![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
152 Cards in this Set
- Front
- Back
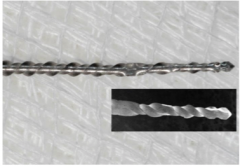
What is wrong with this? |
Lack of uniform flutes on file. Uneven files is a precursor to fracture |
|
|
Essential that you know ( ) of each file before placement |
Length |
|

What is this |
Endo barbed broach: removes vital pulp tissue, cotton pellets, and other debris/material from root canal. |
|
|
What is endo barbed broach NOT used for? |
englarging canal space and should never bind to the canal. |
|
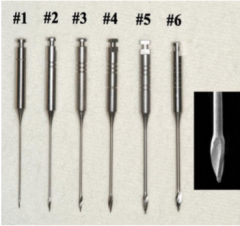
What are these? What are they used for? |
Gates Glidden burs. Used to enlarge the coronal one third to one half of the canal space providing straight line access. Aids in cleaning and shaping. Can't be used beyond first curve. Only #2 and #3 should be used in narrow roots such as mandibular incisors |
|
|
Cutting diameter of Gates glidden drills? |
1: 0.5 2: 0.7 3: 0.9 4: 1.1 5: 1.3 6: 1.5 |
|

|
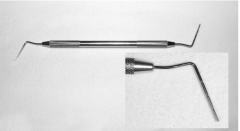
Orifice opener which can be used in place of gates glidden for straight line access. |
|
|
Size of tur-shape orifice opener |
#20 tip and a taper of 0.08. 16 mm shaft. 0.75 MFD and 7 mm fluted length. Used at 300 rpm |
|

|
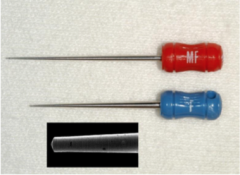
Wave one gold instruments. Alternative approach to cleaning and shaping the canal. |
|
|
Small |
Yellow: 20 tip/7% taper. size 15-20 file. |
|
|
Primary |
Red: 25 tip/ 7% taper. size 20-25 file |
|
|
Medium |
green. 35 tip/6% taper. size 30-35 file |
|
|
Large |
White. 45 tip/5% taper. size 35-40 file |
|
|
Wave one system |
A single use system with an M wire. Prior to using a glide path is established with a size 20 file. |
|
|
What type of rotary motion is a wave one? |
reciprocating. 30 degrees clockwise (disengages instrument), 150 degrees counterclockwise (advances instrument, engaging and cutting dentin. 3 reciprocating cycles complete one rotation. |
|

|
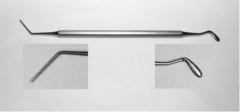
Lentula spiral |
|

|
Luer-Lok syringe with 27 guage needle. Needle should NEVER bind. forcing sodium hypochlorite beyond the apex will cause a sodium hypochlorite accident. ALWAYS know length of needle. Should be bent 1-2 mm short of CWL. |
|
|
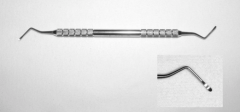
Endo spreaders. lateral compacting of gutta percha and root canal filling materia. |
|

