![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
234 Cards in this Set
- Front
- Back
|
Mechanisms of Hormonal Regulation |
•Hormones relay information to cells and are integrated with the nervous system to regulate responses to the internal and external environment •Autocrine •Paracrine •Endocrine |
|
|
Autocrine |
•Within the cell •Molecules act on the same cells that produce them |
|
|
Paracrine |
•Between local cells •Molecules act on cells that are close by •Neurotransmitters |
|
|
Endocrine |
•Between remote cells •Picked up by the circulatory system and transported to cells at a different area •Hormones |
|
|
Negative Feedback Loop of the Thyroid |
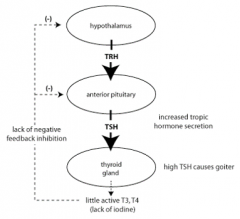
•TRH:thyroid releasing hormone •TSH:thyroid stimulating hormone •T3/T4:thyroid hormone |
|
|
Tropic Hormones |
stimulate the production and secretion of hormones by other endocrine glands.
ex. TSH |
|
|
Nontropic Hormones |
stimulates cellular growth, metabolism, or other functions; ex. thyroxine |
|
|
Regulation of Hormone Release |
•Chemical factors •Endocrine factors •Neural control •Negative feedback loop provides precise control •Endocrine, neurologic and immune systems work together to respond to stressors |
|
|
Chemical factors |
•Blood glucose (insulin), serum calcium (parathyroid hormone) |
|
|
Endocrine factors |
•Hormone from one gland controls another gland (HPAaxis) |
|
|
Negative feedback loop provides precise control |
•When altered, pathologic excess hormone is produced |
|
|
Endocrine,neurologic and immune systems work together to respond to stressors |
•General Adaptation Syndrome |
|
|
Hormone Transport |
•Water-soluble hormones circulate in “free” state (unbound) •Lipid-soluble hormones are bound to a carrier protein •Equilibrium between free and bound hormones •If protein levels are down, less hormones are bound |
|
|
Water-soluble hormones circulate in “free” state (unbound) |
•Large with high molecular weight •Expected half-life of seconds to minutes due to catabolism by enzymes •Short-acting responses •Bind to receptors on the cell surface (cannot diffuse into cells) -example: insulin |
|
|
Lipid-soluble hormones are bound to a carrier protein |
•Expected half-life is hours to days •Both short and long-acting responses •May bind to receptor or just diffuse through the plasma/nuclear membrane -example: cortisol and adrenal adrogens |
|
|
Hormone Action |
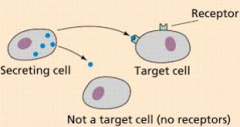
•Can only act upon cells/organs with appropriate receptors |
|
|
Two functions of Hormone Receptors |
1. Recognize and bind to the hormone with high affinity 2. Initiate the signal within the cell |
|
|
# of receptors on cells |
•Number of cell receptors can change as needed, within hours •More receptors, the higher the sensitivity in the cell |
|
|
Up-regulation (of receptors) |
-occurs with low concentration of hormone •Result: increase in the number of cell receptors |
|
|
Down-regulation (of receptors) |
• occurs with high concentration of hormone •Result: decrease in the number of receptors •Example:Insulin resistance |
|
|
Hormone receptor locations |
•Located in/on the target cell at two locations •In the plasma membrane of the target cell •In the intracellular compartment of the target cell |
|
In the plasma membrane of the target cell |
•For high molecular weight, water-soluble, unbound, that are freely circulating in serum •Example: drugs that act on the membrane-Catecholamine •Epinephrine and norepinephrine |
|

In the intracellular compartment of the target cell |
•Action once the lipid-soluble hormone has entered the cell •Example: steroid hormones synthesized from cholesterol •Androgens and Estrogens •Glucocorticoids and Mineralocorticoids •Thyroid hormones •Vitamin D |
|
|
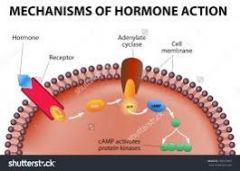
Hormone Actions |
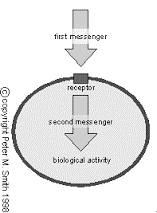
First Messenger Second Messenger |
|
|
First Messenger |
•Hormone secreted into the bloodstream •Brings a message to the cell via the receptor |
|
|
Second Messenger |
•Occurs as a result of the first messenger reaction •Signal is generated inside the cell •Mediates the effects of the hormone on the target cell Types of second messangers: •Cyclic AMP •Cyclic GMP •Enzymes |
|
|
Hypothalamic-Pituitary Axis (HPA) "Neuroendocrine system” |
•Central integration of neurologic and endocrine systems •Hormones produced for thyroid, adrenal, reproductive |
|
|
Hypothalamus |
•Connects to the pituitary by the pituitary stalk •Anterior pituitary via blood vessels •Posterior pituitary via nerve •Can produce releasing hormones that act on the pituitary |
|
|
Pituitary |
•Anterior pituitary= adenohypophysis •Posterior pituitary= neurohypophysis |
|
|
Posterior Pituitary Hormone Secretion |
•Secretes two hormones 1.Antidiuretic hormone (ADH) also called arginine vasopressin 2. Oxytocin |
|
|
Posterior Pituitary Hormones |
•These hormones are synthesized in the hypothalamus and stored in the posterior pituitary •Release is mediated by cholinergic and adrenergic neurotransmitters •Glutamate releases the hormones (Enhances) •GABA inhibits their release (Inhibits) •When released, they are in an unbound form •Free, water-soluble and cannot diffuse into a cell •Requires receptor on target cell membrane |
|
|
Posterior Pituitary: Antidiuretic Hormone (ADH) What does it do? |
•Controls plasma osmolality •Concentration of the plasma components |
|
|
Posterior Pituitary: Antidiuretic Hormone (ADH) Mechanism of Action |
•Increases permeability of distal renal tubules and collecting ducts •Increases water reabsorption from the kidney back into the blood (increases serum volume) •Reduces serum osmolality (makes it dilute) but increases urine concentration |
|
|
Posterior Pituitary: Antidiuretic Hormone(ADH) Regulation of secretion |
•Osmoreceptors in the hypothalamus •Baroreceptors in the left atrium, carotid arteries and aortic arch also aid in regulation |
|
|
Osmoreceptors in the hypothalamus |
•Stimulated when serum osmolality increases (concentrated) resulting in more ADH release •Reabsorption of water in the kidney and returned to the body (less urine, concentrated) •Reduced ADH secretion with low serum osmolality (dilute plasma) •Removes more water from the body via the kidney |
|
|
Baroreceptors in the left atrium, carotid arteries and aortic arch also aid in regulation |
•Are stimulated with volume loss, triggering ADH secretion, causing reabsorption of water in the kidney to return to the plasma •Reduced ADH secretion when intravascular volume is high, as in hypertension |
|
|
Oxytocin (posterior pituitary) |
•Contracture of the uterus and milk ejection, if lactating •Also an antidiuretic effect like ADH •Reduced waterloss via the kidney •Secreted in response to suckling •Binds to receptors on mammary cells and causes contraction of the cell •Let-down reflex •Also responds to distension of uterus •Causes contraction |
|
|
Anterior Pituitary |
