Neurotransmitter and released intothe blood stream to go to distant locations to have its effect |
|
|
Do hormones have any nutritional value ? |
No, they are non-nutritive |
|
|
What system consists of a variety of glands working together? |
Endocrine Sytem |
|
|
What type of effects arelocalized actions resulting from cell to cell communication? Is it mechanical or chemical? |
The paracrine effect.Chemical |
|
|
An ________ is a molecule released by infected cells to bind to other cellsto give some aspect of immunity against the virus. This is described as a _________ solution since it is Released into tissue and has it's affect locally |
An Interferon is a molecule released by infected cells to bind to other cellsto give some aspect of immunity against the virus. This is described as a paracrine solution since it is Released into tissue and has it's affect locally |
|
|
Hormonesreleased by cells that act on the membrane receptor on the same cell tomodify its activity is called the ______ effect |
Autocrine |
|
|
An__________solution releases vesicles to the surface and then there are receptors for that specific molecule and the vesicles bind and down regulates the receptors of that molecule |
An autocrine solution releases vesicles to the surface and then there are receptors for that specific molecule and the vesicles bind and down regulates the receptors of that molecule |
|
|
Will endocrine secretions ever be released outside of the body? |
no |
|
|
Endocrine secretions are secreted into the _____ _______ |
blood stream |
|
|
Endocrine secretions Usually results from a ductless gland, thus,contents are dumped into the ________ _______ |
extracellular space |
|

Endocrine Secretions cont... From the picture. Why do we seewater stay in the capillary bed and not go out? |
- Higher solute concentration inside thecapillaries. There is a larger number of solutes inside the capillaries thenthere is outside. The water is kept inside that capillary bed preventing itfrom going out. -Fluid flow out from the heart- Hydrostaticpressure (I think) - Fluid going in is osmotic pressure - If we release hormones from the cells (blue) 80x more fluid flow goes in the direction of the orange arrow than going down thecapillaries. The membranein the capillary is non restrictive. Anything will move across it |
|
|
What type of secretion releases its contents outside of the body? The secretion will be released into a specific part of the body |
Exocrine secretion |
|
|
exocrine secretion comes from a gland with a _____ |
duct |
|
|
Exocrine Secretions: what has a message transmission directly from cell to cell, is local, and specificity depends on anatomic location. |
Gap Junctions |
|
|
exocrine secretions: what has a message transmission across a synaptic cleft, is local, and specificity depends on anatomic location and receptors it is aspace; chemical messenger allows us to transfer information from one cell tothe next. |
synaptic |
|
|
A synapse can happen on 1 of 3 things. What are they? |
Synapse on another nerve Synapse on a muscle Synapse on glandular tissue |
|
|
Exocrine secretions What has a message transmission by diffusion in interstitial fluid, can diffuse locally, and specificity depends on receptors Interferon and Prostaglandins are an example |
Paracrine |
|
|
Exocrine Secretion: What has a message transmission by circulating bodily fluids, is general, and specificity depends on receptors. It releasesits secretions into the interstitial tissue space but then diffuse easily intothe capillary beds and the rest of the body. |
Endocrine |
|
|
What organ is considered both exocrine and endocrine? |
pancreas-10% is endocrine. 90% of mass is exocrine- the pancreas releases its contents to the lumin of the duodenum and it produces/releases digestive enzyme's (proteases, pancreative lipases etc…) - They are released to the lumin of the small intestine and some of them will be excreted which is why it is called an exocrine tissue: released via a duct which will eventually be released to the outside of the body |
|
|
What are the functional units of the nervous system? |
Neurons |
|
|
The Nervous system maintains a ____ response, but the effects are _____ lived |
The nervous system maintains a fast response, but the effects are short lived |
|
|
The nervous system is composed of both the ____ and _____ systems |
somatic and autonomic systems |
|
|
The somatic nervous system travels to |
to the skeletal muscle |
|
|
The autonomic systems go to the |
cardiac muscle, smooth muscle, and glands |
|
|
The endocrine system will release hormones to the bloodstream in a _____ manner |
ductless |
|
|
The endocrine system has a ____ response, but the effects are much _______ lasting |
The endrocrine system has a slow response but the effects are much longer lasting |
|
|
Does the endocrine system maintain direct contact with the affected cells? |
no |
|
|
What is defines as a combination of both nervous and endocrine system |
neuroendocrine |
|
|
The neuroendocrine system has specialized neurons that release chemicals that travel through the vascular system and interact with target tissue. they are released just like a neurotransmitter, bind like a neurotransmitter, but might not have an immediate effect |
just info |
|
|
What is not only a neurotransmitter, but also a neurosecretion? |
Epinephrine |
|
|
Who was the father of endocrinology? |
Bertold |
|
|
What experiment did bertold perform to study male behavior |
1. Castrated roosters failed to develop normal size combs and wattles (would be reduced in size and turn pink instead of normal red) along with a failure to exhibit normal male behavior. Would be docile, not as territorial or aggressive. 2. Removed testes and observed a decrease in aggression 3. Re-implanted testes and noted a return of the traits and characteristics, wattles and combs were larger and darker red. Aggression returned and normal behavior returned. |
|
|
Bertold also found that he didn't have to implant both testes into the rooster. If he implanted just one then the testicle grew significantly larger than if there were two testes. This happens to compensate for the loss of the other testicle. The one testicle produced enough for the two that were removed. What is this called? |
Compensatory Hypertrophy |
|
|
Who was the first to describe diabetes mellitus by removal of the pancreas? |
Von Mering and Minkowski Diabetes was usually a death sentence. They worked on dogs, removed their pancreas and the dogs developed the signes and symptoms of type 1 diabetes |
|
|
What are the common signs and symptoms of Diabetes Mellitus? |
Frequent urination feeling thirsty (Polydipsia) fatigue Hunger |
|
|
What did Banting and Best discover? |
They discovered that insulin was produced in the cell of the pancreas and named it islutin |
|
|
What is the definition of homeostasis? |
The tendency for physiologic systems to maintain consistent internal environments. |
|
|
Equilibrium is maintained through ________ _______ _______ |
negative feedback mechanisms |
|
|
Small fluctuations, such as temperature fluctuations, are the result of _____ _____ |
negative feedback |
|
|
An increase in one hormone will lead to a _____ in another hormone produced |
decrease |
|
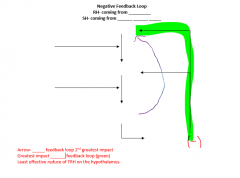
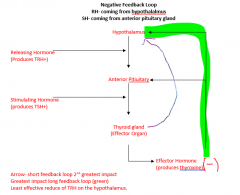
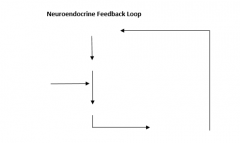
Fill in this negative feed back loop chart |
|
|
|
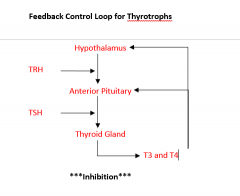
Which feedback loop has the greatest impactonthe feedback loop? |
Long feedback loop Thyroxine T3, T4 |
|
|
Long feedback loop: Thyroxin (effector hormone) will have a ______ effect at the hypothalamus by decreasing additional production of TRh |
Significant |
|
|
Short feedback loop: TSH secreted from the anterior pituitary gland will have a _____ greatest at the hypothalamus by decreasing additional production of TRH |
Second |
|
|
Which part of the feedback loop has the smalles impact on the Feedback loop?