|
Locking cotton pliers |
|
|
Endo spoon excavator |
|
|
Endo 5/7 plugger. used for compaction of gutta percha |
|
|
Glick #1 |
|
|
Measurements for radiographs are rounded to the nearest |
0.5 mm. |
|
|
Teeth longer than ( ) can;t be mounted |
25 mm. |
|
|
Radiographic evaluation of teeth (10) |
tooth length, root curvature, canal curvature, apical canal dilacerations, size of canal space, size of pulp chamber, apical development, calcification, resorption restorations. |
|
|
The images for preop and post op radiographs are made with a... |
straight on paralleling device |
|
|
Maxillary incisors angle |
right angle |
|
|
maxillary canine angle |
Right angle |
|
|
Maxillary premolars angle |
mesial 20 degrees |
|
|
Maxillary molars angle (routine) |
Right angle |
|
|
Maxillary molars angle 4 canals |
Mesial 20 degrees |
|
|
Mandibular incisors angle |
distal 20 degrees |
|
|
Mandibular canine angle |
Mesial 20 degrees |
|
|
Mandibular premolars angle |
Mesial 20 degrees |
|
|
Mandibular molars angle |
Distal 20 degrees |
|
|
What is a second "angled" radiograph used for? |
Beneficial in helping ID the third dimension. |
|
|
Horizontal angulation (mesial or distal) assists in... |
Viewing multiple canals, determining the plane of root curvature |
|
|
Vertical angulation assists in... |
moving anatomical features away from roots, determination of horizontal root fractures. NOTE: can cause foreshortening or over elongation of roots. |
|
|
EDA |
Anterior teeth: Middle of crown to coronal portion of pulp chamber Posterior teeth: Occlusal surface to most coronal aspect of pulp chamber. |
|
|
EDA prevents |
perforation or excessive removal of tooth structure. |
|
|
IF you reach the EDA and haven't found the chamber then... |
Stop and take a parallel radiograph to assess the relationship of your preparation and the pulp space. |
|
|
EWL |
calculated by subtracting 1 mm from the reference point. |
|
|
What does the subtraction of 1 mm for the EWL account for? |
Relation of the actual foramen to the radiographic apex and magnification of the tooth due to the x ray beam. |
|
|
Place the largest file that will go to the CWL and take a radiograph. Round to the nearest 0.5 mm. Continue until 1 mm from the apex is the result. |
|
|
|
When is it permissible to not place a rubber dam? |
If the access is difficult or maintaining longitudinal orientation is a concern. Rubber dam is placed after locating the chamber. |
|
|
What can't be used until rubber dam is placed? |
irrigants such as sodium hypochlorite hand instruments such as broaches and files cannot be used until rubber dam is applied. |
|
|
In cases when pulp is vital, pulp should be removed with... |
spoon excavator, barbed broaches, and files. Never with a bur! |
|
|
Maxillary incisor access opening |
triangular in shape for young individuals due to pulp horns. ovoid in shape for older individuals. |
|
|
Maxillary incisor canal |
1 canal in 100% of cases |
|
|
Maxillary canine access opening |
ovoid in shape bc no pulp horns. DO NOT violate marginal ridges with access preparation. |
|
|
Canal in maxillary canine |
1 canal in 100% of cases. |
|
|
Maxillary premolar access |
ovoid or elliptical. NEVER round |
|
|
Maxillary premolar canals |
two canals (buccal and lingual) constrained in mesial distal direction due to mesial concavity. |
|
|
Maxillary first molar canals |
Three roots with four canals. Mesial concavity at CEJ. |
|
|
Mandibular incisors access |
triangular in shape for young patients, ovoid for old patients |
|
|
Mandibular incisors common perforation site? |
Facial because of facial inclination. |
|
|
Canals? |
Two canals in 25% of cases |
|
|
Mandibular canine access? |
ovoid bc no pulp horns |
|
|
Canals? |
Two canals 30% of time. |
|
|
Mandibular premolars access? |
ovoid/elliptical access opening |
|
|
Canals? |
Single canal: 70%. Two canal: 29%. |
|
|
Mandibular Molar access? |
Rectangular in shape |
|
|
Mandibular molar canals |
two roots with three to four canals present |
|
|
Common perforation in mandibular molars? |
Lingual and Mesial |
|
|
carbide bur mm for flute and shaft |
4 mm for flute and 4 mm for tapering portion of shaft. Serves as a guide during access preparation. |
|
|
Where is the MB2 located in the maxillary molars? |
Under a shelf of the mesial wall and may be 1-3 mm lingual to the main MB canal. |
|
|
Criteria for access openings |
proper outline form, proper location, all coronal pulp tissue removed, no excessive removal of tooth structure, chamber is completely de roofed, all caries have been removed, all canals are located, no perforations. |
|
|
What motion do you use to place the K file? |
twiddling watch winding motion. |
|
|
When to use passive stepback? |