•Larger portion of the pituitary (75%) •Connection is via blood vessels •Hormone production is regulated by: •Secretion of hypothalamic releasing hormones •Regulated by feedback from the hormones produced in the target cells •Also direct effects from neurotransmitters |
|
|
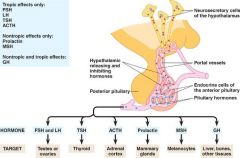
Anterior Pituitary Hormones |
•Follicle-stimulating hormone (FSH) -Influences reproductive function (not discussedhere) •Luteinizing hormone (LH) -Influences reproductive function (not discussedhere) •Thyroid-stimulating hormone (TSH) -Regulates thyroid gland activity, and thus TH production •Adrenocorticotropic hormone (ACTH) -Influences cortisol release from the adrenal cortex •Prolactin Influences milk production and ovulation •Melanocyte-stimulating hormone (MSH) -Secretion of melanin, darkening skin color •Growth hormone (GH) -This production is controlled by the hypothalamus •Growth hormone-releasing hormone (GHRH) increases GH production •Somatostatin inhibits GH production |
|
|
Anterior Pituitary Hormones (bloodvessel) |
|
|
|
Thyroid Gland (anterior pituitary) |
•Two-lobed gland joined by the isthmus •Normally not visible but can be felt during swallowing •Consists of follicular cells and parafollicular cells |
|
|
Follicular cells of thyroid gland |
•synthesize and secrete thyroid hormones (T3/T4) •Neurotransmitters may directly affect secretion from the neurons terminating in the thyroid gland |
|
|
Two Hormones secreted by Parafollicular Cells of thyroid gland
|
•secretes thyrocalcitonin and somatostatin |
|
|
Thyrocalcitonin |
•lowers serum calcium by inhibiting osteoclasts •Deficiencies do not cause hypocalcemia •Calcium regulation is regulated by parathyroid hormone |
|
|
Somatostatin |
•inhibits release of somatotropin, insulin and gastrin •Can have an effect on growth |
|
|
Thyroid Hormone (TH) Regulation |
•Regulated via negative feedback loop •TRH levels increase with -Exposure to stress -Exposure to cold -Decreased levels of T4 •TH isregulated by TSH and also by serum iodine levels •Adequate iodine is needed to produce TH •Production is usually elevated in response to demand •Puberty, pregnancy, iodine-deficient state, and immunologic, viral or genetic disorders |
|
|
Thyroid Hormone Transportation |
•TH is transported as both free and bound TH •Most is bound, therefore, longer acting and able to diffuse through membrane (fat soluble) •Majority is bound to thyroxine-binding globulin (TBG) •Lesser bound to thyroxine-binding pre-albumin (reservoir) •Free form is active (water soluble) •Short acting, binds to receptor on the target cell (cannot diffuse) |
|
|
What does thyroid hormone control |
•Controls the rate of metabolic processes in the body •Needed for neuro development in the fetus and infants •Affects neurologic functioning in adult •Alters protein, fat, and glucose metabolism •Increases heat production and oxygen consumption |
|
|
Parathyroid Glands |
•Four glands located behind the thyroid gland (can vary 2 to 6) •Produces parathyroid hormone (PTH) |
|
|
Parathyroid Hormone Function |
•Most important regulator of serum calcium •Increases serum calcium •Releases calcium from bone •Increases calcium reabsorption via the kidneys •Increase calcium absorption from the Gastrointestinal tract •Decreases serum phosphate •Reduces phosphate reabsorption via kidney |
|
|
Regulation of Parathyroid Hormone Levels(PTH) |

•NOT part of the Anterior Pituitary control •Controlled by blood concentration of Ca+ |
|
|
Calcium Regulation and PTH |
•1,25-Dehydroxy-vitamin D3 works as a cofactor with PTH •Promotes Calcium and phosphate absorption in the GI tract •Enhances bone mineralization (make bone) •Serum calcium decreases when serum phosphate increases •Forms a calcium-phosphate precipitate (forms insoft tissue) •Indirect stimulation of PTH if phosphate increases •Low serum magnesium levels can cause mild stimulation of PTH secretion, even if calcium is normal |
|
|
Adrenal Glands |
•Pair of organs located above each kidney •Consists of two separately functioning portions •Adrenal cortex (AnteriorPituitary control) •Adrenal medulla |
|
|
Adrenal cortex (AnteriorPituitary control) |
•Larger portion(80%) •Three zones which produce different steroid hormones (3 S’s: salt, sugar, sex) •Outer: mineralocorticoids (aldosterone: salt) •Middle: glucocorticoids (cortisol, cortisone, corticosterone: sugar) •Inner: adrenal androgens and estrogens (sex) Three stimulated by ACTH from pituitary |
|
|
Adrenal medulla |
•Smaller portion (20%) •Secretes catecholamines: epinephrineand norepinephrine •Innervated by SANS and PANS |
|
|
Mineralocorticoid: Aldosterone (adrenal cortex) |
•Aldosterone, most potent mineralocorticoid •Synthesis regulated by renin-angiotensin in renal system (angiotensin II) •Degraded by the liver and excreted via kidneys •Mechanism of action via the kidneys (distal nephron) •Increase sodium reabsorption •Increase potassium & hydrogen excretion •Takes 90 min to 6 hours |
|
|
Mineralocorticoid: Aldosterone (adrenal cortex) Affects |
•Affects transport in epithelial cell membrane resulting in •Sodium retention •Potassium and hydrogen loss •Other affects •Cardiac: enhanced contraction and ventricular pacemaker effect •Vessels: increased vascular resistance •Homeostasis: decreased fibrinolysis (Chronically elevated levels can lead to heart failure, resistant hypertension, insulin resistance) |
|
|
Glucocorticoids Produce Many Effects |
•Metabolic effect •Anti-inflammatory effect (affects innate and adaptive immunity) •Growth-suppressing effect •Other effects |
|
|
Metabolic effect |
•Increase blood glucose via gluconeogenesis in liver AND decreasing uptake into cells •Outside the liver, stimulates protein catabolism and inhibit protein synthesis |
|
|
Anti-inflammatory effect (affects innate and adaptive immunity) |
•Suppresses immunity via decreased T lymphocyte production, especially T-helper •Decreases the release of proteolytic enzymes |
|
|
Growth-suppressing effect |
•Inhibits bone formation and interferes with action of GH |
|
|
Other effects |
•Increases gastric acid secretion and interferes with calcium absorption •Increases number of circulating RBCs (polycythemia) •Increases appetite |
|
|
Cortisol: Natural Glucocorticoid |
•Main product of the adrenal cortex •Needed to maintain life and protect body from stress •90 minute half-life with most deactivation by the liver |
|
|
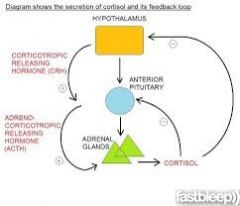
Cortisol: Natural Glucocorticoid Secretion |
•Secretion is regulated by ACTH from the anterior pituitary •ACTH binds to the cells of the adrenal cortex •Cortisol production and secretion occur immediately |
|
|
Cortisol: Natural Glucocorticoid Production |
•Production of ACTH is influenced by •Negative feedback (high levels of cortisol suppress/low stimulate) •Diurnal rhythm: peaks 3-5 hours after sleep begins •Stress increases production |
|
|
Adrenal Medulla |