|
Very short feedback loop. |
|
|
Very short feedback loop: TRH secreted from the hypothalamus will have the _______effect at the hypothalamus by decreasing the additional production of additional TRH |
least |
|
|
Does positive feedback happen more or less frequently when compared to negative feedback |
less frequently |
|
|
What causes positive feedback? |
it results when an initial trigger significantly increases the production of a hormone. The production continues until the initial trigger is eliminated |
|
|
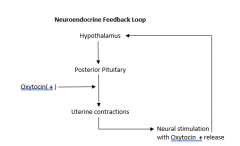
What are two major examples of positive feedback |
i. Increase in cortisol production leads to an Increase in oxytocin production hormone release to increase in uterine contraction followed by infant delivery ii. Clotting- cut ourselves, initial stimulus, we initiate a clotting response until we eliminate the bleeding |
|
|
|
|
|
|
|
|
Oxytocin will continue to increase until the baby is delivered followed by a decrease in release. Oxytocin can continue to be released until most of the milk has been depleted. T/F |
True |
|
|
What is a chemical structure on thesurface of a cell or inside a cellthat binds the hormone to initiate some change within the cell i.e. cellexcitation via depolarization (i.e. opening of ion channels followed by localdepolarization), activation of intracellular pathway and/or protein synthesisvia transcription and translation (i.e. anabolic steroids) |
Receptor |
|
|
Creatine Monohydrate has two main mechanisms of action. What are they? |
1. Keeps phosphates bound in muscle tissue. Shuttles creatine into the muscle cells which keeps the phosphates available to bind to AMP and ADP to make ATP 2. Serves as an osmotic agent |
|
|
There are two types of receptors. What are they? |
steroid receptors protein receptros |
|
|
What are some characteristics of steroid receptors? |
1. Intracellular/do not bind to the cell membrane 2. located within the cell and interact with hydrophobic structures/cytoplasmic receptors 3. Steroid analogs can pass through the cell membrane and interact with intracellular receptors inside the cell. 4. Steroids are made from cholesterol |
|
|
Steroids cannot easily make it through the cell membrane. How do they get through? |
Cholesterol makes up 13% of all cell membranes which provides fluidity in the cell membrane. The function of cholesterol in the cell membrane is to push the phosphate heads apart which allows for the steroids to travel to the inside where it is hydrophobic, just like steroids, so they feel comfortable there. |
|
|
Where are protein receptors located? |
on the cell surface |
|
|
What do protein receptors that are located on the cell surface interact with? |
hydrophilic receptors |
|
|
What is released form nerve cells and is a short lasting signal that is transmitted to a local area via an electrical impulse. They are chemical messengers that bridge the synapse |
Neurotransmitters |
|
|
What is an example of a neurotransmitter |
epinephrine and norepinephrine |
|
|
How does epinephrine work? |
epinephrine comes into the cell, activates adenycl cyclase and then converts ATP into CAMP (secondary messenger), then opens up an ion channel to allow sodium to come into the cell. |
|
|
Neurotransmitters work via a second messenger and then are further broken down locally. what is the second messenger and what breaks it down? |
second messenger: cCAMP broken down by PDE (Phosphodiesterase) |
|
|
What is a long lasting impulse which is produced by the hypothalamus/pituitary gland locally and at distant sites? |
neurosecretion Note: These are released by a cell that looks like a nerve, but has an effect like a hormone |
|
|
What are produced by glands and have longer lasting effects; effects can be observed at tissues located far away. Example: Epinephrine - released by the adrenal medulla into the blood stream to travel to all parts of the body for the fight or flight response |
hormones |
|
|
What is defined as the amount of time it takes to clear the hormone out of the blood stream and the effectiveness of the hormone? |
half life |
|
|
Do larger molecules or smaller molecules have a longer half life? |
larger |
|
|
What organs are hormones cleared by? |
The liver, some by the kidneys |
|
|
What are 8 physiological roles of hormones |
1. Affect cell synthesis and secretion 2. Affects Metabolism (both anabolic and catabolic metabolic processes) 3. Affects muscle function 4. Controls reproduction 5. Controls Cell growth 6. Affects the movement of cations (Na+, K+, and Ca+) 7. Play part on effectiveness of other hormones 8. Important in normal animal behavior. |
|
|
What is an example of how hormones affect cell synthesis and secretion? |
Increase in epithelial cell production and increase in milk production in the mammary glands |
|
|
What are the five main hormones of growth? |
insulin thyroid testosterone HGH IGF |
|
|
Hormones affect muscle function. An example is when a person is hypocalcemic they maintain low levels of Ca++ in their serum. Explain this. |
Too little calcium, we’ll go up to the threshold (0). If we get closer to that then it is an unstable membrane which can lead to arrhythmia or palpitations. Too much extracellular calcium is going to cause instability Calcium has to be in a narrow range to maintain proper cardiac muscle function. Every roid step in the clotting cascade requires Ca++ as a coenzyme, therefore, decreased serum Ca++ leads to instability |
|
|
What two hormones are important in normal animal behavior? |
testosterone and estrogen |
|
|
What are two modified amino acids and what does that mean? |
Tyrosine and Tryptophan. They will serve as the initial building block for some hormones. ie: Tyrosine can be modified to make thyroid hormone |
|
|
What are the 4 different classifications of hormones? |
modified amino acids
|
|
|
Whenwe add two peptides together we remove water via a ________ or _________ ________ |
Whenwe add two peptides together we remove water via a condensationor dehydration synthesis |
|
|
by breaking the peptide bond apart we will undergo a _______ reaction. |
hydrolysis |
|
|
How many amino acids do each have: Peptide Polypeptide Proteins |
Peptide:< 10 amino acids Polypeptide:10 – 50 amino acids Proteins:> 50 amino acids |
|
|
Glycoproteins are proteins with carbohydrates attachment. what are three examples?