If unable to negotiate file to EWL using a twidding motion. |
|
|
What is passive stepback? |
Removal of dentin coronal to the estimated working length with sequentially larger files at progressively shorter lengths. |
|
|
What does passive stepback do? |
Removes initial coronal interferences of dentin, which creates a glide path for future instrument use and enables use of larger files for the working length radiographic image. |
|
|
When is passive stepback not necessary? |
If canal is large (size 15 file goes to EWL). |
|
|
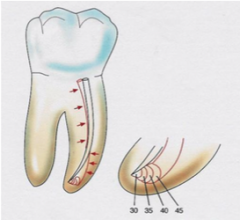
Three curvatures to be aware of? |
Root curvature, canal curvature and apical canal dilaceration |
|
|
Complexities of root curvature |
Slight: 1-30 degrees Moderate: 31-60 degrees Severe: 61-90 degrees S shaped curves |
|
|
Definition of working length file |
The largest file that binds at the estimated working length after passive step back preparation. File must be tight in the canal so it doesn't move during film/image exposure. |
|
|
Working length file must be at least a size.. |
#15. |
|
|
Requirements for proper film? |
Properly angled radiograph, visible radiographic apex, visible tip of the working length file in the apical portion of the tooth. |
|
|
When adjustments are ( ) from the EWL, a new radiograph is not necessary |
0.5 mm |
|
|
Inadequate working length image |
Improperly angled radiograph, radiographic apex not visible, tip of file not visible, tip of working length file not in the apical portion of the tooth (ie 3.5 mm from EWL), file is extended through apex more than 1.0 mm. |
|
|
Straight line access purpose |
To allow files to be placed without binding or deflection through the chamber to the first canal curvature in a curved root or the CWL in straight canals. |
|
|
Gates should never go beyond... |
the first curvature |
|
|
In anterior teeth, when has adequate straight line access been performed? |
When the lingual bulge is removed. |
|
|
If size 35 file binds tightly to CWL, the MAF is... |
size 30. want it to PASSIVELY bind. |
|
|
Once MAF is determined...what is next? |
Passive step back |
|
|
Straight line access criteria |
MAF is no deflected off enamel significantly or off dentin and passes unimpeded to the apical CWL or to the first canal curvature. |
|
|
For canals with an apical stop, MAF <40 what is performed? |
Final apical enlargement with irrigant and smear layer removal followed by dry reaming with the FAF (no irrigant) |
|
|
For canals with an apical stop, MAF> or equal to 40 what is performed? |
Smear layer removal followed by dry reaming with the MAF (no irrigant) |
|
|
For canals that are open or seat you need to... |
create a stop |
|
|
For canals with a seat or open configuration where no stop can be created... |
proceed to smear layer removal (no apical enlargement or dry reaming). |
|
|
When is reaming used? |
passive step back and final apical enlargement. Reaming is a 360 degree hand rotation. |
|
|
Recapitulation definition |
Loosening of dentin chips which collect in the apical portion of the canal. Accomplished with a small file or MAF. Maintains canal patency. Followed by irrigation. |
|
|
Step back preparation definiton |
removal of dentin after MAF determination. Larger files are used in 0.5 increments at decreasing lengths. Until you get to 70. (for canal negotiation prior to MAF determination you do passive step back until you can get a size 15 file) |
|
|
Crown down preparation definition |
Preparation using larger to smaller SS instruments or gradually enlarging the canal with NiTi coronal to apical. technique produces a tapered shape in the coronal to apical orientation. |
|
|
Middle third and apical third preparation can only performed with... |
SS hand files or nickel titanium. |
|
|
Passive step is performed how? |
File must be manipulated around the periphery of the canal in a reciprocating motion. clean the full circumference of the canal by planing with the file laterally in all directions. Enlarge canals only on the pull stroke. |
|
|
How do you know if passive step back is good? |
Know if it resulted in a proper taper if the finger spreader fits loosely or within 1 mm of the CWL. |
|
|
If finger spreader doesn't go to length after passive step back? |
Do passive step back again making sure the larger files go to CWL. |
|
|
IF spreader already fits to WL after MAF determination do you perform passive step back? |
YES to ensure proper cleansing of the walls |
|
|
Procedural errors during instrumentation are primarily caused by... |
Too large file length, excessive force, or by excessive use of small files at length. |
|
|
Nickel titanium instruments use what technique? |
The crown down technique. |
|
|
When can nickel titanium instruments NOT be used? |

