Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
23 Cards in this Set
- Front
- Back
|
Embryonic precursor of superior parathyroid gland.
|
4th and 5th pharyngeal pouch
|
|
|
Embryonic precursor of inferior parathyroid gland.
|
3rd pharyngeal pouch
|
|
|
What structures do 4th and 5th pharyneal pouch develop into?
|
superior parathyroid gland
thyroid C cells (parafollicular) |
|
|
What structures do 3rd pharyngeal pouch develop into?
|
inferior parathyroid gland
thymus |
|
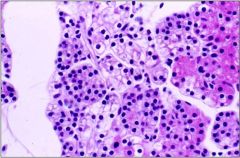
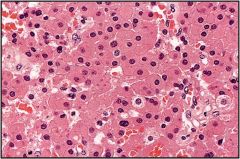
What type of parathyroid cells do you see in this image?
|
- chief cells: basophilic, look clear if more glycogen, screte PTH
- oxyphil cells: many mitochondria, do not secrete PTH - fat |
|
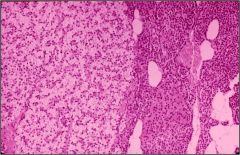
Is this parathyroid section from a young or an old adult?
|
young adult
- 50-90% cells - rest is fat |
|
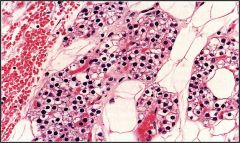
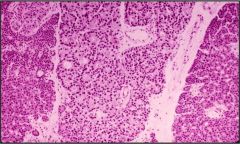
Is this parathyroid section from a young or an old adult?
|
old adult
- 30-60% cells - oxyphil cell nodule |
|
|
What are some symptoms of hyperparathyroidism?
|
- groans (GI)
- bones (resorption) - stones (urinary) - moans (psychic) |
|
|
Primary vs. secondary vs. tertiary hyperparathyroidism?
- high PTH - high/normal Ca2+ |
primary hyperparathyroidism
- one or more parathyroid gland secrete excess PTH which leads to hypercalcemia |
|
|
Primary vs. secondary vs. tertiary hyperparathyroidism?
- high PTH - low/normal Ca2+ |
secondary hyperparathyroidism
- conditions that chronically lowering serum Ca2+ (hypercalciuria) -> high PTH |
|
|
Primary vs. secondary vs. tertiary hyperparathyroidism?
- high PTH - high/normal Ca2+ - previousely had secondary hyperparathyroidism |
tertiary hyperparathyroidism
- autonomous PTH secretion develops after secondary hyperparathyroidism |
|
|
What are some common causes of primary hyperparathyroidism?
|
- adenoma in one gland (75-85%)
- 4 gland hyperplasia (10-15%) - carcinoma (1-3%) - double adenoma: rare |
|
|
What is the most common cause of primary hyperparathyroidism?
|
adenoma in one gland
|
|
|
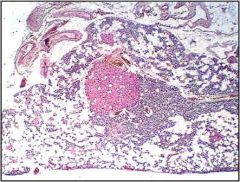
What is this parathyroid disease?
gross - 1 gland > 1cm, 300mg - encapsulated, red-brown - compressed normal yellow-tan parathyroid Lab - high PTH - high Ca2+ - may be hemorrhagic or cystic |
adenoma
|
|
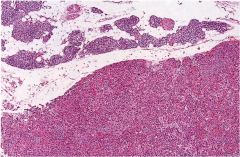
What is this parathyroid disease?
|
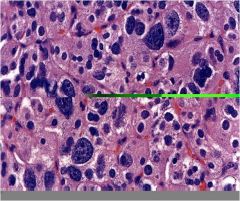
parathyroid adenoma
- sheets of cells - no intracellular or stromal fat - atypical nuclei - compressed normal gland |
|
What is this parathyroid disease?
|
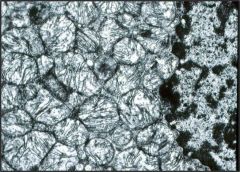
oxyphilic cell adenoma - a variant of parathyroid adenoma
- large cells - cytoplasm packed with mitochondria |
|
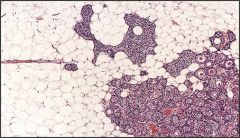
What is this parathryroid disease?
|
lipoadenoma- a variant of parathyroid adenoma
- solid nests of chief and oxyphil cells mixed with mature fat |
|
What is this parathyroid disease?
- all 4 glands greater than 55mg - all are hypercellular |
4 gland hyperplasia
- chief cell hyperplasia (including water clear cells) - solid and follicular patterns |
|
|
What is the tumor genetics of parathyroid carcinoma?
|
- loss of Rb tumor suppressor gene
- over-expression of cyclin D1 - reduced expression of CDK inhibitor P27 |
|
|
What is the most common cause of secondary hyperparathyroidism?
|
chronic renal failure
- reduced alpha1-hydroxylase activity -> less vitD -> low serum ca - reduced GFR -> phosphate retention -> increased serum phosphate -> decreased serum Ca - decreased serum Ca -> increased PTH with 4 gland hyperplasia -> increased bone resorption -> osteitis fibrosa cystica |
|
|
What is this condition?
- low serum Ca - low serum PTH |
hypoparathyroidism
|
|
|
What are some common causes of hypoparathyroidism?
|
- surgical removal during thyroidectomy
- congenital (diGeorge syndrome) - familial hypoparathyroidism: AIRE mutation (APS1) - idiopathic |
|
|
What is this condition?
- Chvostek sign - Trousseau sign - anxiety, depression, instability - cataracts, lens calcifications - QT prolongation |
- low ionized serum Ca -> neuromuscular irritability -> tetany
|