•Made of chromaffin cells (pheochromocytes) •Release catecholamines directly into the bloodstream •Epinephrine(adrenalin) •Only 30% produced here (hormone); 70% from nerve terminals (neurotransmitter) •Norepinephrine •Stress to the body triggers acetylcholine which causes depolarization •Storage granules in chromaffin cells release catecholamines •ACTH and glucocorticoids also increase secretion •Once in bloodstream, remain for only seconds to minutes •Binds to plasma membrane receptors in target cells •Fight or flight response •Promotes glucose release |
|
|
Estrogens and Androgens |
•Secretion is regulated by ACTH from the anterior pituitary •Normally, minimal amounts are produced •Changes occur with pregnancy, menarche •Substancesfrom the adrenal cortex are weakly androgenic •Converted to stronger androgens and estrogens in peripheral tissue •Testosterone, estrogen •Adrenal sex hormones have the same biologic effect as those produced by the gonads •Will cover in greater detail in chapter 31 |
|
|
Pineal Gland and Melatonin |
•Made of photoreceptor cells that secrete melatonin •Release is stimulated by exposure to dark (more when asleep) •Release is inhibited by light exposure (less when awake) •Effects of Melatonin •Regulates circadian rhythms •Regulates reproductive system (GTRH) •Increases nitric oxide release from blood vessels •Removes toxic oxygen free radicals •Decreases insulin secretion •Tryptophan>>>>Serotonin>>>Melatonin |
|
|
Growth Hormone (somatotropin) |
•Stimulates growth, cell reproduction, and cell regeneration •Anabolic affect on the body’s tissues (builds up) •Interacts with a specific receptor on the surface of cells •Common effects •Increases muscle mass •Increases bone mineralization •Promotes lipolysis •Increases protein synthesis •Secreted by somatotropic cells in the anterior pituitary gland •Regulated by Growth Hormone Releasing Hormone |
|
|
Pancreas, a “Double Gland” |
Exocrine Endocrine |
|
|
Exocrine |
•portion produces digestive enzymes (Unit 11) •Will not address today |
|
|
Endocrine |
•portion produces hormones •Innervated from both SANS and PANS •Islets of Langerhans have 4 types of hormone-secreting cells •Alpha: secretes glucagon -Mobilizes glycogen in the liver •Beta: secretes insulin and amylin -Assists glucose to enter the cell (and exit the serum) •Delta: secretes somatostatin •F: secretes pancreatic polypeptide |
|
|
Insulin Secretion |
Regulated by three controls •Chemical control •Hormonal control •Neural control |
|
|
Chemical control |
•Increases when serum glucose rises •Diminishes with low serum glucose |
|
|
Hormonal control |
•Increases when GI hormones rise •glucagon, gastrin, cholecystokinin, and secretin •Diminishes with high levels of insulin (negative feedback loop) |
|
|
Neural control |
•Increases with parasympathetic stimulation (PANS) of Beta cells •Diminishes with sympathetic stimulation (SANS) of Alpha cells •Glucagon released by Alpha cells to stimulate gluconeogensis (>BS) |
|
|
Insulin Action At The Cell |
•Must bind to plasma membrane receptor •Cascade of actions that end with activation of glucose transporters •Allows glucose into the cell •Sensitivity of binding site maintains normal function •When insulin cannot bind, the cell is resistant to insulin •Linked to hypertension and diabetes •Action is anabolic (builds and requires energy) •Stimulate synthesis of proteins, carbohydrates lipids and nucleic acids •Reduce serum glucose level •Functions mostly in liver, muscle and adipose tissue •Brain, RBCs, kidney and lens do not require insulin for glucose transport •Facilitates intracellular transport of Potassium, phosphate and magnesium •Reduces serum K level |
|
|
Other Pancreatic Hormones |
•Glucagon (antagonist to insulin) •Amylin (satiety effect) •Gastrin (digestion) •Pancreatic somatostatin (digestion) •Grehlin (appetite control) |
|
|
Glucagon (antagonist to insulin) |
•Increases serum glucose via gluconeogenesis in muscle and lypolysis in fat •Release is stimulated by low glucose and SANS; inhibited by high serum glucose |
|
|
Amylin (satiety effect) |
•Co-secreted with insulin to control serum glucose •Delays nutrient uptake and suppresses glucagon secretion after meals |
|
|
Gastrin (digestion) |
•Stimulates gastric acid secretion |
|
|
Pancreatic somatostatin (digestion) |
•Essential in carbohydrate, fat, & protein metabolism •Different from hypothalamic somatostatin which inhibits GH and TSH •pancreatic somatostatin inhibits secretion of insulin |
|
|
Geriatric Issues with the Endocrine System Pituitary |
•Posterior with reduced ADH secretion •Less efficient kidney reabsorption of fluids •Anterior with decline in GH release •Decreased muscle tone, increased visceral fat |
|
|
Geriatric Issues with the Endocrine System Thyroid |
•gland atrophies, general decrease in TSH, T3and T4 |
|
|
Geriatric Issues with the Endocrine System Pancreas |
•glucose intolerance via decreased insulin receptor activity |
|
|
Geriatric Issues with the Endocrine System Adrenal |
•decreased synthesis of estrogen/ testosterone, cortisol secretion & Aldosterone |
|
|
Geriatric Issues with the Endocrine System Gonads |
•female: post menopause with decreased estrogen/progesterone, increased FSH •men: decreased testosterone (sex drive, muscle strength, bone) |
|
|
Endocrine Dysfunction |
1.Excessive function 2. Insufficient function |
|
|
Excessive function |
•Hypersecretionof hormone •Exaggerationof hormone action (tumor cells) |
|
|
Insufficient function |
•Hyposecretion of hormone orinactivation of it before reaching the target cell by antibodies •Inadequateblood supply •Lack of enoughprotein carriers in the serum |
|
|
Other Endocrine Issues |
•Abnormal cellreceptor function, usually a decreased number -Defectivehormone-receptor binding leading to insensitivity (Type II DM) •Alteredintracellular response to hormone-receptor response -Defect inpost-receptor signaling (lack of second messenger) |
|
|
Alteration of Hypothalamic-PituitarySystem |
•Hypothalamicdysfunction via a pituitary stalk issue -Head injury,destructive lesion, surgical transection -Loss of ALLhypothalamic hormones (Anterior pituitary) |
|
|
Anterior Pituitary: Hypopituitarism |
•Absence ofselective pituitary hormones or all of them -Usually lackof adequate hypothalamic-releasing hormones -Can be in thepituitary: space occupying lesion or infarction/ischemia --Infarctionresults in necrosis and edema which impedes blood supply to pituitary -Loss ofpituitary due to head trauma, infection, autoimmune |
|
|
Anterior Pituitary: Hypopituitarism Clinical Picture |
•Dependent onwhich hormones are affected •FSH •LH •TSH •ACTH •IGF-1 |
|
|
Hypopituitarism effect by hormone |
•FSH/LH -Loss ofsecondary sex characteristics •TSH -Thyroiddeficiency, growth •ACTH -Cortisoldeficiency •Prolactin -Inability tolactate postpartum •GH/IGF-1 -Poor growth inchildren |
|
|
TSH (thyroid stimulating hormone) |
•Rarely does ithappen alone •Takes 4-8weeks to develop symptoms -Coldintolerance -Dry skin -Mild myxedema -Lethargy/decreasedmetabolic rate •In general,less severe then primary hypothyroidismd |
|
|
ACTH (adrenocorticotropin hormone) |