|
FSH, TSH, HCG |
|
|
Glycoproteins have an alpha and beta subunite. What do they do? |
Beta subunit is for specificity alpha subunit is just consistent amongst all four hormones. |
|
|
Which hormones derive their structure form the cholesterol backbone? |
steroid hormones |
|
|
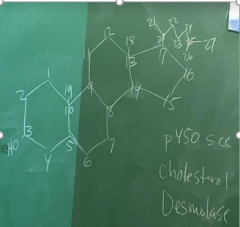
What is P450 Scc? |
cytokine cleavage |
|
|
If we remove the sidechain of cholesterol we will end up with? |
pregnenolone |
|
|
Cholesterol in the body accumulates in two different ways. What are they? |
through the diet through liver production (serum) - this is a genetically predetermined quantity that dictates the production by the liver. More important than the diet |
|
|
what is a drug that helps to decrease the absorption of cholesterol through the gut lining. |
zetia |
|
|
what inhibit an enzyme in the liver called Hmg CoA reductase which allows us to make cholesterol from fatty acids? What is the problem with them? |
Statins. The problem is that they increase the chance of rhabdomyolysis since were significantly increasing the amount of cholesterol in the cell membrane |
|
|
What drug pulls bad cholesterol out of the blood stream? |
repatha |
|
|
Serum cholesterol is carried in the blood in two distinct structures. what are they and define them. |
High Density Lipoprotein (HDL): Good cholesterol which has an increased amount of protein surrounding the cholesterol molecule. More protein/less fats Low density Lipoprotein (LDL)- bad cholesterol which has a decreased amount of protein surrounding the cholesterol. LDL density: More cholesterol/less protein |
|
|
what is the first structural modification to create a steroid hormone? |
Cholesterol |
|
|
Name two steroid characteristics |
they are fat soluble, but not water soluble circulatory concentration in ng/dL |
|
|
CIs cholesterol the initial cause of development of cardiovascular disease? |
No, it is an innocent bystander. It is involved in the healing process after. It is not the initial cause |
|
|
What are two main causes of endothelial damage? |
Increase in blood pressure Increase in endothelial inflammation from free radicals from the sugar that is being consumed |
|
|
mmodified fatty acids: eicosanoids- arise from ______ acid and from the phospholipid bilayer |
arachidonic acid |
|
|
Explain the arachidonic acid pathways |
the phospholipid bilayer uses phospholipase A2 to produce Arachidonic acid. From there 1 of three pathways are possible. 1. Arachidonic acid using COX to create prostalandin. - prostaglandins are local tissue hormones. Examples include PGE, PGA, PGF2alpha, They decrease in the size and function of the corpus luteum. possible correlation to menstrual cycles, incolced in smooth muscle contraction. (sidenote cox inhibitors will inhibit the formation of cyclooxygenase (COX) to produce prostaglandin 2. Arachidonic acid using LOX to create Leukotriens (aka: slow reacting substances of anaphylaxis) - leukotrienes are produced by WBC's - important in the development of asthma, allergies, and anyphylaxis (about 1000 times more potent than histimine) 3. Arachidonic acid uses 12-lipoxygenase to make HETE ( class of eicosanoids - inflammatory agentfound in metabolic syndrome, alzheimers, cancer, and general inflammation |
|
|
also involved in the arachidonic acid pathway Peroxidase can be split three ways into prastaglandins, prostacyclins and thromboxanes.explain what these do |
prostaglandin- involved in smooth muscle contraction thromboxane A2 is produced by damaged endothelium. we see dynamic constriction of the vessel wall. Significantly increases platelet aggregation- platelet clotting prostacyclins- produced by healthy endothelium. They cause vasodilation which decreases blood pressure and they decrease platelet aggregation so we don't have clotting occur where it shouldn't |
|
|
histamine is secreted by both mast cells and basophils. What happens during an anaphylactic reaction? |
mast cells and basophils release histimine and serotonin to increase capillary permeability which will increase inflammation |
|
|
what happens during an anaphylactic reaction? |
We could see massive swelling in this region, decrease in the ability to breathe from a narrowing or restricted passageway- Third spacing- if we release massive amounts of materials that cause increase in capillary permeability. The heart continues to pump blood pushing the fluid out of the vessels into interstitial tissue space causes: hypovolemic shock- a decrease in the volume of blood- death |
|
|
What determines the half life of a hormone? |
Their size. the bigger the molecule is the longer the half life. GNRH this hormone is 10 amino acids long andhas a half life of 7 minutes in the blood stream FSH- this hormone is 540 amino acids and hasa half life of 2.5 hours |
|
|
epinephrine can be broken down locally and released into the bloodstream by? |
Monoamine oxidase in the blood stream. (MAO) |
|
|
MAO inhibitors prevent the breakdown of the monoamines in the blood stream. Why do we need them ? |
b/c all of the monoamines are feel good hormones. Their function is to increase the level of monoamines in the blood stream to prevent the sensation of depression |
|
|
Norepinephrine is released at synapse, has local effects and is broken down by ? |
COMT (catechol-o-methyl transferase |
|
|
For small molecules , one pass through the liver will alter the molecule by what percent??? |
70% |
|
|
Are protein hormones hydrophillic or hydrophobic |
hydrophiilic |
|
|
protein hormones are hydrophilic therefore they bind to receptors where? Do they pass through the cell membrane |
they bind to the receptors in the cell membrane to create or cause their effect. they don't pass through the cell membrane because they're water soluble and can't pass through the lipid tails |
|
|
the mechanism of action requires a protein receptor on the cell ____- |
surface peripheral cell proteins are on the inside of the cell surface not the outside of the cell surface |
|
|
lipid explain the mechanism of action of the lipid hormone/steroid hormone |
Steroidhormones travel through the cell membrane by binding to the steroid horomonereceptor complex. The steroid hormone receptor complex goes into the nucleus tobind to a segment of the dna called a HRE Hormone Response Element.. HRE thenactivates transcription and translation within that cell i. They are soluble in fats (hydrophobic), thus, theycan travel through the cell membrane. Onceinside the cell they can bind to their target receptor.ii. Transport through the membrane is made possiblesecondary to the cholesterol in the membrane which separates the phospholipidmolecules. The membrane cholesterolmakes up 13% of the total membrane mass and increases fluidity of the cellmembrane and solubility/easier transport for lipid like molecules |
|
|
what has a long half life secondary to the sugar attached which make them more difficult to break down? |
glycoproteins |
|
|
Definition: These hormones are made up of amino acids that are bound to a peptide chain one at a time, beginning from the amino terminal to the carboxyl end |
Proteinaceous Hormones |
|
|
definition: The pre-signal peptide is cleaved in the RER. This molecule has the signal peptide still attached (once we've cleaved off the signal peptide the _________ is now the prohormone_ |
Pre-prohormone |
|
|
Definition: The inactive hormone is further modified somewhere around the golgi apparatus |
prohormone |
|
|
Definition: This hormone will be released via exocytosis. Not 100% of the pre-pro hormones become these type of hormones |
Active hormones |
|
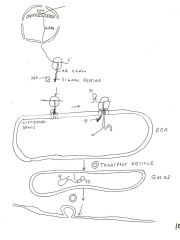
Explain the 9 steps of protein synthesis |
1. mRNA synthesized in the nucleus via transcription 2. mRNA travels out through the nuclear pores into the cytoplasm and binds to a ribosome 3. Peptide chain elongation by peptide bond formation until a stop codon is reached. The codon will be paired with itsanti-codon. This results secondary to aminoacyl tRNA synthase.New amino acids will be bound to the growing amino acid chain via peptidyl transferase. 4.The signal peptide within the cytoplasm binds to the signal recognition particle (SRP) on the amino terminal of the growing peptide molecule. 5. The SRP will only facilitate guiding the protein to the endoplasmic reticulum where it will bind to a receptor/channel on the Rough ER called a translocon. Thus,the developing protein into the RER. Here is where we have the pro-hormone 6. The protein continues to get longer until we reach a chain terminating sequence. The protein can serve many different functions at this point. Let’s consider the product another hormone. 7. The molecule with its signal peptide still attached is a pre-cursor hormone --> pre-prohormone. Eventually the signal peptide can be cleaved with signal peptidase --> now we have a prohormone. The prohormone will now be bud off into a transport vesicle and head to the Golgi apparatus. Enzymes present in the vesicles will continue to digest the molecule into an active hormone. 8.In the Golgi, N-glycosylation and disulfide bond formation will occur. 9.Hormones are packaged by the Golgi apparatus into secretary vesicles in their active form to be exocytosed from the cell |
|
|
Insulin is a great example- entire structure of a prohormone looks like the proinsulin, then when they cleave off the C peptide the insulin is left. Insulin is the active hormone. Proinsulin is the inactive hormone. |

|
|
|
Two properties of steroids.