S shaped canals, canals with severe dilacerations, where two roots join to form one canal, calcified canals, large canals. |
|
|
How do you use the wave one system |
The files are used in a very PASSIVE, in and out manner only to resistance (2-3 mm increments). Recapitulate between passes. |
|
|
Do not keep the files rotating for more than ( ) seconds in the canal |
3 seconds |
|
|
What file do you recapitulate with? |
Recapitulate to CWL with SS K flex file size 15 0.02 taper after each nickel titanium file insertion to loosen debris. |
|
|
Forcing the nickel titanium instruments places what force on it? |
Torsional which will bind the file and result in separation. |
|
|
Do you remove dentin during recapitulation? |
No you only LOOSEN debris and follow it with irrigation. |
|
|
Canal preparation is smooth when (3) |
1. walls are glassy smooth 2. finger spreader easily fits at or within 1 mm of CWL without binding. 3. The apical configuration is identified. |
|
|
When preparation (cleaning and shaping) is complete and prior to the next step what do you do? (3) |
irrigate and dry with paper points. |
|
|
Cleaning criteria (2) |
1. Glassy smooth walls. 2. No ledges no debris or irrigant in canal |
|
|
Shaping criteria (2) |
1. Adequate spreader penetration 2. Apical configuration identified. |
|
|
After cleaning and shaping, what is the next step?. |
final apical enlargement/apical clearing. |
|
|
Procedural order with stainless steel instruments |
Access opening canal negotiation passive step back length determination straight line access and MAF Cleaning and shaping Step back with SS files recapitulation to corrected WL Apical clearing-when indicated Final apical enlargement smear layer removal (EDTA/NaOCL) dry reaming preparation for obturation obturation. |
|
|
Procedure order: reciprocal wave one instruments |
Access opening canal negotiation passive step back length determination straight line access and MAF Insure there is a glide path with a size 20 SS file. Place wave one file into canal and progress toward resistance-use lubricant-remove file and clean flutes-recapitulate at corrected WL with small SS files-repeat until wave one reaches CWL. Apical clearing-when indicated Final apical enlargement smear layer removal (EDTA/NaOCL) dry reaming preparation for obturation obturation. |
|
|
What method is step back? |
turn pull followed by "peripheral" filling to plane all canal walls |
|
|
Never try to use a rotary instrument which has not first been instrumented by a size ( ) file |
20 |
|
|
What do you use as a lubricant when canals are very small and can't be negotiated |
glycerin |
|
|
What do you use as your reference point in teeth with multiple canals? |
The same cusp tip (MB is usually best for molars, buccal for premolars) |
|
|
Procedural errors in cleaning and shaping |
Loss of working length transportation apical perforations lateral stripping instrument breakage |
|
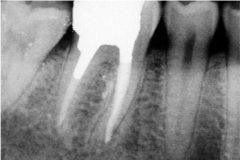
What is this an example of? |
Apical transportation |
|