•Rarely does ithappen alone •Loss ofcortisol and potentially life-threatening •Within 2weeks, symptoms include -Nausea/vomiting -Anorexia -Fatigue andweakness -Hypoglycemia -Decreasedurine output due to reduced GFR |
|
|
FSH (follicle stimulating hormone) LH (luetenizing hormone) |
•Reproductivechanges in women -Amenorrhea -Atrophicvagina, uterus and breasts -Decreasedlibido and body hair •In men, ingeneral -Testicularatrophy -Stunted beardgrowth -Decreasedlibido and body hair |
|
|
GH (Growth hormone) |
•Children -Often geneticin nature -Growth failure(hypopituitary dwarfism) •Adults -Pathophysiologicorigin is usually pituitary -Symptoms arevague •Socialwithdrawal •Fatigue/Loss ofmotivation •Osteoporosis •Reduced leanbody mass |
|
|
Hypopituitarism Diagnosis |
•Difficultdiagnosis -Signs andsymptoms may be very vague (TSH, ACTH, GH, FSH,…) -Labs(determined by symptoms) •Poor growth •Fatigue,weakness, nausea, vomiting -Imaging of thepituitary |
|
|
Hypopituitarism Treatment |
•Correctunderlying cause if possible (tumor, lesion) •Replacedeficient hormones -Lots ofchecking and monitoring of hormone levels -Oftentimesinjections -Growth hormone |
|
|
Hyperpituitarism: Primary Adenoma |
•AnteriorPituitary, slow growing benign tumors -Can be presentand cause no hazard -May causeexcess hormone secretion *Hypersecretion comes fromadenoma; therefore no negative feedback to control it •Can invade orcompress surrounding tissues -Hyposecretion if area isunder pressure: GH, FSH, LH -Visualdisturbances with optic nerve CV II (eyemovement with CV III, IV, VI) -Ifhypothalamus is involved, normal regulation is disturbed *wakefulness,thirst, appetite, temperature |
|
|
Hyperpituitarism: Primary Adenoma Clinical Picture |
•Clinicalpicture (varies with hormone affected and secretion pattern) •Headache,fatigue, neck pain, seizures •Visualchanges, often beginning in one eye •Excessivegrowth if GH is involved |
|
|
Hyperpituitarism: Diagnosis |
•Adenomas arefound via -Laboratorystudies *Specifichormone assays -Radiologicexam of the skull or MRI |
|
|
Hyperpituitarism: Treatment |
•Protect fromnegative effects of tumor growth (compression,..) -Tumor removalor resection •Controlhormone hypersecretion and itseffects -Medications orradiation |
|
|
Hypersecretion of Growth Hormone |
•Giantism: Children •Acromegaly:Adults |
|
|
Giantism: Children |
•Occurs whenepiphyseal plates are still open, causing excessive skeletal growth •Peripheralnerve damage from impingement/entrapment |
|
|
Acromegaly:Adults |
•Specific issuewith bone growth patterns -Slow growingand present for years before being diagnosed -Epiphysealplates are closed *Boneproliferation is seen as enlargement of the jaw, forehead, hands, feet *Enlargedtongue, interstitial edema, overactive sebaceous and sweat glands (BO) *Course skinand body hair, barrel chest due to enlongated ribs -Can causeearly death due to heart disease from hypertension, atherosclerosis, DM •Almost alwaysdue to GH-secreting adenoma -Unrestrainedsecretory pattern of GH (not related to sleep is a hint for diagnosis) |
|
|
Acromegaly and Giantism |
•Diagnosisvia clinical symptoms and elevated GH levels •Treatmentis to reduce GH levels and prevent complications of adenoma -Surgicalresection of GH secreting adenoma (immediate) -Radiationtherapy (will take time to lower GH levels) -Medicationsto lower GH levels (somatostatin analogs reduce GH secretion) *Lanreotide, Octreotide, Pasireotide |
|
|
Prolactinoma |
•AnteriorPituitary tumor may secrete increased prolactin •Most commonhormonally active pituitary tumor •Not the onlycause for increased prolactin •Renal failure•Polycysticovarian disease •Primaryhypothyroidism" |
|
|
Prolactinoma Clinical Picture |
•Amenorrhea(suppresses ovarian function) •Galactorrhea(milk production in a non-postpartum woman) •Hirsutism(estrogen deficiency) |
|
|
Prolactinoma Diagnosis and Treatment |
•Diagnosis •Investigatemedications as the possible cause; MRI finds the adenoma •Treatment•Adenomaremoval or medications to control the prolactin secretion |
|
|
Posterior Pituitary Abnormalities |
•Usually relateto abnormal secretion of ADH•Excessive secretion ADH •Deficientsecretion ADH |
|
|
Excessive secretion of ADH |
•Water retentionand hypo-osmolar condition(serum) -Urine outputis decreased •Diagnosis: Syndrome ofInappropriate Antidiuretic Hormone (SIADH) |
|
|
Deficientsecretion of ADH |
•Possibledehydration and hyper-osmolar (serum) -Urine outputis increased •Diagnosis:Diabetes insipidus (DI) |
|
|
Syndrome of Inappropriate AntidiureticHormone Secretion (SIADH) |
•High levels ofADH without a reason for it (feedback isOK) -Usually fromtumors that produce ADH, or -PulmonaryCause *Carcinoma orpneumonia, Cystic Fibrosis, mechanical ventilation -CNS Cause *Infections,tumor, trauma -Post-surgeryas a cause *Can cause highADH levels for 5-7 days -Medications *chlorpropamide, narcotics,analgesics, chemo, NSAIDS, antidepressants |
|
|
SIADH clincical picture |
•Waterreabsorption increases in the kidney from excess ADH -Concentratedurine: specific gravity >>1.010(normal is 1.005-1.035) -Increasedextracellular fluid volume and hyponatremia |
|
|
SIADH Diagnosis |
all must bepresent •Serum hypoosmolality and hyponatremium •Urine hyperosmolality(concentrated) •Urine sodiummatches intake •Normal adrenaland thyroid functioning •Absence ofconditions that would alter serum volumestatus |
|
|
SIADH Treatment |
•Correct causeof ADH excess (surgery) •Fluidrestriction •Demeclocycline: causes renaltubules to develop resistance to ADH and will decrease water reabsorption |
|
|
Diabetes Insipidus |
•Too little ADHaction, resulting in the inability of thekidneys to concentrate urine -Outcome: dilute urine, large quantities -8-10 L/day(normal is 1-2) with low specific gravity (<1.005) |
|
|
How many forms of Diabetes Insipidus |
•Two forms, ocuring at differentlevels 1. Central DI 2. Nephrogenic DI |
|
|
Central DI (Diabetes Insipidus)
|
•Insufficientsecretion of ADH from posterior pituitary -Tumor,aneurism, infection, closed-head injury -Can behereditary |
|
|
Nephrogenic DI (Diabetes Insipidus) |
•Renal tubulesdo not respond to ADH and therefore do not reabsorb water -Acquired: viadamage to tubule *pyelonephritis,amyloidosis, destructive uropathies, polycystickidney -Genetic: viadamage to the water transport channels in renal tubule |
|
|
Diabetes Insipidus ClinicalPicture |
•Polyuria, nocturia, and polydipsia (crave cold drinks) -Dehydration iffluids are not ingested/replaced regularly -High plasma(serum) osmolality and hypernatremia •Central DI hasabrupt onset •Nephrogenic isgradual and patient may have large bladder with nephrosis |
|
|
Diabetes Insipidus Diangnosis |
•Distinguishfrom other high urine output states -DM,osmotically induced diuresis, psychogenic polydipsia (xs water intake) -Waterdeprivation testing: continued large output despite lack of in input |
|
|
Diabetes Insipidus Treatment |
•Replace ADHusing DDAVP (desmopressin) and oralrehydration |
|
|
Alterations of Thyroid Function |
•PrimaryThyroid disorders (gland) •Secondary(Central) thyroid disorders |
|
|
Primary Thyroid disorders (gland) |