1. absorbed through the ____ Hard on the _____ |
absorbed through the gut hard on the liver |
|
|
What are the oral anabolic steroids vs. injectable steroids impact on liver function |
Oral anabolic: hard on the liver. Will travel through liver quickly because they’re absorbed through the gut. Broken down in a faster rate. Hard on liver/less efficacy or activity
Injectable steroids: not as hard on liver/last longer in the blood stream. |
|
|
all steroid hormones are derived from _____ |
cholesterol |
|
|
Which carbon does most enzyme activity occur on cholesterol? |
Carbon 17 |
|
|
Explain steroid hormone synthesis |
a. Synthesis in the smooth endoplasmic reticulum Composed from cholesterol Travels in the blood via apo lipil proteins (Apolipil protein which carries cholesterol esters, triacylglycerides) b. Cell membrane receptors for HDL’s and LDL’s c. Pregnenolone synthesis from cholesterol d.Pregnenolone converted to progesterone within the smooth endoplasmic reticulum e. Note the way we refer to the carbons in the pregnenolone molecule |
|
|
Explain the steroid pathway |
1. LDL molecule binds to the LDL receptor located on the outer membrane of the cell. Binding causes the entire complex to be endocytosed into the cell. 2. The endocytosed complex will bind with the lysosome inside the cell and be digested into its respective parts (apolipoproteins, cholesterol, and protein) 3. LDL receptors are reused/reconstituted/ and re-expressed on the cell surface 4. Apolipoproteins are broken down into simple amino acids and used however the body sees fit 5. The fatty acids and cholesterol will be further processed by the mitochondria. Cholesterol will be exposed to the enzyme cholesterol desmolase which will cleave the side chain. Side chain removal will cause its transformation into pregnenolone. 6. Pregnenolone will travel from the mitochondria,to the smooth ER into the Golgi. The golgi will convert pregnenolone into progesterone. And then it will be exocytosed outside of the cell |
|
|
protein hormones go through the _____ ______ and steroid hormones go through the ________ (hint: parts of the cell) |
Protein hormones go through the Endoplasmic Reticulum Steroid hormones go through the mitochondria (remember this b/c it is the power house of the cell) |
|
|
would women or men see more significant gains if they take anabolic steroids? |
women because they are more sensitive to testosterone. |
|
|
what are the irreversible changes women can have if they take anabolic steroids? |
body hair, clitoris enlargement |
|
|
What drug is used initially as an aromatase inhibitor for post menopausal women and breast cancer? |
arimidex |
|
|
what is another aromatase inhibitor besides arimidex? |
Femara |
|
|
Clomid is used in women fertility what does it do? |
Inhibits the estrogen receptors in the hypothalamus. Which increases FSH, serves as a fertility drug to increase the number of folliclesovulated to give the women a chance for a viable pregnancy |
|
|
What does clomid do to males that take anabolic steroids and have low testosterone levels?
|
Blocks estrogen receptors in the hypothalamus now the hypothalamus doesn’t see any estrogen so it allows the pathway to jumpstart the testosterone and make sperm again |
|
|
Do steroid and protein hormones travel through the cell membrane and bind to an intracellular receptor |
steroid |
|
|
Do protein hormones or steroid hormones bind to a cell membrane protein receptor? |
protein |
|
|
Protein hormones all bind to a cell membrane protein receptor with one exception which can travel through the cell membrane and bind to an intracellular receptor. what is it? |
thyroid hormone |
|
|
hormonal binding to the cell membrane will elicit one or more of the following actions: |
1. Activation of G proteins 2. Initiation of tyrosine kinase pathways 3. Open zion channels 4. Other unknown activities: meiosis,transcription, translation |
|
|
what is a specific enzyme that dephosphorylates a protein? |
phosphorylase |
|
|
Activation or deactivation of phosphorylase can be caused by either..... |
phosphorylation or dephosphorylation |
|
|
what is a family of enzymes that phosphorylates a protein by adding a phosphate? |
kinases |
|
|
What typically phosphorylates a protein by adding a phosphate? |
tyrosine kinase |
|
|
what typically phosphrylates serin/theronine amino acids in the protein chain |
serine/threonine kinase |
|
|
what is A protein composed of three subunits that break apart when activated to initiate reactions within the cell |
G- protein |
|
|
What are the three types of G-proteins and what do they do? |
-Gs-protein: Stimulatory which activated the cAMP/PKA system -Gi-protein: Inhibitory which inhibits the cAMP/PKA system -Gy- protein-activates the PKC system (protein kinase C pathway) |
|
|
explain the protein hormone synthesis pathway (stimulatory pathway) |
1. Catecholamine binds to a beta-adrenergic receptor and initiates a down stream pathway 2. Release of GDP from the attached α-subunit (when hormone binds the alpha subunit loses its affinity for GDP) GDP comes off so… 3. Binding of GTP and release of α-subunit from G-protein (this is the step the G protein is now active, GTP leaves with the alpha subunit in tact) 4. Inactive adenylate cyclase makes active adenylate cyclase 5. Adenylate cyclase converts ATP into cCAMP (A 2ndmessenger) 6. cAMP will be broken down into 5’AMP byphosphodiesterase (PDE) 7. Inactive PKA is converted to active PKA 8. Phosphorylation of serine/tyrosine residues to activate the enzyme glycogen phosphorlase. This enzyme will enable glycogen to be transformed into glucose, thus, allowing an increase in blood glucose. |
|
|
The guanylate cyclase system is an enzyme-linked receptor system. cGMP will act as a second messenger initiating intracellular activity. The downstream pathway might result in phosphorylation/dephosphorylation of a protein. What is an example of guanylate cyclase system? |
activation of nitric oxide within arterioles |
|
|
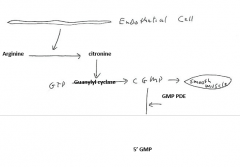
Explain the nitric oxide pathway |
This processis initiated when endothelial cells which line the inside of the vascularsystem are exposed to stress. Stress can result from tension and/or shearing of the endothelial layer. 1. Endothelial stress/shearing release of eNOS(endothelial nitric oxide synthase) 2. Enos converts Arginine or citrulline NO(nitric oxide) which is made at the endothelial cell. Will have its effect onthe muscle cell wall of the vessels 3. Activation of Guanylyl cyclase 4. GTP cGMP 5. cGMP is a 2nd messenger, thus, acascade of results will follow ( GMP-PDE could convert CGMP to 5’ GMP) a. Smooth muscle dilation ( to take the stress offof the endothelial cells) b. Hypotension c. Decreased stress on the cell |
|
|
What will nitric oxide supplementation do |
increase blood flow to the muscles, increased exchange of nutrients and wastes and alsohas potential positive cardiovascular effects by decreasing blood pressure. |
|
|
Artherosclerosis is the deposition of fat. it is a hardening of the arteries. Will we see an increase or decrease in blood pressure and blood volume |
increase |
|
|
there are two kinds of plaque that causes heart attacks. What are they? |
