Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
72 Cards in this Set
- Front
- Back
|
Describe the release of GnRH
|
D-Secreted in a pulsatile manner into the hypophysial portal blood
-Stimulates the pituitary to make both FSH and LH |
|
|
What are the gonadotrophins?
|
FSH and LH
|
|
|
Describe the actions of FSH
|
Stimulates follicular growth in the woman and spermatogenesis in the man
|
|
|
Describe the actions of LH
|
Male:
Stimulates androgen secretion Female: -Stimulates estrogen secretion -Triggers the LH surge at midcycle -Triggers progesterone secretion -Maintains the corpus luteum during the luteal phase of the cycle |
|
|
What hormones are produced by the gonads?
|
Steroid hormones (testosterone, estradiol, estrogen, inhibin)
|
|
|
Describe the gonadal steroid hormone feedback in males
|
Testosterone has only negative feedback at the level of the pituitary and causes hypothalamus to turn off GnRH and gonadotrophin secretions
|
|
|
Describe the gonadal steroid hormone feedback in females
|
-Estradiol has negative feedback effects
-The rapid rise in estrogen during the midfollicular phase of the cycle has a positive feedback effect -It can trigger the LH surge |
|
|
Describe inhibin
|
-Made by the granulosa cells and Sertoli cells
-Feeds back at the pituitary to turn off FSH secetion |
|
|
Describe how the GnRH axis is controlled by sex hormones
|
-GnRH neurons dont have sex steroid receptors
-A number of other neurons impact on the GnRH neurons which are regulated by sex steroids -These include dopamine, NE, beta-endorphin (endogenous opiod), and kisspeptin |
|
|
Describe Kisspeptin
|
Stimulates GnRH secretion
|
|
|
What can control GnRH secretion?
|
-Sex hormones
-Kisspeptin -Overall stress -Corticotropin releasing factor |
|
|
Describe the GnRH response in stress
|
-Cortisol and CRH goes up during stress
-CRH not only stimulates the adrenal axis but also secondarily suppresses the gonadal axis through an endogenous opiod mechanism |
|
|
Describe how kisspeptin works
|
-Works via a receptor that is present on GnRH neurons
-Very important in stimulating GnRH release -Can help explain differences in + and - feedback in males and females |
|
|
Describe kisspeptin in females
|
There are two sets of kisspeptin neurons which mediates negative feedback and another group of neurons that mediates positive feedback of estrogen on GnRH
|
|
|
Describe kisspeptin in males
|
-Lack some of the neurons of females
-Dont get the positive feedback effects of steroids |
|
|
What occurs if you infuse kisspeptin?
|
Stimulate LH secretion
|
|
|
What is the result of abnormalities of the kisspeptin receptor or gene?
|
Hypogonadalism on a hypothalamic basis
|
|
|
Describe GnRH stimulated release of LH and FSH
|
-GnRH stimulates LH and FSH release when secreted in a pulsatile manner
-GnRH inhibits LH and FSH release if secreted in a continuous manner |
|
|
What is the effect of chronic GnRH secretion on LH and FSH
|
Chronic GnRH secretion downregulates the entire system and turns it into an antagonist rather than an agonist
|
|
|
Describe the uses of chronic GnRH
|
-Used to suppress puberty
-Medical castration -Used to suppress the GnRH axis in some cancer treatments -Not used to stimulate reproduction |
|
|
What occurs if someone is taken off chronic GnRH therapy?
|
-Upregulation of LH and FSH
-Increase in levels of both |
|
|
What occurs with beta-endorphin infusion?
|
Suppression of LH release
|
|
|
What is the effect on infustion of CRH?
|
CRH suppresses LH and stimulates cortisol
|
|
|
What is the effect on infusion of CRH and the opioid antagonist naloxone
|
Naloxone blocks the effect on LH. The combination still stimulates cortisol
|
|
|
How does stress suppress the pituitary-gonadal axis?
|
It does this via a CRH and endogenous opiod dependent mechanism. This happens in both men and women.