•Alteration inthyroid hormone (TH) levels with secondary feedback effects onThyroid-stimulating hormone (TSH) -TH levels riseand TSH decreases because of negative feedback |
|
|
Secondary (Central) thyroid disorders |
•Disorderoccurs at the level of the pituitary, affecting TSH secretion -With excessiveTSH production from pituitary *TH levelrises but no feedback to stop TSH production -With toolittle TSH productionfrom pituitary *TH levels arelow and remain low due to no increase in TSH via feedback loop |
|
|
Hyperthyroidism: Thyrotoxicosis |
•Increasedlevels of TH from the thyroid gland •Primaryhyperthyroidism: Gravesdisease, toxic adenoma •Secondaryhyperthyroidism: TSH-secretingpituitary adenoma |
|
|
Hyperthyroidism: Thyrotoxicosis Clinical Picture |
•Increasedmetabolic rate •Increasedtissue sensitivity to SANS stimulation •Intolerance toheat•Goiter --> |
|
|
Hyperthyroidism: Thyrotoxicosis Diagnosis |
•Primaryhyperthyroidism (Thyroid gland) -Elevated T3& T4 with decreased TSH (negative feedback intact) •Secondaryhyperthyroidism (Central cause) -Normal toincreased TSH with elevated T3 & T4 *Here, theelevated T3/T4 is not signaling the reduction in TSH |
|
|
Hyperthyroidism: Thyrotoxicosis Treatment |
•Control excessTH production (T3/T4), secretion or action -Surgery toremove adenoma -Radioactiveiodine therapy to thyroid -Anti-thyroiddrug therapy *Blocks T4conversion to active T3 |
|
|
Graves Disease |
•50-80% of allhyperthyroidism, more common in females •Autoimmunedisease -Geneticfactors interacting with environmental triggers -Form ofhypersensitivity reaction *Thyroid hastissue-specific antigens on its cell membranes *Body producesantibodies and attaches to antigen receptor ^Thyroid-stimulatingimmunoglobulin (TSI) *Causes thyroidto malfunction and overproduce TH (goiter) *TSH is reduceddue to negative feedback loop |
|
|
Graves Disease Clinical Picture |
•As withhyperthyroidism, plus from Thyroid-stimulating Ig -Exophthalmia,blurred vision, photophobia, decreased acuity *Hyperactivityof SANS *Infiltrativechanges in the orbit and ocular muscles -Pretibialmyxedema (Graves dermopathy) *Subcutaneousswelling of the shins *Indurated andedematous |
|
|
Graves Disease Diagnosis and Treatment |
Diagnosis •T3/T4 elevatedwith very low TSH Treatment •Ablationtherapy with radioactive iodine (replacement will be needed) •Antithyroid medications(PTU) •Medications tocontrol the signs/symptoms if mild |
|
|
Thyrotoxic Crisis (Thyroid Storm) |
•Rare butdangerous worsening of thyrotoxic state -Can die within48 hours if not treated -Usually foundin undiagnosed or undertreated Graves disease *With anadditional stress ^Infection,pulmonary/cardiac disorder, trauma, seizure |
|
|
Thyrotoxic Crisis (Thyroid Storm) Clinicalpicture |
•Hyperthermia •Tachycardiawith atrial dysrhythmia, high-output heat failure •Agitation anddelirium •Nausea,vomiting or diarrhea |
|
|
Thyrotoxic Crisis (Thyroid Storm) Diagnosis |
•Laboratorystudies and clinical picture •T3/T4 elevatedwith very low TSH |
|
|
Thyrotoxic Crisis (Thyroid Storm) Treatment |
•Aimed atsymptoms which are due to increasedbeta-adrenergic receptors and catecholamines -Medicationthat blocks T3/T4 synthesis *Propylthiouracil (PTU) *Methimazole -Beta-blockersfor cardiovascular issues -Steroids -Supportivecare |
|
|
Hypothyroidism |
•Insufficientproduction of TH from the thyroid gland •Most commonthyroid disorder; women more than men |
|
|
Two forms of Hypothyroidism |
•Primaryhypothyroidism (99% of allcases) •Secondary(Central) hypothyroidism |
|
|
Primaryhypothyroidism (99% of allcases) |
-Loss ofthyroid function at the gland: decreased TH despite increased TSH and TRH •Autoimmune(Hashimoto’s thyroiditis) •Loss ofthyroid tissue after surgery/radiation •Iodinedeficiency |
|
|
Secondary(Central) hypothyroidism |
-Pituitary doesnot produce adequate TSH or a lack of TRH, resulting in low TH, TSH, TRH •Pituitarytumor •Traumaticbrain injury •Subarachnoidhemorrhage |
|
|
Hypothyroidism Clinical Picture |
-Insidious andeffects most body systems •Low basalmetabolic rate *Weight gaindespite no change in diet •Coldintolerance (poor heat production) •Lethargy (notdue to aging) •Goiter (fromexcessive TSH effect on thyroid) •Myxedema, iflongstanding *Nonpitting edema ofeyes, hands, feet *Myxedema comais a medical emergency |
|
|
Hypothyroidism Diagnosis |
•Primary -Clinical features pluslabs: elevated TSH with decreased T3 & T4 •Secondary -Clinicalfeatures plus labs: TSH, T3 and T4are all low |
|
|
Hypothyroidism Treatment |
•Treatment for all ishormone replacement therapy -levothyroxine (Synthroid) *Dose istitrated to keep the TSH normal for Primary disease |
|
|
Specific Hypothyroid Conditions |
•PrimaryHypothyroidism •CongenitalHypothyroidism |
|
|
PrimaryHypothyroidism |
•Autoimmunethyroiditis (antibodies destroy the gland) -Hashimoto’sthyroiditis and chronic lymphocytic thyroiditis •Subacutethyroiditis: due to viral illness •Painlessthyroiditis: similar process as Hashimoto •Postpartumthyroiditis: similar process as Hashimoto |
|
|
CongenitalHypothyroidism |
•Occurs ininfants who lack thyroid tissue or have TH synthesis defects •Mandatorynewborn screen -Symptoms wouldnot show til ~4months and could have irreparabledamage to cognition by then |
|
|
Thyroid Carcinoma |
•Most commonendocrine malignancy -Ionizingradiation, especially during childhood -Usually foundvia exam since T3/T4 are usually normal *Change invoice and swallowing/difficulty breathing *Metastatictumor in lungs, brain or bone |
|
|
Thyroid Carcinoma Diagnosis andtreatment |
•Found vianeedle biopsy •Treatmentincludes -Thyroidectomy -TSHsuppression therapy (Levothyroxine T4) -Radioactiveiodine -Chemotherapy |
|
|
Hyperparathyroidism |
•Greater thannormal secretion of parathyroid hormone (PTH) andhypercalcemia |
|
|
Two forms of Hyperparathyroidism
|
•PrimaryHyperparathyroidism (gland level) •SecondaryHyperparathyroidism (other than gland) |
|
|
PrimaryHyperparathyroidism (gland level) |
•Excessive PTHfrom one of the parathyroid glands and not under feedback control of elevatedcalcium to inhibit PTH -Parathyroidadenomas, hyperplasia or carcinoma |
|
|
SecondaryHyperparathyroidism (other than gland) |
•Compensatorymechanism to chronic hypocalcemia -Secretion ofPTH is elevated, but cannot maintain normal calcium levels due to lack of Vit D/calciumintake *Some drugsinterfere with Vit D absorption ^Phenytoin, phenobarb and laxatives |
|
|
Hyperparathyroidism Clinical Presentation |
•May beasymptomatic or display symptoms of hypercalcemia/hypophosphatemia -Fatigue,headache, depression -Anorexia,nausea and vomiting -Pathologicfractures (from bone resorption), vertebral compression fractures, kyphosis -Calcium renalstones due to increased calcium renal filtration, alkaline urine and increasedrenal phosphate excretion *Can lead toimpaired renal function, hydronephrosis |
|
|
Hyperparathyroidism Diagnosis |
•Primary (nonegative feedback) -Increasedserum calcium levels along with elevated PTH level •Secondary(feedback is present) -Low serumcalcium levels with elevated PTH level -Look forchronic renal failure as the cause |