hard- from calcium depositions, stable plaques, long standing soft- of more concern than hard plaques, unstable, typically leads to an MI |
|
|
What are macrophages that gobble up cholesterol and gest so full they look like soapy suds. It spews this like a volcano and binds to clotting factors. Leads to most MI's |
foam cell |
|
|
A heart muscle is the only muscle that is aerobic. 75% of people that have a heart attack and survive will have muscle tissue damage. How do you fix that? |
beta blockers causes vasodilation of the blood vessels. Slows down heart rate, slows down force ofcontractions, gives the heart a little chance to rest. |
|
|
Cardiovascular disease andsupplementation with beta blockers and Ca++ channel blockers. Any hypoxic tissue will secrete ________ which will resultin increased vascular tissue which may increase cardiac function demand. The effects of angiogenin won’t be observedin tissue that has died. |
angiogenin
|
|
|
What is a major player involved in maintaining both a resting membrane potential and skeletal muscle contraction? |
Calcium |
|
|
Explain the IP3 Pathway |
1. Hormone will bind to the receptor protein 2. The G-protein binding will cause a confirmation change, thus, the GDP will disassociate from the α subunit followed by GTP binding to the α subunit initiating a confirmation change. Next the α subunit-GTP complex will disassociate from the G-protein. 3. The α subunit-GTP complex will bind with phospholipase C (PLC) 4. Activation of PLC will cause phosphotidyl inositol biphosphate (PIP2) to split into 2 molecules (IP3 andDAG). PIP2 is part of the plasmamembrane. ***NOTE*** IP3 and Ca++interact with different Ca++ ion channels via different mechanisms 5. IP3 will travel to the sarcoplasmic reticulum(SR) and bind to a IP3 receptor on the Ca++ channel in the phospholipidbilayer. Binding to the receptor willcause an efflux of Ca++ from inside the SR into the cytoplasm outside the SR. Efflux will have three different fates 1. Ca++ may bind to calmodulin (has 4 binding sites) to initiate smooth musclecontraction. a. Contraction may result in cardiac (Nernstpotential is ~ -90mV) or smooth muscle (Nernst potential ~ - mV). Thus, there is more electrical potential found outside cardiac muscle vs smooth muscle. Ca++ blockers will have more of an affect on cardiac when compared to smooth muscles resulting from the difference in electrical potential. 2. Ca++ may bind to a Ca++ regulated ion gate on the SR, thus, allowing a greater efflux of Ca++ to enter the cytoplasm from inside the SR 3. Ca++ may also bind to the Ca++ ion channellocated on the cells outer membrane. The binding here will allow Ca++ to enter the cytoplasm from outside the cell wherethe [Ca++] is at its greatest. 4. Diacyl glycerol (DAG) a. DAGwill activate protein kinase C (PKC). This Ca++ dependent. If we don’t have Ca++ available in the cytoplasm this isn’t a good pathway. b. PKC will allow for phosphorylation of serine and threonine residues, thus, allowing for possible gene transcription/translation c. Arachidonic acid is created which can make prostaglandins |
|
|
Albumins are responsible for _____ or ____ pressure |
oncotic or osmotic pressure |
|
|
what acts as clotting factors? |
fibrins |
|
|
What is the most commonly prescribed anti-clotting medicaiton post MI event? |
plavix |
|
|
_______ proteins carry various molecules in the blood. For example a steroid molecules can be carried in the blood once bound to a globular hydrophilic molecule. The hydrophobic protein carries the hydrophobic steroid. |
globular |
|
|
many globular proteins are specific to specific hormones while others are not. examples are? |
sex hormone: sex hormone/steroid binding globulin corticosteroid: corticosteroid binding globulin thyroid: thyroid hormone binding globuliin/tranthiertan steroid: steroid binding globulin |
|
|
a small proportion of proteins travel through the blood unbound. what is an example? |
hydrophobic aldosterone 40% travels bound to globular proteins 60% Travelsfree |
|
|
What are three different types of carrier proteins? |
non specific- Carry many different types of hormones. Protein carrier molecules found in high concentration in the blood, therefore, carrie sa significant percentage of hormones within the blood
specific: Has binding sites for specific hormones and will carry the hormone through the blood unbound: A small amount of hormone types are carried through the blood unbound |
|
|
Explain hormone movement into the target cell |
a. Binding proteins release the hormone at the target cell and the steroid diffuses into the target cells cytoplasm b. Receptors are located within the nucleus orcytoplasm of the target cell c. Binding is to specific receptors d. Steroid hormone receptors belong to a super family of nuclear and DNA binding proteins that act as transcriptionfactors that are only active in the receptor protein/steroid hormone state. |
|
|
Explain hormone activation of a receptor |
a. Hormone enters the cytoplasm possibly via diffusion and the hormone will bind to a nuclear receptor. The hormone/receptor complex will bind to the Hormone Response Element (HRE) and initiation of transcription will take place. i. Specific Hormone Response Elements (1) ERE- Estrogen response elements (2) ARE- Androgen response elements |
|
|
what is the master gland of the master gland- directly control release of hormones from the anterior pituitary (master gland). |
hypothalamus |
|
|
The hypothalamus is located where? |
below the thalamus and is an extension of the brainstem. Hypothalamic tissue surrounds the 3rd ventricle and it creates a bowl in which the 3rd ventricle sits in which is filled with CSF. (CSF will provide feedback to nucleus) |
|
|
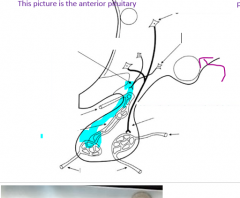
The hypothalamus contains a large quantity of nerve cell bodies called _____ which are int he walls of the hypothalamus and have _____ ______ which travel to either the ____ ____ and terminate (release neurosecretions. The ___ ______ have axons which travel down and release their secretions into the ____ _____ artery located at the posterior pituitary proper |
The hypothalamus contains a large quantityof nerve cell bodies called nuclei. The nuclei are in the walls of the hypothalamus and have short axons which travel to either the median eminence and terminate (release neurosecretions). The long nuclei have axons which travel down and release their secretions into theinferior hypophyseal artery located at theposterior pituitary proper. |
|
|
The median eminence is a highly vascularized structure and comprises what? |
the floor of the 3rd ventricle and the base of the infundibulum |
|
label this |
|
|
|
The superior and inferior hypophyseal arteries both receive blood from the ____ ______ ____- |
middle cerebral artery
|
|
|
What is the most common vessel involved in a stroke? What are the two most commonly affected regions? |
middle cerebral artery pre-central gyrus and post-central gyrus are the 2 most commonly affected regions |
|
|
A stroke could result in necrosis to the ___ ____ which would result in hormone disturbances |
Pituitary region |
|
|
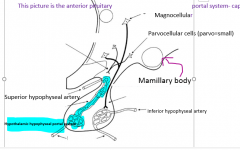