|
File breakage on MB. loss of working length on ML and D. |
|
|
In molars, size 2 3 and 4 gates are usually used unless.. |
the root is narrow or exhibits a significant concavity. |
|
|
Only the ( ) should be used in narrow roots such as mandibular incisors |
2 and 3. |
|

|
Stripping during straight line access |
|
|
Apical transportation (zip) and perforation-mesial stripping performation |
|
|
Purpose of intracanal medicaments |
Inhibit bacterial growth in root canal thus supporting periapical healing. In immature teeth, create an environment to permit the formation of apical hard tissue matrix against which gutta percha may be condensed. |
|
|
Intracanal medicament used? |
calcium hydroxide |
|
|
When is CaOH indicated |
in teeth with pulp necrosis after an appropriate space is created by performing straight line access and determining MAF. |
|
|
Smear layer removed when? |
prior to placement of CaOH. |
|
|
Smear layer removal steps |
Irrigate with 17% EDTA (1 min) to remove inorganic hydroxyapatite components, followed by 3% NaOCL to remove remaining organic material and dry with paper points. |
|
|
CaOH placement steps |
CaOH powder is mixed with water to form a thick paste. placed with a lentulo spiral on slow speed in forward (which will prevent separation of lenulo and cause paste to flow in not out of canal). Introduce to coronal portion of canal, never stop rotation. Should place until coronal third is packed (should see CaOH visually) |
|
|
When do you know if you have a placed enough CaOH |
when you can see it visually in canal orifice (means coronal 1/3 is adequately packed) |
|
|
Placement of CaOH with syringe (recommended) |
Smear layer removal, prefilled syringes,remove the luer lock and plac ea drop of water in the navi tip and attack to syringe. deliver navi tip staying 2 mm short of CWL. keep delivery LOOSE in canal. Navi tip must never bind when placed in canal. Fill canal until visual. remove excess. temporize with cotton pellet and IRm. |
|
|
When you need to place a temporary restoration, what do you do? |
Seal with a small cotton pellet and IRM or cavit. Place IRM in several increments NOT blob technique. |
|
|
Purpose of temporary coronal restorations |
seal coronally, preventing ingress of oral fluids and bacteria Satisfy esthetic requirements. |
|
|
Indications for temporary coronal restorations |
When RCT is not completed in one visit When RCT is complete but final restoration will be replaced by another dentist. |
|
|
What are the components of IRM? |
Zinc-oxide powder with eugenol |
|
|
When is IRM used? |
Required when one or more marginal ridges are not intact or when extended periods of time between endo appointments exist. STRONG |
|
|
Cavit components? |
Zinc oxide and calcium sulfate |
|
|
When is cavit used? |
When interval between appointments is short and marginal ridges are intact such as access through a gold or porcelain crown. |
|
|
IRM placement technique |
Fluff powder, place one scoop and one drop of liquid on mixing pad. Replace top immediately. Spatulate the powder until smooth and thick. Want it thick enough to form a ball in fingers. If proximal surface is missing, a toffelmire matrix band can be placed. place cotton pellet. |
|
|
When a toffelmire band can't be adapted due to the presence of rubber dam what do you do? |
Place a small cotton pellet and seal the pulp chamber with cavit. Then remove the dam and place IRM. |
|
|
Cavit placement technique |
Squeeze material from tube. No mixing necessary. Place a very small cotton pellet in pulp chamber. Place cavit incrementally and wet with cotton pellet. Moisture required for setting. |
|
|
When little remaining tooth structure exists place... |
glass ionomer for strength |
|
|
When RCT is complete use the ( ) technique |
double seal |
|
|
Double seal technique? |
Remove all remaining provisional materials. 1-2 mm of cavit is placed over obturated canal orifices followed by IRM. No cotton pellet. Place incrementally NOT blob. |
|
|
Definition of apical clearing |
Removes dentin and debris following cleaning and shaping to enlarge the canal at the CWL. |
|
|
Final apical enlargement is performed when..? |
Only if there is an apical stop and a file size less than 40. |
|
|
What is Final apical enlargement? |
Instruments 2-4 sizes larger than MAF are used with irrigant in a reaming action to enlarge the apical portion of the canal at CWL. |
|
|
Last instrument used in final apical enlargement becomes |
FAF |
|
|
If canal has a stop and a file size greater than 40 what do you do? |
Perform dry reaming. |
|
|
FAF definition |
Last file at CWL whether Apical clearing has been performed or not. |
|
|
ljkl |
fdsafds |