|
|
Hyperparathyroidism Treatment |
•Primary -Surgicalremoval of adenoma -Removal ofthree of the four glands for hyperplasia •Secondary -Calcium/vitaminD replacement -Dietaryphosphate restriction -Phosphatebinders |
|
|
Hypoparathyroidism |
Abnormally lowPTH levels •Most commoncause is damage during thyroid surgery •Geneticsyndromes: DiGeorge syndrome,familial hypoparathyroidism Low magnesiumalso affects calcium and phosphate •Decreases PTHsecretion and PTH function •Whenhypomagnesemia is corrected, PTH secretion returns to normal and tissuesrespond as they should |
|
|
Results of low parathyroid Hormone |
•Depressed serumcalcium (impaired bone resorption/kidney reabsorption) •Increasedserum phosphate (kidney reabsorbs phosphate when PTH is inadequate) -Further lowerscalcium concentration by inhibiting Vit D (poorer GI absorption) |
|
|
Hypoparathyroidism Clinical Picture |
Reflectshypocalcemia •Nerve/muscleexcitation due to reduced threshold -Tetany/musclespasms, Hyperreflexia, Tonic-clonic convulsions -Laryngealspasms>>>asphyxiation -Dry skin andloss of body/scalp hair -Horizontalridges on the nails -Cataracts andbone deformities |
|
|
Hypoparathyroidism Diagnosis |
•Low PTH levelsplus •Low serumcalcium with high phosphorus without kidney failure, intestinal malabsorption or nutritionaldeficiency |
|
|
Hypoparathyroidism Treatment |
•Parenteralcalcium for acute state •Vit D and calciumreplacements for a more chronic state |
|
|
Diabetes Mellitus (DM) |
•Group ofdiseases of the endocrine pancreas with high serum glucose resulting from a lack of insulin,defect in insulin action, or both •8.3% of Americans |
|
|
Four types of Diabetes Mellitus (DM) |
1.Type 1 DM •Beta celldestruction leading to insulin deficiency 2. Type 2 DM •Insulinresistance or insulin secretory defect 3. Otherspecific types 4. GestationalDM •Dysregulationoccurring during pregnancy |
|
|
Diagnosis of DM |
Based onseveral laboratory values •Glycosylatedhemoglobin (HbA1C) > or = 6.5% -Glucosepermanently attaches to hemoglobin -Lab reflectsaverage plasma glucose level in the last 120 days *Gives a betteridea of control over time •Fasting plasmaglucose (FPG) > or = 126mg/dL -Only reflectsvalue at this moment •Oral glucosetolerance testing (OGTT) > or = 200mg/dL -Serum glucoselevel two hours after ingesting 75 g of glucose •Random serumglucose level > or = to 200 mg/dL -Only reflectsvalue at this moment |
|
|
Type 1 DM |
•Most commonpediatric chronic illness -Rare under 9months and peaks at about 12 years |
|
|
Two Types of Type 1 DM |
•Autoimmune,also known as type 1A -More common ofthe two types •Nonimmune,also known as type 1B -Far lesscommon and due to other diseases, such as pancreatitis -More common inAsian and African descent |
|
|
Pathophysiology of Type 1A DM |
•Slowlyprogressive autoimmune disease -Geneticassociation seen with HLA –DQ and HLA-DR *HLA-DR isassociated with other autoimmune diseases ^Graves,Hashimoto and Addison’s disease *Gene-environmentinteraction results in autoantigens on the membrane of the beta cells -Immune systemmediates the disease and destroys the beta cells *Cellularimmunity via T cytoxic cells andmacrophages *Humoralimmunity via autoantibodies (immunoglobulins) -Symptoms ofdisease are not seen until 80-90% of beta cells are destroyed *Can be presentfor a while |
|
|
Pathophysiology of Type 1A DM (cont) |
•Insulinnormally suppresses glucagon -Glucagonincreases serum glucose bygluconeogenesis in muscle and lypolysis in fat -Release ofglucagon is stimulatedby low glucose and SANSstimulation -Release ofglucagon is inhibited byhigh serum glucose andinsulin •Withoutinsulin, glucose production rises via glucagon •Amylinsecretion is also decreased -Normallysuppresses glucagon release form the pancreatic alpha cells -Withoutamylin, glucose production rises viaglucagon |
|
|
Type 1A DM Clincal Manifestations |
•Longpreclinical period with gradual destruction of beta cells -At 80-90%destruction, symptoms are seen *Hyperglycemiawith insulin deficiency ^Widefluctuations occur *Glucosuria as renalthreshold is exceeded ^Causes osmoticdiuresis: polyuria with reflex polydypsia (thirst) *Weight lossdue to breakdown of protein and fat because of the lack of insulin ^This breakdownproduces circulating ketones; can be seen in urine if threshold is exceeded(check urine for ketones) |
|
|
Type 1A DM Diagnosis |
•Diagnosis fromsymptoms and laboratory values -Symptoms *Polyuria,polydipsia, polyphagia -Labs (also some specific autoantibodies) *HbA1C > or = 6.5% *Fasting Plasmaglucose > or =126mg/dL *Oral glucosetolerance test > or = 200mg/dL *Random serumglucose level > or = to 200 mg/dL -Many with Type1A DM are not diagnoseduntil they presentwith DiabeticKetoacidosis (DKA) which can be life-threatening *Acetone, avolatile form of ketones isproduced in DKA ^This fruityscent can be smelled when they exhale Importantassessment |
|
|
Type 1A DM Treatment |
•Achieveoptimal glucose without causing hypoglycemia -Insulin therapy *Short or longacting preparations *Subcutaneousvia injections or insulin pump -Meal planning *Carb countingis common and utilizes short acting insulin coverage ^“give 2 unitsof humalog for every 10carbs ” -Exerciseregimen *Consistencyand balancing with insulin to control blood sugar -Monitorchronic complications *Renal, nervoussystem, cardiac, PV, renal and bone |
|
|
Type 2 DM |
•More commonthan type 1 and rising in incidence -> 10% ofAmericans *Highest inblack women *Affecting morechildren, especially Native American and obese |
|
|
Type 2 DM Risk Factors
|
•Age •Obesity •Hypertension •Physicalinactivity •Family history •Metabolicsyndrome |
|
|
Metabolic Syndrome |
A group ofdisorders that places one at high risk for Type 2 -Waistcircumference •>40 in formales; > 35 in for females -Triglycerides •> 150 mg/dL -HDL levels •< 40 mg/dL for males;< 50 mg/dL for females -Blood pressure •> or = to130/85 mmHg -Fasting bloodglucose •> or = to100mg/dL |
|
|
Type 2 DM Pathophysiology |
•Multiple geneabnormalities which result in -Insulinresistance in target organs -Decreasedinsulin secretion by pancreatic beta cells •Insulinresistance -Suboptimal response to insulin intarget cells/tissues *Especiallyliver, muscle, adipose tissue -Obesitycontributes to resistance in many ways *Increasedinflammation *Interferencewith intracellular signaling *Hyperinsulinemiawith decreased insulin receptors |
|
|
Type 2 DM Pathophysiology, cont’d |
•Increasedinsulin production masks diabetes for years until beta-cell dysfunction occursand decreased insulin production sets in (“exhaustion”) -Both decreasedbeta-cellfunction and beta-cell mass •Glucagonconcentration increases -Alpha cellsbecome less responsive to glucose inhibition -Blood glucoseincreases because glucagon stimulates glucogenolysis and gluconeogenesis •Amylin levelsare deficient, causing increased glucagon •GI hormonesalso play a role in insulin resistance -Ghrelin |
|
|
Type 2 DM Clinical Picture |