hypothalamic hypophyseal portal system travels from the ____ ______ to the ____ ______ ____ |
hypothalamic hypophyseal portal systems travels from the median eminence to the anterior pituitary gland, |
|
|
What is a hormone that is bound to another molecule,which comes from the hypothalamus and is released from either the anterior orposterior pituitary gland. The bound complex will travel down the axon together. As they are released into the blood stream the complex will breakapart. There is currently no known function of the binding molecule once it separates from the active hormone in the bloodstream. |
Neurophysins |
|
|
1. Hypothalamic neurons synthesize and secrete neurohormones or _______ |
neurosecretions |
|
|
Hypothalamic-hypophyseal system contains the |
a. Posterior pituitary- contain magnocellular cells i. Contain 2 main nuclei that contain magnocellular cells (large cells with long, vericose axons Supra optic nucleus Paraventriculear nucleus b. Anterior pituitary – i. Main nuclei arise from the parvocellular cells in the hypothalamus. |
|
|
list the Hypothalamus hormones: (if you see RH or IH you know it is from the hypothalamus |
TRH- Thyrotropin Releasing Hormone GnRH- GonadotropinRelease Hormone GHRIH- -Growth hormone releasing inhibiting hormone GHRH- GrowthHormone Releasing Hormone CRH-CorticotropinReleasing Hormone PRIH- ProlactinReleasing Hormone ( |
|
|
What are the functions of TRH- Thyrotropin Releasing Hormone |
stimulate synthesis and release of TSH Stimulates the release of prolactin |
|
|
What are the initiating factors of TRH- Thyrotropin Releasing Hormone |
i. Release when exposed to cold environments --> TRH stimulation --> TSH -->increased metabolism --> increased metabolic rate through the downstream pathway of the thyroidsystem ii. Release in response to a decrease in circulating thyroid hormone |
|
|
i. TRH is important in the proper _____ function |
cerebellum |
|
|
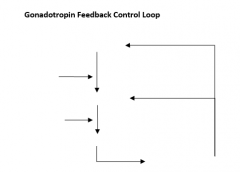
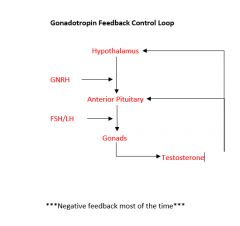
GnRH Gonadotropin release hormone function: |
Relase of FSH and LH from the anterior pituitary gland |
|
|
GnRH Gonadotropin release initiating factors: |
Low levels of circulating estrogen, testosterone and progestins Low frequency pulses of GNRH will cause FSH release: LH produces testosterone FSH- produces sperm |
|
|
Exogenous testosterone use will inhibit the hypothalamic-hypophyseal-gonadal axis (HHG). High levels of testosterone will cause a decrease in____, decrease in production of ____ and decrease of production in ____ |
decreasein GnRH, decrease in production of sperm and decrease of production in testosterone. |
|
|
What does GHRIH (AKA: GHIH- Growth hormone releasing inhibiting hormone) doin the thyroid. |
i. decrease release in calcitonin (tones down blood calcium). A decreased release results in Ca2+ removal from bones into the blood thus a decrease in bone density is seen. ( will be excreted by the kidneys) |
|
|
What does GHRIH (AKA: GHIH- Growth hormone releasing inhibiting hormone) do in the pancreas. |
(1) Inhibits insulin and glucagon production Glucagon’s job is to put sugar in the blood, insulin pulls sugar from the blood and puts it in the cell. Samatostatin inhibits both processes |
|
|
What does GHRIH(AKA: GHIH- Growth hormone releasing inhibiting hormone) do in the pituitary. |
(1) Inhibits growth hormone from the pituitary gland. Will inhibit at the anterior pituitary. It also inhibits the production of TSH from the anterior pituitary gland. |
|
|
What does GHRIH (AKA: GHIH- Growth hormone releasing inhibiting hormone) do in the Gi |
(1) Contributes to the balance observed between production/non-production of enzymes for digestion, which enables energy to be conserved. (2) Inhibits secretions of all glands within the digestive system. Lumones is a generalized term for a hormone that will have aneffect on the GI system. (3) You spend upwards of 40% of your metabolic requirements dealing with digestion on an average day |
|
|
What does GHRIH(AKA: GHIH- Growth hormone releasing inhibiting hormone) do in the Brain |
(1) It has a generalized sedative effect on the body which contributes to drowsiness |
|
|
What are the only true anabolic hormones?
|
insulin igf (insulin growth factor) hgh (human growth hormone thyroid hormone testosterone |
|
|
What are the two main growth inhibiting hormones |
somatostatin and corticosteroids |
|
|
GHRH Growth Hormone Releasing Hormone function is
|
Stimulates GH production in the anterior pituitary gland |
|
|
CRH - Corticotropin Releasing Hormone is formed/produced in the ? |
placenta Crh production increases within the placenta as the baby becomes stressed. Causes an increase in the cortisol production within the baby. That is the initiating factor to cause oxytocin levels to increase. |
|
|
If a female in labor has pre-term labor contractions (Braxton Hickscontractions) or bleeding (placenta abruptio- the placenta has torn away from the endometrium) Treatment of choice is ________and probably bedrest. since it inhibits uterine contractions |
Progesterone |
|
|
PRIH –Prolactin Releasing Hormone is also called |
dopamine
|
|
|
PRIH - functions to |
inhibit prolactin release |
|
|
opiates are also called |
endorphins/enkephalins |
|
|
Formation of opiates- all of the following are cleaved off of POMC: these are neurohormones with endogenous analgesic effects. Called the Natural Opiates i.e endurance exercise will cause a surge of endorphins |
Endorphin and met-enkephalins, |
|
|
Formation of opiates- all of the following are cleaved off of POMC: ____ _____ ____ binding to receptors can lead to hyperpigmentation secondary to stimulation ofmelanocytes which will cause the skin to darken. This is a very common side effect observed inAddison’s disease |
Long term ACTH |
|
|
Opiates function: |
i. See an increase in GH and PRL (prolactin) release. ii. In the brain the opiates have a synergistic affect by stimulating the release of epinephrine. Recall epinephrine is one of the feel good hormones. iii. Hypothalamus: decrease in GnRH release is observed which will also lead to a decrease in LH/FSH. Long term elevation of opioids can lead to amenoria(sp?) in females. |
|
|
3 factors contribute to infertility in active women. |
1. Increased production of opioids 2. A decrease in fertility in women 3. Decrease in body fat |
|
|
- Why does a decreasein body fat cause problem with decrease in menstruation? |
Body fat is loaded with aromatase. Increase in body fat= increase in aromatase activity. Decrease in body fat decreases aromatase which converts testosterone into estrogen. If there is no estrogen women have problems with menstruation. If a woman decreases body fat that will cause a decrease in menstruation which will lead to a decrease in bone density. Estrogen is required to maintain bone density. |
|
|
What is the problem with post-menopausal women being given hormone replacement therapy (increasing levels of estrogen) |
- caused increase in breast cancer because they were feeding this problem. We stopped doing HRT in females, but now guys are getting high levels of testosterone because they have low testosterone and they’re developing prostate cancer.