|
|
|
Describe stress suppression of the pituitary-gonadal axis in men
|
-Severe stress can lower testosterone levels
-Can occur in extremely sick patients |
|
|
Describe normal LH secretion in males
|
-Secreted in a pulsatile manner
-There is some diurnal variation -Very predictable and nothing changes too much unless something pathological is occuring |
|
|
Describe normal LH secretion in females
|
-You get pulsatile secretion in the beginning
-Then there is a surge, you have estrogen, you have progesterone, you have the whole cycle to deal with. -There are positive and negative feedback effects. -Steroid levels and LH and FSH pulse frequency change dramatically in the woman depending on the stage of the cycle. |
|
|
What genes on the Y chromosome are necessary for testicular development?
|
Testicular determining factors/TDF
|
|
|
What occurs in human development to the primordial gonad in the absence of testicular determining factors?
|
The primordial gonad becomes an ovary
|
|
|
Describe testicular development
|
The testicles develop into Sertoli and Leydig cells
|
|
|
Describe Leydig Cells
|
They make testosterone
|
|
|
Describe the different pathways for testosterone
|
-Testosterone can be 5alpha-reduced to dihydrotestosterone
-Testosterone can be aromatized to give estradiole |
|
|
Describe Sertoli Cells
|
-They make anti-Mullerian homrone, which is necessary to get regression of the Mullerian duct structures (female reproduction structures)
-Ultimately this leads to the formation of the epididymis, vas deferens, and seminal vesicles |
|
|
Describe the production of estrogen
|
Comes from testosterone
|
|
|
Contrast testosterone and dihydroxytestosterone
|
-Both bind to the same receptor
-Both are transported into the nucleus where they bind the same androgen receptor -Due to difference in how they react with other factors and different affinities for the receptor, there are differences in: a. Transcription b. mRNA protein synthesis depending on what the receptor is activated by |
|
|
What structures are normally testosterone dependent structures?
|
-Vas deferens
-Seminal vesicle -Epididymis |
|
|
What structures are normally dihydrotestosterone dependent structures?
|
-Prostate
-Penis -Scrotum |
|
|
Describe what occurs in genitalia develop with 5alpha-reductase deficiency
|
-Very abnormal genitalia develop
-Patients have either female or ambiguous genitalia -Patients have testicles so produce high testosterone during puberty |
|
|
Describe the use of 5alpha reductase inhibitors
|
Used for male pattern baldness and BPH
|
|
|
When does sperm production occur?
|
After puberty
|
|
|
Describe testosterone levels throughout life
|
-Very early in fetal development, in the first or second trimester the male fetus has almost adult levels of androgen
-It goes down and there is another surge shortly after birth -This is suppressed around 6 months and is totally suppressed until puberty -At puberty testosterone levels rise |
|
|
Where does the testosterone come from in the fetus?
|
-Fetal hCG from the placenta acts just like LH
-That is important in stimulating testosterone production from the Leydig cells in the fetus to get the adult testosterone level that is critical for the normal development of external genitalia |
|
|
Describe the pattern of LH secretion in males throughout life
|
-Before puberty you have little gonadotrophin spikes.
-Puberty starts at night. During sleep you get a pulse generator and during the day it goes away until you get the adult pattern. -With stress you can revert back to the midpuberty and prepuberty patterns. This is seen more in girls than boys. |
|
|
Describe the sequence of changes during male puberty
|
-First there is testicular growth with a mean age of 12
-This if followed by growth of the penis -Then there is the pubertal height spurt around age 14 |
|
|
Describe pubic hair growth in males
|
-Mostly the result of testosterone
-In the absence of testosterone, pubic and axillary hair develops as a result of adrenal androgens |
|
|
What compounds are important in the normal growth spurt?
|
Androgens and aromatized estrogen are important for accelerating height.