-Overweightwith dyslipidemia and hypertension -Polyuria andpolydipsia -Nonspecificsymptoms *Fatigue, pruritis, recurrentinfections, visual changes, neuropathy •Latersymptoms, if not treated -Coronaryartery disease -Peripheralartery disease -Cerebrovascularaccident |
|
|
Type 2 DM Diagnosis |
(noautoantibodies) •HbA1C > or = 6.5% •Fasting Plasmaglucose > or = 126mg/dL •Oral glucosetolerance test > or = 200mg/dL •Random serumglucose level > or = to 200 mg/dL |
|
|
Type 2 DM Treatment |
•Restore normalblood sugar and correct metabolic disorders -Dietarychanges and exercise may be enough *Weight lossreduces insulin resistance (improved glucose tolerance) •Medicationsfor optimal management -Oralhypoglycemic (improves insulin sensitivity) -Insulin onlywhen/if beta-cell function is lost |
|
|
Gestational Diabetes |
•Glucoseintolerance with onset duringpregnancy •Complicates 7%of pregnancies •Fetus growsvery large due to mother’s high BS levels (LGA) •Received fromplacental blood flow •Risk factors •Older age,family history, history of glucose intolerance, certain ethnic groups, priorpoor obstetric outcome •Possible type1 or 2 prior to pregnancy •Diagnosis aswith type 2 •Especially Oral GlucoseTolerance Test •Treatment isto control BS throughout pregnancy •35-60% chanceof DM in next 10-20 years for themother |
|
|
Acute Complications of DM Hypoglycemia |
•More common intype 1 versus type 2, unless taking insulin sulfonylureas or exogenous insulin •Glipizide, Glyburide,Glimepiride •Stimulatesinsulin release from pancreas •Reducesglucose output from the liver |
|
|
Hypoglycemia Symptoms |
•Pallor,tremor, anxiety, diaphoresis, irritability•Tachycardia,palpitations •Headache,dizziness, poor judgement, confusion, seizure, coma •Treatment:glucose replacement •Orally (glucosesource) or IV (glucagon) |
|
|
Acute Complications of DM DiabeticKetoacidosis (DKA) |
•Deficiency ofinsulin with increase of counter-regulatory hormones -GH, catacholamines, cortisol,glucagon6 |
|
|
Acute Complications of DM Diabetic Ketoacidosis (DKA) Diagnosis |
1.BS > 250mg/dL 2.Serumbicarbonate <18mg/dL 3.Serum pH <7.30 4.Presence ofanion gap 5.Ketones inurine and serum |
|
|
Acute Complications of DM Diabetic Ketoacidosis (DKA) Clinical presentation |
•CNSdepression, ketonuria, Kussmalrespirations to compensate for acidosis, postural dizziness, anorexia, nausea, abdominal pain, thirst,polyuria |
|
|
Acute Complications of DM: DKA |
•Pathophysiology •Insulinprevents fat catabolism, so when deficient, fat breakdown is enhanced •Fatty acidsdelivered to the liver resulting in glyconeogenesis with the production of ketone bodies of themitochondria •Ketoneproduction > ketone peripheral use •Ketoneaccumulation causes metabolic acidosis |
|
|
Acute Complications of DM: DKA Treatment:Emergency |
•Hydration and slow restorationof acceptable blood sugar •Complicatedand often ICU managed |
|
|
Acute Complications of DM Dawnphenomenon |
•Early morningrise in BS with no hyperglycemia during the night due to nocturnal elevationsof Growth Hormone •GH causesincrease insulin-like growth hormone factor |
|
|
Chronic Complications of DM |
•Mostcomplications are associated with chronic hyperglycemia •Microvascular:retinopathies,nephropathies, neuropathies •Macrovascular:coronaryartery, PV, and cerebral vascular disease |
|
|
Hyperglycemia |
•causesnegative complex metabolic pathways •Polyol pathway •Protein KinaseC •Nonenzymatic glycation •Goal is tomaintain a normal serum glucose levels •Less strictwith type 2 DM |
|
|
Hyperglycemia and the Polyol Pathway |
•Body’s methodto compensate for high glucose level •Tissues thatdon’t need insulin cannot down regulate intake when blood sugar is high so itkeeps entering the cells •Kidney, RBC, bloodvessels, eye lens, nerves •Excessintracellular glucose is shunted to the polyol pathway, contributing to twocomplications 1. Excessiveaccumulation of polyol (sorbitol) •Increasesintracellular osmotic pressure •Water flowsinto the cell •Causesswelling in the lens>>visual changes, predisposition to cataracts 2. Reductionin the level of glutathione, an important antioxidant •Oxidativeinjury occurs in cells/tissues |
|
|
Hyperglycemia and Protein Kinase C |
•Protein KinaseC is an enzyme involved in many processes •Binding ofhormones •Plateletactivation •Tumorpromotion •Contributes tomicrovascular complicationsof DM •Protein kinaseC is inappropriately activated with hyperglycemia •Insulinresistance •Production ofextracellular matrix •Pro-inflammatorycytokines•Vascularendothelial proliferation•Increasedpermeability••r v |
|
|
Hyperglycemia and Non-enzymatic Glycation |
•Glucose, undernormal conditions, reversibly attaches to proteins, lipids and nucleic acids •This is a goodthing •Duringpersistent hyperglycemia, glucose is irreversibly bound to proteins in bloodvessels, interstitial tissue, and cells •Causes injuryor pathologic conditions resulting in diabetic complications •In hemoglobin,it decreases its ability to transfer OxygenN |
|
|
Microvascular Disease |
•Occurs in thecapillaries and results in •Lesions occurand include •Severity isdependent on |
|
|
•Occurs in thecapillaries and results in |
•Retinopathy(retina) •Nephropathy(kidney)Neuropathy(nervous system |
|
|
•Lesions occurand include |
•Thickening ofbasement membrane •Endothelialhyperplasia •Thrombosis |
|
|
•Severity isdependent on |
•Duration ofthe disease (10 yrs) •Status ofglycemic control |
|
|
Microvascular: Diabetic Retinopathy |
•Leading causeof blindness in < 60 yr olds in US •Cataracts andglaucoma are also common •Retinaldetachment is a possibility •Develops morerapidly in type 2 (longstanding hyperglycemia) •Underlyingpathology •Hypoxia,damage to retinal blood vessels and RBC aggregation •Macular edemacauses decreased vision •Sorbitol(polyol) accumulation in lens causes blurred vision |
|
|
Microvascular: Diabetic Nephropathy |
•Most commoncause of End-stage kidney disease •More common intype 1 than type 2 •Exact processis unknown, but all processes mentionedup to now are included •Renalglomerular changes occur resulting in glomerulosclerosis with decreased bloodflow and filtration •Starts earlyin diabetes process •First clinicalsign is microalbuminuria (special test, not a dipstick) •Such a smalllevel that it requires an immunoassay •Once frankproteinuria is present, life expectancy is <10 years |
|
|
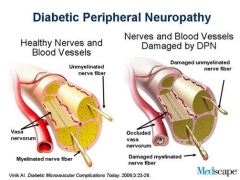
Microvascular: Diabetic Neuropathies |
•Most commoncomplication of DM •Chronichyperglycemia causes vascular changes resulting in ischemia & demyelinationof nervous tissue •Nervedegeneration and delayed conduction •Somatic andperipheral nerves cells are damaged •Sensory lossis more common than motor deficits •Often theneuropathies are progressive, but some can improve •Can alsoinclude visceral issues from autonomic neuropathy •Delayedgastric emptying Impotence •Diabeticdiarrhea Orthostatic hypotension •Heart rate variability Altered bladder function |
|
|
Diabetic Peripheral Neuropathy |
|
|
|
Macrovascular Disease |