|
|
|
How do guys fix low testosterone? |
lose weight and body fat to increase testosterone naturally |
|
|
|
|
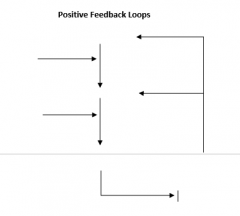
fill in blanks. Is this negative or positive feedback most of the time? |
|
|
|
|
|
|
What Arose from rathkes pouch during 1st trimester whichwas ectodermal invagination of the oral pharynx. 5 cells types, distinguished by size andshape of the secretory gland, staining characteristics and cell shape. |
Pituitary Gland |
|
|
What are the four types of things that arise from the anterior pituitary gland? |
Corticotrophs Gonadotrophs Thyroptrophs Somatotrophs |
|
|
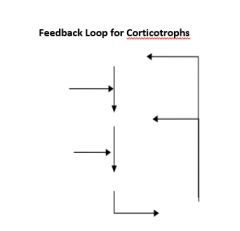
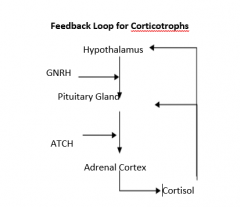
What is the corticotroph function? What does it release ? |
to stimulate the adrenal cortex. Releases ACTH- Adrenocorticotropin, Beta-Lipotropin and MSH |
|
|
Cortisol has a Negative or Positive feedback loop at they hypothalamus and the anterio pituitary gland on ACTH? |
Negative |
|
|
Increased levels of cortisol down-regulates or up-regulates ACTH? |
Down regulates |
|
|
What are the six stimuli for ACTH release? |
1. Anxiety 2. Pyrogens - increased fever 3. Hypoglycemia 4. Pain 5. Circadian rhythms (cortisol, menstruation etc) 6. physical stress |
|
|
Increased levels of stress can lead to a condition known as what? |
Crooks Hyaline Change/Cushings Syndrome |
|
|
High levels of stress can do damage in three ways. what are they? |
1. increase release of sugars into the blood stream causing endothelial damage 2. coronary artery vasospasm 3. increase in blood pressure |
|
|
What do gonadotrophs secrete? |
gonadotropins: LH (Leutinizing hormone) and FSH (Follicle stimulating hormone) |
|
|
What tells the body to release LH/FSH? |
GNRH |
|
|
LH and FSH are produced in _____ ______: once every hour which may be different between males and females
|
episodic bursts |
|
|
GnRH comes from the _________ (where in the brain) |
hypothalamus |
|
|
In males Inhibin is secreted from the ________ cells which are located in the tubule in the seasmen vesicle |
sustentacular |
|
|
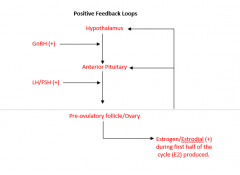
Estradiol (estrogen) confers a negative feedbackresponse most of the time in females. However, during the ________surge there is a huge positive increase inestrogen which greatly increases in GnRH |
Ovulatory stage GnRH,estrogen-->follicular cells -->increased GnRH -->increased FSH/LH -->increased estrogen |
|
|
What female cells produce inhibin on the female side? |
granulosa cells |
|
|
What inhibits production of sperm and tells FSH to shut down bypassing GNRH? |
Inhibin |
|
|
What secretion will increase the production of FSH? |
Activin |
|
|
What is the function of FSH in males? |
A. Stimulate the development and MATURATION OF SPERM B. Involved in the production (STIMULATION) of ANDROGEN BINDING PROTEIN which helps keeps testosterone in the testes for proper sperm development. |
|
|
What is the function of FSH in females? |
A. Stimulates OVARIAN FOLLICULAR GROWTH AND DEVELOPMENT. B. Stimulates ESTROGEN SYNTHESIS synthesis and release from the follicular cells |
|
|
What is the function of LH in males |
A. Responsible for SECONDARY SEX CHARACTERISTICS (ANDROGENIC: FACIAL HAIR, ACNE, HAIR LOSS – ANABOLIC: MUSCLE GROWTH) B. Responsible for most of the PRODUCTION OF TESTOSTERONE |
|
|
What is the function of LH in females |
A. Stimulates the CORPUS LUDEUM FORMATION B. Stimulates maturation of the ovum for OVULATION. Note:There is an LH surge 12-24 hours prior to ovulation, thus, it is called the ovulation hormone. |
|
|
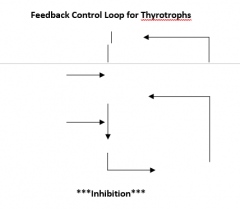
What hormone do thyrotrphs produce? |
TSH |
|
|
Thyrotroph cells will ______. The receptors on the cell will require an antibodyto bind to it
|
immunostatin |
|
|
What is the main function of TSH |
the synthesis and release of thyroid hormone stimulation |
|
|
TSH has increased synthesis of _________ Increased ____ transport into the follicular cells of the thyorid gland Increased ____ of thyroglobulin Increased exocytosis to ____ and ____ |
TSH has increased synthesis of thyroglobulin Increased iodide transport into the follicular cells of the thyorid gland Increased endocytosis of thyroglobulin Increased exocytosis to T3 and T4 |
|
|
What is the precurser to the thyroid hormone? |
thyroglobulin |
|
|
What produces the growth hormone? |
Somatotrophs |
|
|
What hormone is regulated by GHRH from the hypothalamus? |
Growth hormone |
|
|
GRGH is increased by what? |
GHIH |
|
|
What stimulates GHRH |
process of fasting exercise- weight training increase in protein in the diet physical stress increase in carbohydrate consumption |
|
|
Explain what happens when GH acts on the liver |
There are many GH receptors on the liver. The liver will produce Insulin like growth factors/IGF’s in response to high HGH - When GH binds to the receptors. IGF’s will stimulate bone growth, muscle growth,increase amino acid uptake and will exert a negative feedback on GNRH and GH production |
|
|
Serum [HGH] is pulsatile and hard to measure,thus, it is more common to see clinician’s measure _________ |
somatomedians (AKA: IGF’s). (IGF’s are in higher concentrations in the bloodstream, maintain a more regular release and have a longer half-life when compared to serum [HGH].) |
|
|
Dwarfism results from a ____ deficiency |
GH |
|
|
What congenital dwarfism will the patient have a lack of GH receptors, but will produce the proper amount of GM? Also the most common form of dwarfism. |
Laron's Dwarfism |
|
|
What congenital dwarfism will have a normal GH, but an inappropriate rise in IGF. This may result from a problem with GH receptors on the liver |
African Pigmy |
|
|
What type of congenital dwarfism stems from a gene deletion |
Hereditary |
|
|
What are the two ways to acquire dwarfism |
1. pituitary tumors which will squeeze out the somatotrophs 2. pituitary infection (a potential mechanism for this to happen is a sinus infection that could destroy the pituitary gland) |
|
|
What is the treatment for dwarfism |
using recombinant HGh |
|
|
What is a problem with supplementing with HGH |
HGH is species specific, thus,supplementation with GH from another species there would be very little response. Original treatment consisted of HGH harvesting from 120 cadavers over the course of a year to provide enough HGH to make a difference. The biggest side effect resulted from prion disease which resulted in death. |
|
|
What type of disease has an increase in GH prior to epiphyseal plate closure. Rapid growth with early epiphyseal plate fusion and occurs before epiphyseal plate fusion |
giantism |
|
|
What are the signs and symptoms for giantism? |
(1) Increase in skin thickness with (dermis and epidermis), deepening of the voice secondary to increasing length in vocal folds, overgrown skeleton, barrel chest, and many cardiovascular complications (because of an increase in glucose and fats in the blood) |
|
|
What is the treatment for Giantism? |
surgery, radiation, hormonal therapy |
|
|
What disease has an increase in GH production after the epiphyseal plate fusion. This can occur when the tumor develops after epiphyseal plate closure |
Acromegaly |
|
|
What are the signs and symptoms for Acromegaly?