|
|
|
Describe what occurs with pubic hair in gonadal failure
|
You should expect some axillary pubic hair because there are still adrenal androgens
|
|
|
Describe the significance of no axillary or pubic hair in a male
|
Suggests a problem with both adrenal and gonadal androgens
|
|
|
Describe testicular development
|
1. Testicular enlargement is the first sign of puberty
2. Most of the testicular size is from the development of seminiferous tubules |
|
|
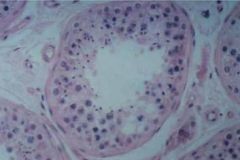
-Histological section of a normal testis
-Mostly semniferous tubules -There are some Leydig cells |
|
|
Describe the testicles when there is a problem with spermatogenesis or seminiferous tubules
|
The testes are small and firm
|
|
|
Describe Spermatogenesis
|
-Dependent on Sertoli cells
-Sperm gradually mature and enter the lumen -During spermatogenesis an androgen binding protein is very important -Intratesticular androgens are important for the development of normal sperm |
|
|
Describe the effects of exogenous testosterone
|
-You will suppress gonadotropins
-You wont have high levels of intratesticular androgen -This suppresses spermatogenesis - |
|
|
If a patient is hypogonadal and wants to undergo spermatogenesis, how do you treat them?
|
-Give them FSH and LH
-FSH is required for normal spermatogenesis -LH is needed to get endogenous testosterone levels up locally to have normal spermatogenesis |
|
|
How long does spermatogenesis take?
|
~90 days
|
|
|
Describe the feedback in the testicular axis
|
-GnRH causes release of FSH and LH
-FSH stimulates spermatogenesis and release of inhibit -Inhibin negatively feeds back to the pituitary -LH leads to testosterone production -Testosterone leads to dihydrotestosterone -Together these lead to virilization -Testosterone negatively feeds back on the pituitary and hypothalamus |
|
|
Where do primary problems occur? Secondary?
|
Primary: Testes
Secondary: Pituitary or hypothalamus |
|
|
Describe primary gonadal failure
|
-Testes wont work
-Androgen levels low -Spermatogenesis low -Gonadotropins elevated* *Hallmark |
|
|
Which testicular cell is more vulnerable: Sertoli or Leydig?
|
Sertoli
|
|
|
What is the likely outcome if someone has light/mild testicular damage
|
-The sertoli cells become damaged and you damage spermatogenesis
-Leydig cells remain fine and testosterone production is normal |
|
|
A patient presents complaining of infertility but is normally virilized. What hormone will be elevated?
|
-The patient has damage to the Sertoli cells, but the Leydig cells are intact.
-There is lack of normal spermatogenesis -No inhibin means that FSH will be elevated |
|
|
How do you treat androgen deficiency?
|
Just give androgens
|
|
|
How do you treat lack of spermatogenesis?
|
Give Gonadotropins
|
|
|
What are the manifestations of testicular failure that only occur if the failure occurs before puberty?
|
-Small testes
-Small penis and prostate -Lack of scrotal rugae and pigmentation -Eunuchoidal skeletal proportions -Delayed bone age -High-pitched voice |
|
|
What are the manifestations of testicular failure in a person who has already completed puberty?
|
-Female fat distribution
-Female escutcheon -Decreased facial and body hair -No temporal hair recession -Decreased muscle mass -Gynecomastia -Decreased libido -Osteoporosis later in life |
|
|
Describe Eunuchoid skeletal proportions
|
Eunuchoid skeletal proportions means long arms and legs. Because of delayed puberty the epiphyses don’t calcify so there is continued growth.
|
|
|
List the genetic/developmental causes of primary hypogonadism
|
-Klinefelter's syndrome
-Androgen Resistance -Enzymatic Defects -Germinal Cell Aplasia |
|
|
List the acquired causes of primary hypogonadism
|
-Infection
-Trauma -Radiation -Chemotherapy |
|
|
List the causes of secondary hypogonadism
|
-Hypothalamic disease
-Pituitary disease -Severe systemic illness |
|
|
What is Geminal cell aplasia
|
Geminal cell aplasia is where you don’t have spermatogenesis but you can normal Leydig cells and androgen secretion.
|
|
|
Describe androgen insensitivity
|
-Patient looks female but is genetically male.
-There is no pubic hair because there is total androgen insensitivity -Androgen levels are high, so estrogen levels are high -Patient is infertile (has testes and Mullerian inhibiting factor) |