•Lesions inlarge and medium-sized vessels cause increased morbidity and mortality •Particularlywith type 2 DM •Acceleratedatherosclerosis and coronary artery disease, along with stroke and peripheralvascular disease •Glycosylatedend-products attach to the proteins in the blood vessel walls •Promotesoxidative stress/endothelial dysfunction •Process isaccelerated by the presence of •Hyperlipidemia •Hypertension |
|
|
Macrovascular: Coronary Artery Disease |
•Prevalenceincreases with duration of disease (not severity) •CongestiveHeart Failure also higher with DM •Due tocollagen in ventricular wall which decreases compliance •Mechanism ofdisease •Hyperglycemiaand insulin resistance •High LDLs andtriglycerides (bad ones) •Low HDLs (goodones) •Plateletabnormalities •Increasedadhesion and decreased fibrinolysis (thrombus formation) •Endothelialcell dysfunction •Ultimate causeof death in 75% of those with DM |
|
|
Macrovascular: Stroke and PVD |
•Stroke is morecommon with DM due to platelet abnormalities •Type 2 is moreat risk •Survival afterstroke is reduced with DM •PVD increaseswith age and duration of DM •Most common inarteries below the knee •Claudication,ulcers, gangrene and amputation •Loss ofsensation •Increased riskof infection complicates issues |
|
|
DM and Infection |
•Increased riskfor infection •Retinalchanges and neuropathy put the patient at risk for injury and loss ofprotection (innate immunity) •Tissues aremore hypoxic due to glycosylated hemoglobin •Impedes therelease of oxygen •Pathogens canreplicate rapidly due to available glucose •Vascularchanges decrease blood supply, especially WBCs •Those that arepresent cannot get to the site •Hyperglycemiaimpairs adaptive immune response, often masking signs of infection |
|
|
Teaching Patients About Diabetes |
•Normal bloodsugar versus individualized patient goal •Normal fastingis considered 60-99 mg/dL but theirgoal may be allowed to go higher •Over 126, onthree occasions is diagnostic •Random bloodsugar readings may be much higher (200) •NormalHemoglobin A1C versus individualized patient goal •Normal isconsidered about 5.5% (6) but often the goal is 7% for patients with DM •How can youhelp patients relate the two systems? •Simplecalculation gives some help (not perfectbut an easy calculation) •(HgA1C - 2)x 30 =approximate equivalent to the BS |
|
|
Disorder of the Adrenals: Hypercortical Function |
•Three types orcauses Cushing Syndrome Cushing Disease Cushing-like Syndrome |
|
|
Cushing Syndrome |
•exposure toexcess cortisol |
|
|
Cushing Disease |
•excessendogenous secretion of ACTH |
|
|
Cushing-like Syndrome |
•from exogenousintake of glucocorticoids (steroid therapy) |
|
|
Disorder of the Adrenals: Hypercortical Function |
•Pathophysiology •Normalcircadian secretion patterns of ACTH and cortisol are lost •Poorregulation of cortisol, especially negative feedback •Excesscortisol is present |
|
|
•Without thefeedback loop intact, •ACTH continuesto be produced by the anterior pituitary •Adrenalscontinue to produce cortisol |
|
|
Hypercortical Function Clinical Picture |
•Weight gainwith adipose tissue in •trunk (truncal obesity) •face (moon face) •cervical area (buffalohump) •Glucoseintolerance from cortisol-induced insulin resistance •Proteinwasting from catabolic affect of cortisol •Striae due to lossof collagen •Bruising dueto loss of support around small vessels •Infections dueto suppression of immune system |
|
|
Hypercortical Function Diagnosis |
•Labs: •Hyperglycemia •Glycosuria •Hypokalemia,metabolic acidosis •Elevatedurinary free cortisol levels •Imaging fortumors |
|
|
Hypercortical Function Treatment |
•Correct thecause of the overproduction of cortisol •Medications •Radiation •Surgery |
|
|
Disorder of the the Adrenal:Adrenocortical Hypofunction |
•Addisondisease: Primary adrenal insufficiency •Caused byautoimmune destruction of adrenal cells •Often withchronic infections (TB) |
|
|
Disorder of the the Adrenal:Adrenocortical Hypofunction Pathophysiology |
•Inadequatecorticosteroid and mineralocorticoid with elevated ACTH (loss of negativefeedback) •90% of adrenaltissue is gone before symptoms are seen |
|
|
Disorder of the the Adrenal:Adrenocortical Hypofunction Clinical Picture |
•Weakness andfatigue •Hyperpigmentationand vitiligo •Hypotension,progressing to vascular collapse |
|
|
Adrenocortical Hypofunction Diagnosis |
•Clinical signsand symptoms •Low serum cortisol •High serum ACTH |
|
|
Adrenocortical Hypofunction Treatment |
•Lifetime replacement •glucocorticoid(cortisol-steroids) •Helps controlinflammation •Mineralocorticoid(spironolactone) •Helps increasewater excretion in the distal tubules by competing for receptor sites |
|
|
Disorder of the Adrenal: CongenitalAdrenal Hyperplasia |
•Enzymedeficiency for cortisol synthesis in utero •Since cortisolremains low, ACTH levels remain high, inducing the production of the 3 S’s •Sex steroids(androgens) increase •Salt(mineralocorticoids) increase |
|
|
Disorder of the Adrenal: CongenitalAdrenal Hyperplasia clinical picture and Treatment |
•Clinicalpicture •Female infantsexperience virilization (ambiguousgenitalia) •Both sexesexperience salt wasting •Treatment •Lifelongreplacement of glucocorticoids and mineralocorticoids |
|
|
Disorder of the the Adrenal: Hyperaldosteronism |
•Excessivealdosterone secretion from adrenal cortex (salt) •Primary: abnormality in adrenal cortex (adenoma) •Secondary:extra-adrenal stimulus of aldosterone secretion," |
|
|
Disorder of the the Adrenal: Hyperaldosteronism Pathophysiology |
•Primary: fluidand electrolyte imbalances due to excess aldosterone •Secondary:variable, depending on renin productionragment- |
|
|
Disorder of the the Adrenal: Hyperaldosteronism Clinical picture |
•Hypertension,leading to L ventricular hypertrophy if not treated •Hypokalemia |
|
|
Hyperaldosteronism Diagnosis |
•Blood Pressureelevation •Serum K is low (normalis 3.5-5.3) •Aldosterone ishigh •Imaging for adenoma |
|
|
Hyperaldosteronism Treatment |
•Surgery if adenoma •Medical management •Blood Pressure •K level--EndFragment--> |
|
|
Hypersecretion of AdrenalAndrogens/Estrogens |
•Can be causedby •Adrenal tumors •Cushingsyndrome •Defect insteroid synthesis •Hypersecretionof estrogen causes feminization in men •Gynecomastia,testicular atrophy and decreased libido •In femalechildren, early secondary sex characteristics and advanced bone age •Hypersecretionof androgen causes virilization in women •Hirsutism,deepening of voice, amenorrhea, breast atrophy |
|
|
Tumor of the Adrenal Medulla |
•Pheochromocytoma •Causesexcessive production of catecholamines |
|
|
Tumor of the Adrenal Medulla Clinical picture(increased SANS) |
•Persistenthypertension •Headache(cerebral blood flow), pallor, diaphoresis •Tachycardiaand palpitations •Acute eventscan be triggered by situations or food |
|
|
Tumor of the Adrenal Medulla diagnosis and treatment |
•Diagnosis •Elevatedlevels of serum catecholamines; imaging tofind the tumor •Treatment •Control theeffects of catecholamines: alfa andbeta adrenergic blockers •Excision ofthe tumor |