|
(1) Increase in skin thickness with (dermis and epidermis), deepening of the voice secondary to increasing length in vocalfolds, overgrown skeleton (long bone diameter increases), barrel chest,increase in muscularity, teeth are separated or lacking, size of tongue can increase, and many cardiovascular problems |
|
|
What is the treatment for Acromegaly? |
Surgery, radiation, hormone therapy |
|
|
What pituitary is the Arterial blood supply provided by the inferior hypophyseal artery. Hormones of the________ pituitary gland are produced in magnocellular cells of the hypothalamusand travel down the axon via axoplamic flow to the axon terminals located inthe median eminence. |
posterior pituitary posterior |
|
|
What are the hormones of the posterior pituitary? |
oxytocin (hint to remember: company OP- oxytocin goes with posterior pituitary) anti-diuretic hormone (ADH) |
|
|
Oxytocin is synthesized in the cells of the _______ nuclei in the hypothalamus |
paraventricular |
|
|
What is the function of Oxytocin? |
Involved in the milk let-down reflex- myoepithelial cells of the mammary gland Will contract uterine contractions- contraction of the myometrium of the uterus |
|
|
Which hormone is aka: vasopressin and is synthesised in the supraoptic nuclei of the hypthalamus? |
Anti-diuretic hormone- ADH |
|
|
What is the funciton of ADH |
Retain fluids vasoconstriction the blood vessels ie: raise blood pressure *** main function |
|
|
Both oxytocin and ADH are synthesised within the rough ER of the magnocellular cells of the hypothalamus. They are packed into secretory granules that migrate down the axon bound to neyrophysisns (pressophysin) from ADH and oxyphysin for oxytocin. ADH also has glycoproteins which are bound. Here the hormones are cleaved into their active form and stored for release when needed. There is no known function for either the neurophysins or the glycoprotein once released into the blood stream |
Both oxytocin and ADH are synthesised within the rough ER of the magnocellular cells of the hypothalamus. They are packed into secretory granules that migrate down the axon bound to _________ (pressophysin) from ADH and ______ for oxytocin. ADH also has glycoproteins which are bound. Here the hormones are cleaved into their active form and stored for release when needed. There is no known function for either the ____ or the _____ once released into the blood stream |
|
|
What is the half life of ADH? |
15-20 minutes |
|
|
ADH function includes osmoregulation. explain this |
Osmoreceptors (vasculosum osmoreceptors) which line the 3rd ventricle. These magnocellular cells sense changes in the osmolality of the extracellular fluid (Na+ content).
In the walls of third ventricle there are osmoreceptors known as the organum vasculosin, these cells monitor the osmolarity of the fluid in the third ventricle. Osmolarity increases in the third ventricle stimulating these osmoreceptors. They project their information to the neurons to cause the superoptic nuclei to release or produce of antidiuretic hormone |
|
|
ADH function is baroregulation. explain this |
a. Changes blood pressure, decrease in BP, lead to an increase in ADH production to conserve water and increase blood pressure.
|
|
|
What stimulates ADH production? |
nausea and vomiting |
|
|
What inhibits ADH production |
Alcohol,caffeine, nicotine will inhibit the release of ADH |
|
|
What will cause devastating effects on the renal system? |
Malignant hypertension If blood flow in kidneys is decreased you’re not clearingout the amount of urine you should be clearing which leads to high bloodpressure |
|
|
Adecreased production of ADH or a decrease in the sensitivity of ADH receptors within the kidneys will result in a tremendous loss of water. Patients can lose up to 25L of fluid per day. This leads to a significant increase of fluid loss. What disease results in this? |
diabetes insipidus |
|
|
What is the nephrogenic cause of diabetes insipidus? What is the Neurogenic cause? |
nephrogenic- receptor stops working normally neurogenic: decrease production of ADH |
|
|
What syndrome most commonly results from a lung tumor(could also be from trauma) which will cause a large amount of ADH productionSeen most commonly with small cell carcinoma and mesyltheliomas. Can cause death. One symptom is cerebral edema and myoclonus(muscle spasms) |
Syndrome of inappropriate ADH production (SIADH) |
|
|
What is the half life of Oxytocin? |
3-5 minutes and then it is degraded by the liver |
|
|
Oxytocin is responsible for the milk let down reflex. Explain |
Afferent neurons in the nipples and the areolasynapse on the magnocellular cells of the paraventricular nucleus causing depolarization and the release of the synaptic granules containing oxytocin. |
|
|
Oxytocin is responsible for the uterine contraction and cervical distention during labor and parturition. Explain |
a. This is a positive feedback mechanism. This process is multi-hormonal. Stretching of the cervix and the myometrium releases oxytocin in normal labor. Once cortisol release from the placenta and/or the baby and an increase in [serum] will initiate this process. The uterine contractions stimulate afferent neurons in the wall of the uterus --> causing the release of oxytocin -->causing the myometrium to contract even more. |
|
|
What drug can be given to kick start or jump start labor after a stalled labor? |
pitocin
|
|
|
What are the actions of oxytocin (supposedly won't be on the test.. but you never know) |
lactation parturition increase in release of sperm into seminal fluid sperm movement corpusluteum |
|
|
What causes decrease in function, pituitary tumors, hypothalamic tumors, infarction, vascular malformation secondary to a genetic condition. |
Hypopituitarism |
|
|
Hypopituitarism: What condition results from a complete loss of function from the anterior pituitary gland. Females will have amenhorrhea and males will have impotence. Both will also observe dysfunction in the other anterior pituitary hormones ie: no FSH/LH or TSH production. This condition may result in lethargy, stupor, and even death. |
Panhypopituitarism |
|
|
What is the treatment for panhypopituitarism? |
replace hormones that are no longer being made. Most important is ACTH, Cortisol is prescribed |
|
|
Hypopituitarism: What condition typically occurs at the hypothalamic pituitary axis. There is a loss of GnRH, thus, in females: amenorrhea, males, a decrease in secondary sex characteristics |
Isolated Gonadotropin deficiency |
|
|
What is the treatment for Isolated gonadotropin deficiency? |
GNRH supplementation |
|
|
Hypopituitarism:What condition is relatively uncommon, but the most common cause is Prednisone Use |
ACTH deficiency |
|
|
Hypopituitarism:What condition is observed secondary to post partum anterior pituitary necrosis. it is not uncommon to see a huge increase in the number of lactotrophs during pregnancy. This increase may create an environment in the anterior pituitary which is highly susceptible to injury. *** TEST QUESTION |
Sheehan's disease |
|
|
What type of diseases typically arise from tumors and precocious puberty (tumors arise form gonadotrophs) |
Hyperpituitarism |
|
|
Hyperpituitarism: What is an ACTH secreting tumor. You will observe an increase in metabolism, redistribution of fat to the face (moonface) and to the back (buffalo hump) hyperpigmentation resulting from an increase in MSH production and possibly diabetes. ***** Know for test |
Cushings Disease |
|
|
Hyperpituitarism: What is the most common of all the pituitary tumors? It is 5x more common in females vs. males. Men will lactate if they have it. Hormonal abnormality with a loss of vision |
prolactin secreting tumor |
|
|
What 4 different target organs does the Growth hormone affect? |
Liver, bone, muscle, adipose tissue |
|
|
What will inhibit the GH Feedback mechanism? |
GHIH or somatostatin |
|
|
What is the most common cause of pituitary tumors? |
Lactotrophs |
|
|
What inhibits lactotrophs? |
secretion of dopamine |
|
|
What inhibits lactation? |
progesterone |
|
|
What will cause an increase production of milk glands during pregnancy? |
prolactin
|
|
|
GH in pre-pubescent individuals will cause an increase in the cell size of bones and muscle AFTER or BEFORE epiphyseal plate fusion? |
after |